Leukopoiesis and Leucoria
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have comprehensive content from the textbooks and excellent images. Let me now deliver the full answer.
Leukopoiesis
Definition
Leukopoiesis is the process of white blood cell (leukocyte) formation. It is one of the three major components of hemopoiesis (hematopoiesis), alongside erythropoiesis (red cell formation) and thrombopoiesis (platelet formation).
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, p. 730-731
Origin and Overview
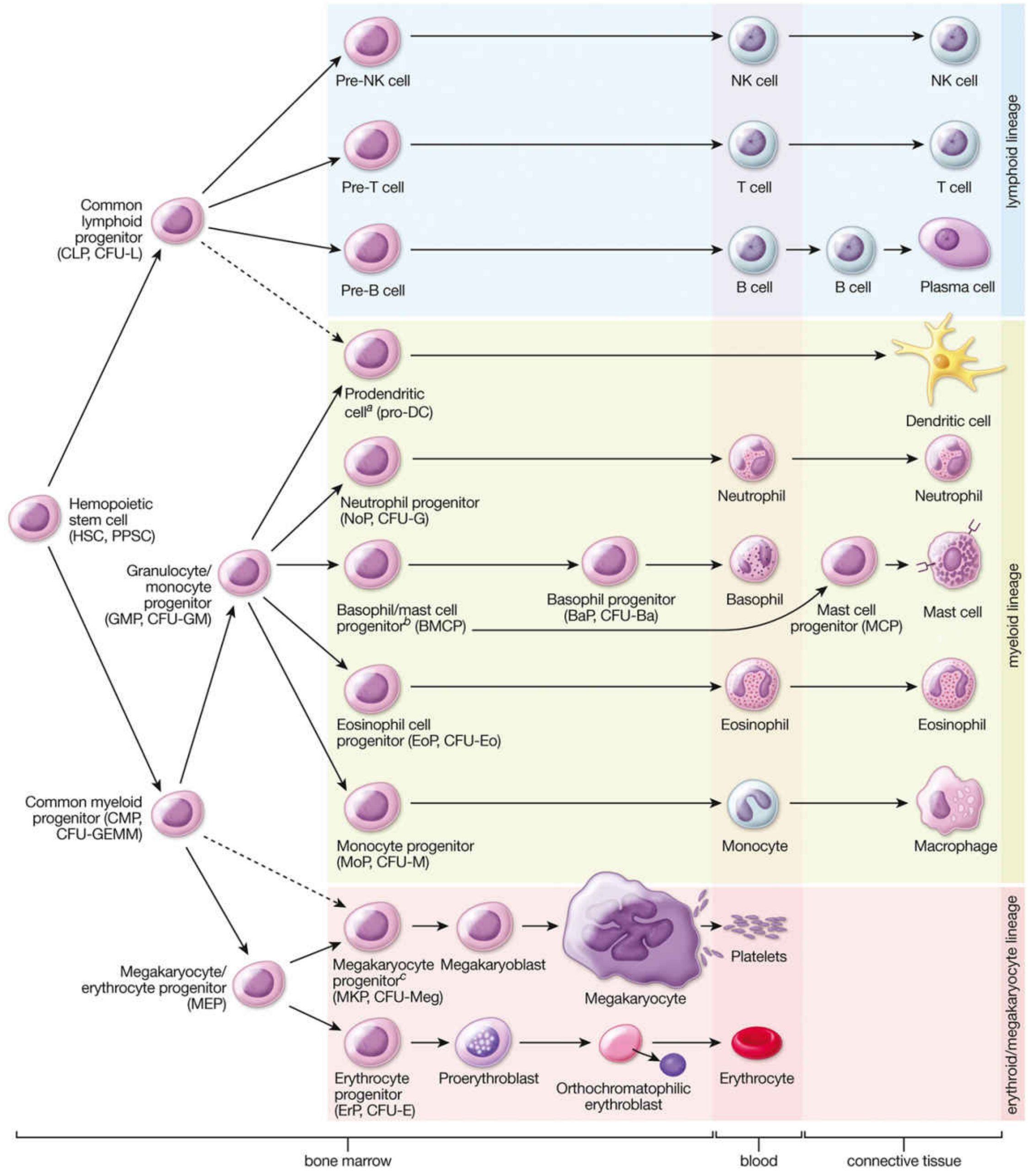
All blood cells arise from hematopoietic stem cells (HSCs) residing in the bone marrow in adults. HSCs are multipotent and differentiate under the influence of cytokines and growth factors into two major progenitor lines:
| Progenitor | Gives rise to |
|---|---|
| Common Myeloid Progenitor (CMP / CFU-GEMM) | Neutrophils, eosinophils, basophils, monocytes, macrophages, dendritic cells, erythrocytes, platelets |
| Common Lymphoid Progenitor (CLP / CFU-L) | T cells, B cells, NK cells, plasma cells |
The hemopoiesis diagram below shows the complete differentiation pathways:
Granulopoiesis (Myeloid White Cells)
Granulocytes (neutrophils, eosinophils, basophils) originate from the CMP, which differentiates into the Granulocyte/Monocyte Progenitor (GMP, CFU-GM).
Neutrophil development passes through six morphologically identifiable stages:
- Myeloblast - earliest recognizable precursor
- Promyelocyte - large cell with primary (azurophilic) granules
- Myelocyte - first stage to exhibit specific (secondary) granules; cell still capable of division
- Metamyelocyte - kidney-shaped nucleus; no longer dividing
- Band (stab) cell - horseshoe-shaped nucleus; immature neutrophil
- Mature neutrophil (segmented) - multilobed nucleus
Eosinophil and basophil development follows a similar maturation pathway from their respective progenitors (EoP and BMCP).
Monopoiesis
Monocytes also arise from the GMP via the monocyte progenitor (MoP, CFU-M). On leaving the bloodstream, monocytes differentiate into tissue macrophages (e.g., Kupffer cells in liver, microglia in CNS, osteoclasts in bone).
Lymphopoiesis
Lymphocytes develop from the CLP and their fate (T vs. B vs. NK) depends on expression of specific transcription factors:
- T cells: mature in the thymus (thymus-dependent)
- B cells: mature in the bone marrow (bursa-equivalent)
- NK cells: develop from pre-NK cell precursors
- Plasma cells: terminal differentiation of activated B cells
Embryonic Leukopoiesis
Blood cell formation is initiated in early embryonic development. Some leukopoiesis occurs in the liver during embryogenesis, though the liver's main role is erythropoiesis in the second trimester fetal period. After birth, the bone marrow becomes the exclusive site for hemopoiesis in adults.
- Histology: A Text and Atlas, p. 731-732
Key Regulators (Cytokines / Growth Factors)
Cytokines act at all stages of leukopoiesis:
- G-CSF (Granulocyte Colony-Stimulating Factor) - promotes neutrophil production
- M-CSF - drives monocyte differentiation
- GM-CSF - stimulates both granulocyte and monocyte lines
- IL-5 - eosinophil maturation and survival
- SCF (stem cell factor) - acts on early HSCs
Clinically: Lithium therapy causes leukocytosis by a direct effect on leukopoiesis. Dopamine receptor antagonists (antipsychotics) can transiently depress leukopoiesis, rarely causing agranulocytosis.
Myeloid:Erythroid (M:E) Ratio
In bone marrow evaluation, the M:E ratio (myeloid to erythroid precursor ratio) is normally ~3:1. A decreased M:E ratio (<1.2:1) indicates either depression of leukopoiesis or erythroid hyperplasia (e.g., hemolytic anemia).
Leukocoria (Leucoria)
Definition
Leukocoria is a white pupillary reflex - the normally red fundal reflex is replaced by a white or yellowish-white glow seen through the pupil.

Note: The right eye shows the characteristic white/yellow reflex instead of the normal dark pupil. This is a red-flag sign requiring urgent ophthalmological evaluation.
- The Wills Eye Manual, Section 8.1
Clinical Importance
Leukocoria in a young child is critically important because it may be the presenting sign of retinoblastoma, a life-threatening intraocular malignancy. Despite routine pediatric screening, leukocoria is frequently first noticed by parents in flash photographs (where one eye shows a white reflection instead of red-eye).
Differential Diagnosis
The following conditions can all present with leukocoria:
| Cause | Key Features |
|---|---|
| Retinoblastoma | Most serious - malignant retinal tumor; mean age 18 months; may be bilateral; iris neovascularization in large tumors |
| Cataract (pediatric) | Lens opacity; may be isolated or associated with systemic disease |
| Persistent Fetal Vasculature (PFV) | Formerly "persistent hyperplastic primary vitreous" (PHPV); failure of regression of fetal hyaloid complex; eye usually smaller (microphthalmos) |
| Retinopathy of Prematurity (ROP) | Previously called retrolental fibroplasia; in premature infants receiving oxygen therapy |
| Coats Disease | Retinal vascular malformation with microaneurysms and macroaneurysms; exudative retinal detachment; almost exclusively males; first decade of life; rarely bilateral |
| Retinal Detachment | Various causes; white reflex from detached retina |
| Toxocariasis | Nematode infection (Toxocara); white elevated granuloma; age 6 months - 10 years; contact with puppies or pica history; serum ELISA positive |
| Familial Exudative Vitreoretinopathy (FEVR) | Hereditary vitreoretinal disorder mimicking ROP |
- Goldman-Cecil Medicine, Table 391-5; The Wills Eye Manual, 8.1
Workup
- Detailed fundoscopy (often under anesthesia / EUA in infants - "examination under anesthesia")
- Ultrasound of the globe - detects calcification (suggests retinoblastoma) and assesses retinal detachment
- MRI of orbit and brain - preferred over CT to avoid radiation; mandatory for bilateral retinoblastoma or family history
- Serum ELISA for Toxocara (positive at 1:8 in the majority of infected patients)
- Systemic pediatric evaluation if retinal astrocytic hamartoma, retinoblastoma, or systemic-disease-associated cataract is suspected
Caution: Anterior chamber paracentesis should be avoided if retinoblastoma is suspected - it risks tumor cell dissemination.
Treatment (by cause)
| Condition | Treatment |
|---|---|
| Retinoblastoma | Chemoreduction, intra-arterial chemotherapy, intravitreal chemotherapy, cryotherapy, thermotherapy, laser photocoagulation, or plaque radiotherapy (in combination). Enucleation for advanced/refractory cases. Systemic chemo for metastatic disease. |
| Toxocariasis | Topical/periocular/systemic steroids; vitrectomy if traction bands; consider laser to visible nematode; albendazole only for systemic disease |
| Coats Disease | FA-guided laser photocoagulation to leaking vessels; intravitreal anti-VEGF agents for posterior involvement; surgical drainage for severe retinal detachment |
| PFV | Cataract removal + retrolental stalk resection ± posterior vitrectomy; amblyopia treatment (visual outcome often poor) |
| Pediatric Cataract | Early cataract extraction, optical correction, amblyopia therapy |
Summary Comparison
| Feature | Leukopoiesis | Leukocoria |
|---|---|---|
| Type | Hematology / Histology | Ophthalmology |
| Meaning | Formation of white blood cells | White pupillary reflex |
| Site | Bone marrow (adults); liver/spleen (fetal) | Eye (pupil) |
| Key concern | Infections, leukemia, drug effects | Retinoblastoma until proven otherwise |
| Most important cause to exclude | Agranulocytosis (drug-induced) | Retinoblastoma |
This is a shared conversation. Sign in to Orris to start your own chat.