Pulse
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a complete clinical overview of the Pulse:
The Pulse - Clinical Overview
Physiology
Blood ejected into the aorta with each cardiac cycle creates a pressure wave. Critically, this wave travels at 3-5 m/sec, while blood itself flows at only ~0.5 m/sec. So when you palpate a peripheral pulse, you are feeling a pressure wave, not blood flow itself. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
The character and contour of the arterial pulse depend on four main factors:
- Stroke volume
- Ejection velocity
- Vascular compliance
- Systemic vascular resistance
(Harrison's Principles of Internal Medicine, 22e)
What to Assess
Six key parameters are evaluated on every pulse examination (S Das, Manual on Clinical Surgery):
| Parameter | What it reflects |
|---|---|
| Rate | Fast (tachycardia) or slow (bradycardia) |
| Rhythm | Regular or irregular |
| Tension / Force | Diastolic and systolic blood pressure |
| Volume | Pulse pressure |
| Character | Underlying cardiac/vascular pathology |
| Arterial wall condition | e.g., atherosclerotic thickening |
Normal pulse rate in adults: 60-100 bpm. Count for a full minute if irregularity is present; in a regular rhythm, count for 15 seconds and multiply by 4.
Pulse Pressure
Pulse pressure = Systolic BP - Diastolic BP (normal ~40 mmHg)
- Widened pulse pressure (≥60 mmHg): anemia, exercise, hyperthyroidism, aortic regurgitation (AR), AV fistula, patent ductus arteriosus, increased intracranial pressure
- Narrowed pulse pressure (≤20 mmHg): hypovolemia, aortic stenosis, pericardial tamponade, early septic shock (increased peripheral vascular resistance), reduced stroke volume
Pulse Characters and Their Causes
The carotid artery is the best site to assess pulse character. Below are the key abnormal pulse types, illustrated by the waveform diagram from Harrison's:
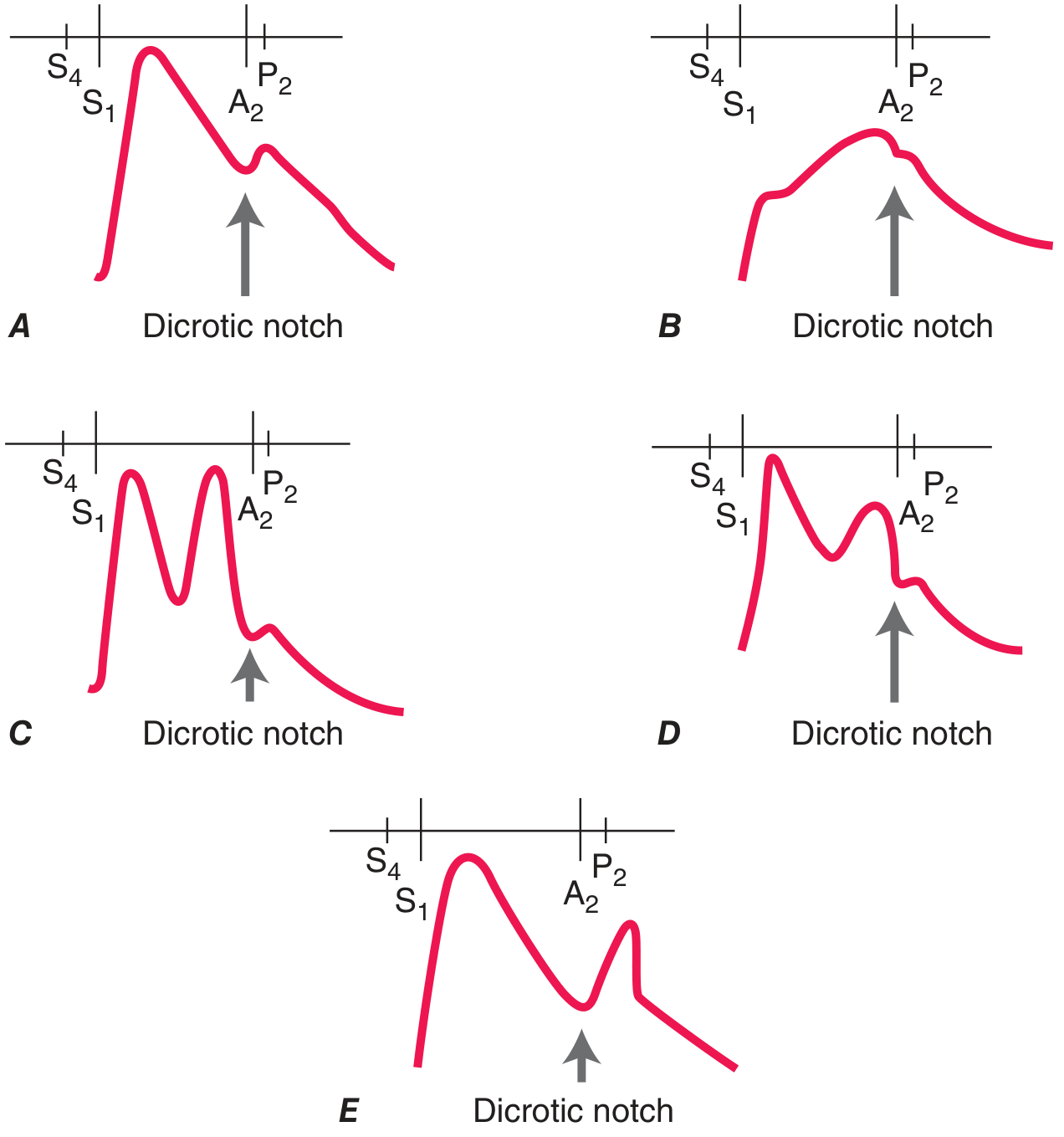
| Pulse Type | Character | Cause |
|---|---|---|
| Pulsus parvus et tardus | Weak, small, delayed upstroke | Severe aortic stenosis (AS) |
| Anacrotic pulse | Slow, notched upstroke | Severe AS |
| Corrigan's / Water-hammer pulse | Sharp rise, rapid fall | Chronic severe aortic regurgitation (AR), thyrotoxicosis |
| Bisferiens pulse | Two systolic peaks | Severe AR, HOCM |
| Dicrotic pulse | Two peaks - one systolic, one diastolic | Sepsis, intraaortic balloon pump |
| Pulsus paradoxus | Systolic BP falls >10 mmHg on inspiration | Pericardial tamponade, massive PE, severe COPD, tension pneumothorax |
| Pulsus alternans | Beat-to-beat variation in pulse amplitude | Severe LV systolic dysfunction |
Pulsus Paradoxus - Measurement
Detected by sphygmomanometer:
- Inflate cuff, deflate slowly
- Note the pressure at which Korotkoff sounds are first heard (expiration only)
- Note the pressure at which sounds are heard throughout the cycle
- A difference >10 mmHg = pulsus paradoxus
- It is palpable at brachial/femoral when the pressure difference exceeds 15 mmHg
- Harrison's Principles of Internal Medicine, 22e
Palpation Sites
Pulses are routinely examined at:
- Radial (most common for rate/rhythm)
- Carotid (best for character - palpate below thyroid cartilage to avoid carotid sinus massage)
- Brachial (best for amplitude/contour)
- Femoral, Popliteal, Posterior tibial, Dorsalis pedis (peripheral vascular assessment)
Caution: Never palpate both carotid arteries simultaneously - this can compromise cerebral blood flow. Auscultate for a bruit before vigorous carotid palpation.
Clinical Significance
-
Absent radial pulse in trauma = strongly suggests hypotension
-
Absence of both radial and femoral pulses = significant predictor of hypotension in hypovolemic shock
-
Reduction in pulse pressure is an early indicator of reduced central blood volume, even before systolic BP drops
-
In patients with nonpulsatile LVADs (HeartMate II/III, HVAD, etc.), pulses may be absent despite adequate perfusion - assess skin warmth and capillary refill instead
-
Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.