I want to prepare my secondary examination for my first class. I want to prepare for-
Asking for Preferences
I want to prepare for my second year examination, which is boy. Which is going to held on... September 1st week. Can you give me a best preparation mode?
Asking for Preferences
Can you give me a notes on diagnosis of... Dengue.
Reading File
Finding Sources
Searching PubMed
dengue fever diagnosis laboratory
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Here are your complete study notes on the diagnosis of Dengue.
Diagnosis of Dengue Fever - Study Notes
Sources: Park's Textbook of Preventive & Social Medicine; Creasy & Resnik's Maternal-Fetal Medicine; Red Book 2021; Goldman-Cecil Medicine
1. The Dengue Virus - Quick Overview
- Causative agent: Dengue virus (DENV), a flavivirus - 4 serotypes (DENV 1-4)
- Vector: Aedes aegypti and Aedes albopictus mosquitoes (daytime biters)
- Incubation period: 3-10 days (commonly 5-6 days)
- Severe dengue is most commonly associated with DENV-2 and secondary infections (a second infection with a different serotype carries higher risk)
2. Clinical Classification of Dengue Infection
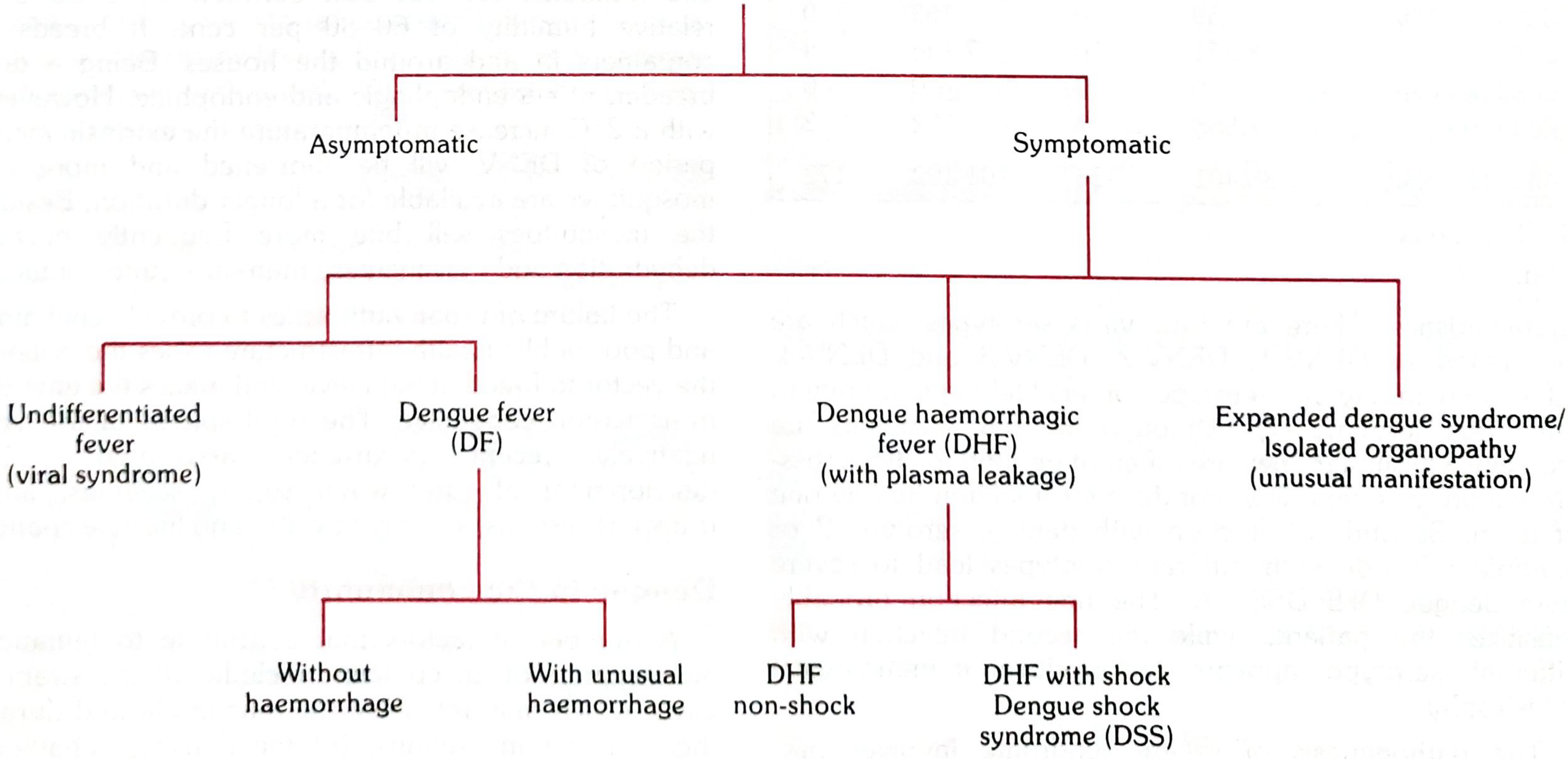
Dengue infection can be:
| Form | Key Features |
|---|---|
| Asymptomatic | No symptoms, common in primary infections |
| Undifferentiated fever | Simple fever + maculopapular rash, indistinguishable from other viral fevers |
| Classical Dengue Fever (DF) | Sudden high fever, headache, myalgia, retro-orbital pain, rash |
| Dengue Haemorrhagic Fever (DHF) | Fever + bleeding + plasma leakage + thrombocytopenia |
| Dengue Shock Syndrome (DSS) | DHF + circulatory failure |
| Expanded dengue syndrome | Unusual organ involvement (hepatitis, encephalitis, myocarditis) |
3. Clinical Phases of Dengue
Phase 1: Febrile Phase
- Sudden onset, high fever (39-40°C), chills
- Intense headache, retro-orbital pain (especially on eye movement or pressure)
- Myalgia, arthralgia ("breakbone fever")
- Photophobia, extreme weakness, anorexia
- Maculopapular rash, flushed face
- Tourniquet test (Rumpel-Leede test) may be positive
Phase 2: Critical Phase (Days 3-7)
- Temperature drops to 37.5-38°C (defervescence)
- Increased capillary permeability → plasma leakage begins
- Rising haematocrit + rapid fall in platelet count
- Warning signs: abdominal pain/tenderness, persistent vomiting, mucosal bleeding, restlessness, liver enlargement >2 cm, oliguria
- Pleural effusion (usually right-sided), ascites
Phase 3: Recovery Phase
- Plasma leakage resolves
- Reabsorption of fluids, risk of fluid overload
- Bradycardia may occur
4. Diagnostic Criteria
Probable Dengue Fever
Fever + two or more of:
- Headache
- Retro-orbital pain
- Myalgia / Arthralgia / Bone pain
- Rash
- Haemorrhagic manifestations
- Leucopenia (WBC ≤ 5,000 cells/mm³)
- Thrombocytopenia (Platelets < 150,000 cells/mm³)
- Rising haematocrit (5-10%)
AND at least one of:
- Supportive serology (HI titre ≥ 1:1280, comparable IgG on ELISA, or positive IgM)
- Occurrence at same location/time as confirmed dengue cases
Confirmed Dengue Fever
Probable case + at least one of:
- Virus isolation from serum, CSF, or autopsy tissue
- Fourfold or greater rise in IgG (by HI test) or rise in IgM to dengue virus
- Antigen detection in tissue/serum/CSF (immunohistochemistry, immunofluorescence, ELISA)
- RT-PCR detection of dengue viral genome
Dengue Haemorrhagic Fever (DHF) - All 4 must be present:
- Acute fever lasting 2-7 days
- Haemorrhagic manifestations (positive tourniquet test, petechiae, ecchymoses, purpura, or bleeding from mucosa/GI tract)
- Platelet count ≤ 100,000 cells/mm³
- Objective evidence of plasma leakage:
- Haematocrit rise ≥ 20% from baseline, OR
- Pleural effusion / ascites / hypoproteinaemia
Dengue Shock Syndrome (DSS)
All DHF criteria + signs of shock:
- Tachycardia, cool extremities, delayed capillary refill, weak pulse
- Pulse pressure ≤ 20 mmHg (e.g., BP 100/80 mmHg)
- Hypotension: systolic BP < 80 mmHg (age < 5 years) or 80-90 mmHg (older children/adults)
5. Laboratory Diagnosis - Detailed
A. Virus Isolation
- Best specimen: Acute-phase serum taken within the first 6 days of illness
- Other specimens: plasma, washed buffy coat, autopsy tissue (liver, spleen, lymph nodes, thymus)
- Gold standard but slow turnaround
B. Viral Nucleic Acid Detection (RT-PCR)
- Detects dengue RNA
- Most useful in early illness (days 1-5) - during viraemia
- Better specificity than simple PCR; faster than virus isolation
- Can serotype the virus
C. Serological Tests
| Test | When Useful | Notes |
|---|---|---|
| IgM capture ELISA (MAC-ELISA) | From day 3-5 of illness | Most practical; IgM appears within days of onset |
| IgG ELISA | Secondary infection / convalescence | Rises rapidly in 2° infection; stays positive for life |
| IgM/IgG ratio | Distinguishes primary vs. secondary | High IgM:IgG = primary; High IgG = secondary |
| Haemagglutination Inhibition (HIA) | Paired sera | ≥4-fold rise confirms diagnosis |
| Complement Fixation (CF) | Research | Less commonly used |
| Neutralization Test (NT) | Reference labs | Most specific; used to confirm serotype |
Important: IgG remains positive for life and is NOT useful for diagnosing new acute infections. Cross-reactivity with other flaviviruses (Zika, West Nile, Japanese encephalitis, yellow fever) can cause false-positive serology. Plaque Reduction Neutralization Test (PRNT) is needed to distinguish dengue from Zika.
D. NS1 Antigen Detection
- Detects dengue nonstructural protein-1 (NS1)
- Can be detected in both primary and secondary infections
- Positive for up to 6 days after illness onset
- Commercial rapid kits available; does not differentiate serotypes
- A key early diagnostic marker
E. Rapid Diagnostic Tests (RDT)
- Detect anti-dengue IgM/IgG antibodies
- Results within 15 minutes
- Accuracy varies; many not fully validated yet
- Used in field/resource-limited settings
F. Haematological Parameters
- Platelet count - falls progressively; < 100,000/mm³ in DHF
- Haematocrit - rises ≥ 20% indicating plasma leakage
- Leucopenia - WBC ≤ 5,000/mm³ is a diagnostic feature
- Monitor daily during critical phase
6. Diagnostic Tests Summary by Timing
| Day of Illness | Best Test |
|---|---|
| Days 1-5 (febrile/viraemic phase) | RT-PCR, NS1 antigen, Virus isolation |
| Day 3+ onwards | IgM (MAC-ELISA) |
| Convalescent / Secondary infection | IgG ELISA, HI test (paired sera) |
7. Tourniquet Test (Rumpel-Leede Sign)
- Inflate BP cuff to midpoint between systolic and diastolic for 5 minutes
- Positive: ≥ 10 petechiae per 2.5 × 2.5 cm (1 inch square)
- In DHF: usually ≥ 20 petechiae (strongly positive)
- Indicates capillary fragility / thrombocytopenia
8. Differential Diagnosis
Dengue should be distinguished from:
- Other arboviral fevers (Chikungunya, Zika, West Nile)
- Malaria
- Leptospirosis
- Typhoid fever
- Viral hepatitis
- Meningococcemia
9. Key Points to Remember for Exam
- NS1 antigen = best early marker (days 1-6)
- RT-PCR = best for confirmation in first 5 days
- IgM (MAC-ELISA) = appears from day 3-5, stays positive for weeks
- IgG = not useful for acute diagnosis (stays positive for life)
- Tourniquet test is the most common haemorrhagic sign in dengue
- Platelet ≤ 100,000 + haematocrit rise ≥ 20% = hallmarks of DHF
- Cross-reactivity with Zika and other flaviviruses is a major pitfall of serology
- Reference testing for dengue is available through the CDC dengue branch
Recent Evidence (2025): A systematic review (PMID: 41037858) published in Journal of Infection and Public Health (2025) provides updated coverage of dengue pathogenesis, diagnosis, and management - consistent with the clinical framework above.
Sources: Park's Textbook of Preventive & Social Medicine, pp. 291-293 | Creasy & Resnik's Maternal-Fetal Medicine | Red Book 2021 (AAP) | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.