wagner classification with images in a single slide like image
Wagner classification diabetic foot ulcer grades 0-5 clinical images diagram
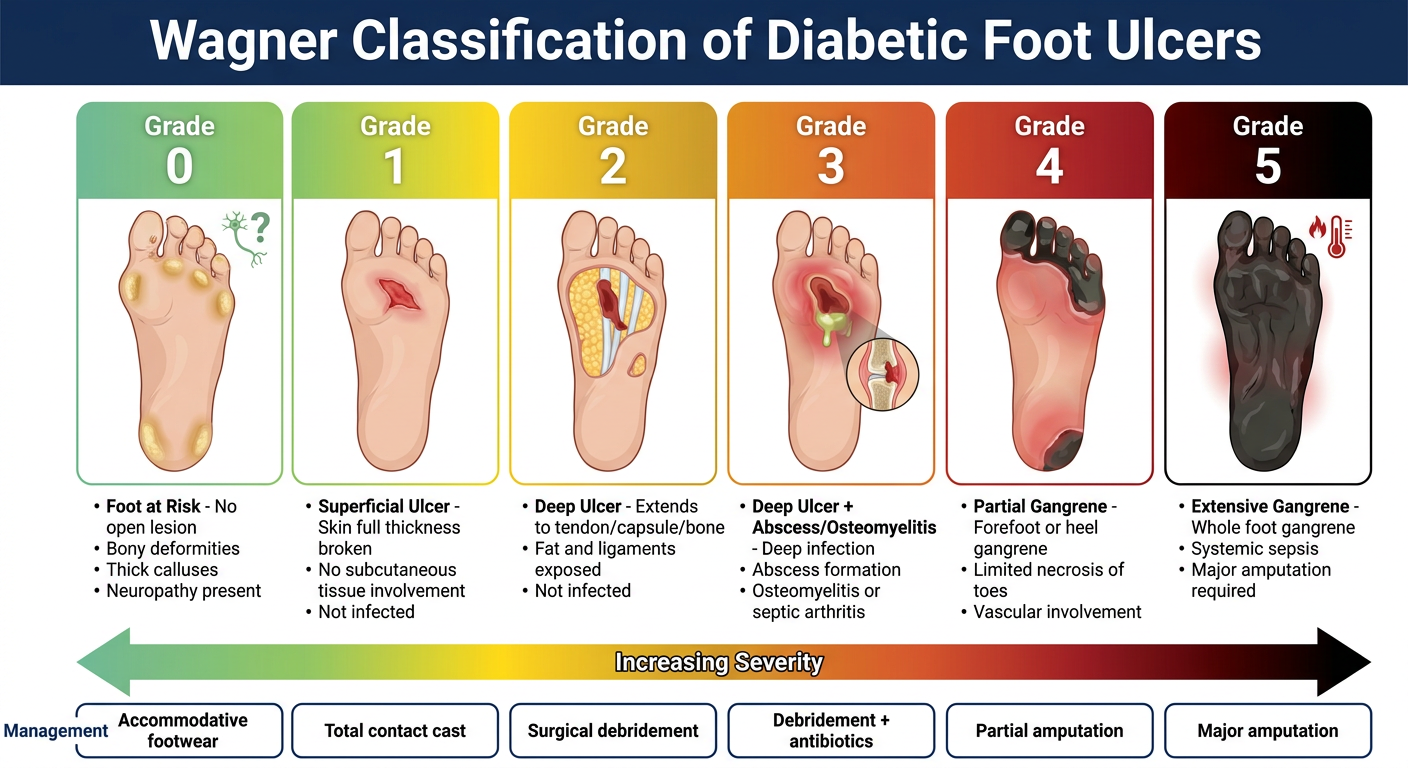
A clean medical education single slide showing the Wagner Classification of Diabetic Foot Ulcers. The slide has a dark navy blue header bar with white bold title text "Wagner Classification of Diabetic Foot Ulcers". Below the header, there are 6 grade boxes arranged horizontally in a single row, each with a distinct color gradient from green (Grade 0) progressing through yellow, orange, to deep red (Grade 5), representing severity. Each grade box contains: the grade number in large bold font at the top, a simple clean clinical illustration or icon of the foot showing the lesion depth/extent, and 3-4 bullet points of key features below. Grade 0 (green): "Foot at Risk - No open lesion, Bony deformities, Thick calluses, Neuropathy present". Grade 1 (yellow-green): "Superficial Ulcer - Skin full thickness broken, No subcutaneous tissue involvement, Not infected". Grade 2 (yellow): "Deep Ulcer - Extends to tendon/capsule/bone, Fat and ligaments exposed, Not infected". Grade 3 (orange): "Deep Ulcer + Abscess/Osteomyelitis - Deep infection, Abscess formation, Osteomyelitis or septic arthritis". Grade 4 (red-orange): "Partial Gangrene - Forefoot or heel gangrene, Limited necrosis of toes, Vascular involvement". Grade 5 (deep red/black): "Extensive Gangrene - Whole foot gangrene, Systemic sepsis, Major amputation required". At the bottom of the slide, a color-coded severity arrow spans left to right labeled 'Increasing Severity' with 'Management' row showing: Grade 0=Accommodative footwear; Grade 1=Total contact cast; Grade 2=Surgical debridement; Grade 3=Debridement + antibiotics; Grade 4=Partial amputation; Grade 5=Major amputation. Clean white background, professional medical style, high contrast.

Wagner Classification of Diabetic Foot Ulcers - Summary
| Grade | Description | Key Features | Management |
|---|---|---|---|
| 0 | Foot at Risk | No open lesion; bony deformities, thick calluses, neuropathy | Accommodative footwear, serial exams, patient education |
| 1 | Superficial Ulcer | Full-thickness skin break; no subcutaneous involvement; not infected | Office debridement, total contact cast |
| 2 | Deep Ulcer | Extends to tendon, joint capsule, or bone; fat/ligaments exposed; not infected | Surgical debridement, off-loading, culture-specific antibiotics |
| 3 | Deep Ulcer + Osteomyelitis | Deep infection with abscess, osteomyelitis, or septic arthritis | Surgical debridement or partial amputation, IV antibiotics |
| 4 | Partial Gangrene | Forefoot or heel gangrene; limited necrosis of toes/foot | Vascular reconstruction + partial foot amputation |
| 5 | Extensive Gangrene | Whole-foot gangrene; systemic effects | Major extremity amputation |
- Grades 0-3 progress by depth of tissue involvement
- Grades 4-5 progress by extent of gangrene (partial vs. whole foot)
- Grade 3 is the critical cutoff - osteomyelitis changes management dramatically (IV antibiotics, bone resection)
- Grades 4 and 5 mandate amputation; extent is determined by vascular status
Target glycemic coontrol in image
target glycemic control HbA1c fasting postprandial goals ADA 2024 guidelines table
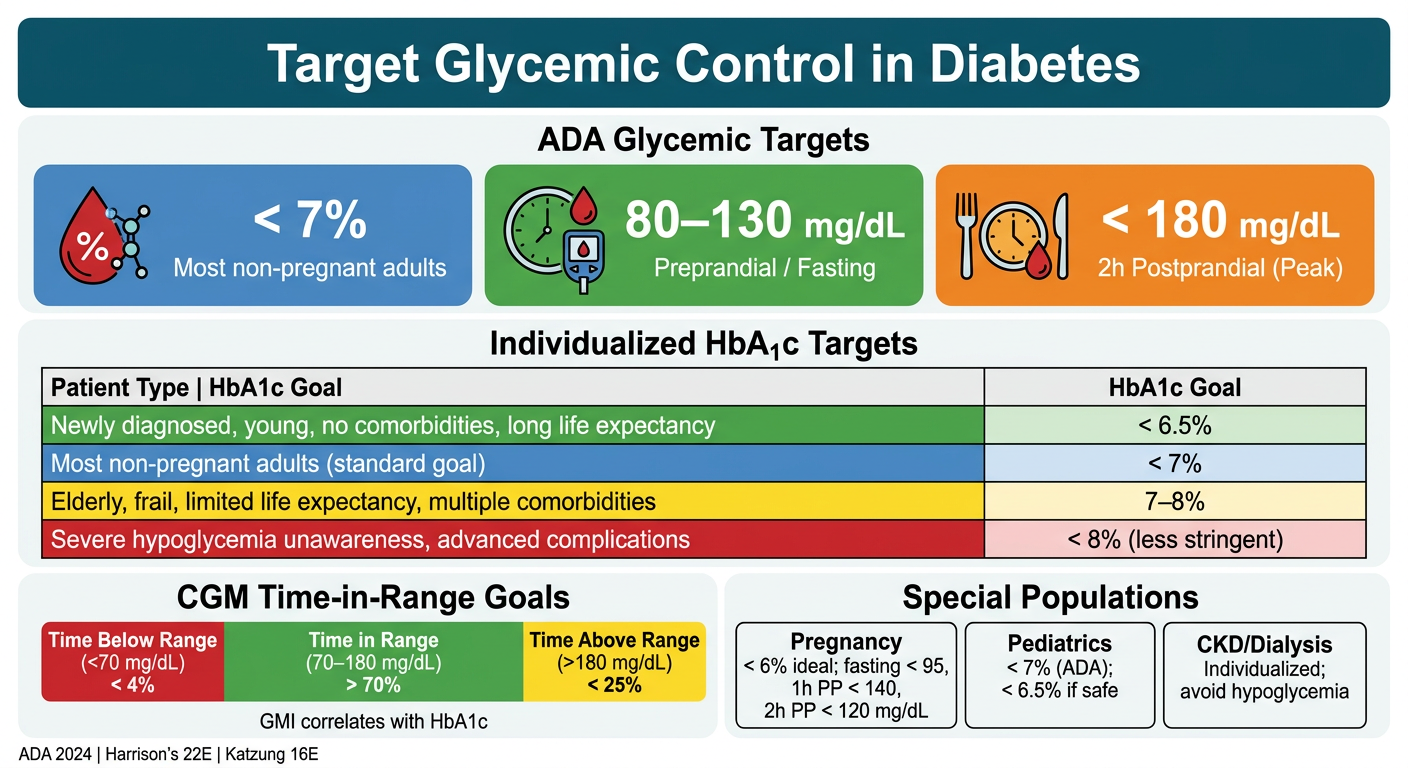
A clean professional medical education single-slide infographic titled "Target Glycemic Control in Diabetes" with a dark teal header bar and white bold title text. The slide is divided into clear sections: TOP SECTION - "ADA Glycemic Targets" with 3 large colored metric boxes in a row: - Box 1 (blue): HbA1c icon, large text "< 7%", subtext "Most non-pregnant adults" - Box 2 (green): fasting glucose icon, large text "80–130 mg/dL", subtext "Preprandial / Fasting" - Box 3 (orange): postprandial icon, large text "< 180 mg/dL", subtext "2h Postprandial (Peak)" MIDDLE SECTION - "Individualized HbA1c Targets" table with 4 rows: - Row header: Patient Type | HbA1c Goal - Row 1 (green): "Newly diagnosed, young, no comorbidities, long life expectancy" | "< 6.5%" - Row 2 (blue): "Most non-pregnant adults (standard goal)" | "< 7%" - Row 3 (yellow): "Elderly, frail, limited life expectancy, multiple comorbidities" | "7–8%" - Row 4 (red): "Severe hypoglycemia unawareness, advanced complications" | "< 8% (less stringent)" BOTTOM SECTION - Two panels side by side: Left panel "CGM Time-in-Range Goals" with a horizontal color bar showing: Time Below Range (<70 mg/dL) < 4% in red | Time in Range (70–180 mg/dL) > 70% in green | Time Above Range (>180 mg/dL) < 25% in yellow. Below: "GMI correlates with HbA1c" Right panel "Special Populations" with 3 mini boxes: - Pregnancy: "< 6% ideal; fasting < 95, 1h PP < 140, 2h PP < 120 mg/dL" - Pediatrics: "< 7% (ADA); < 6.5% if safe" - CKD/Dialysis: "Individualized; avoid hypoglycemia" Footer note: "ADA 2024 | Harrison's 22E | Katzung 16E" in small text. Clean white background, modern flat design, high contrast colors, professional medical style.
Target Glycemic Control - Key Values
| Parameter | Target |
|---|---|
| HbA1c | < 7% (53 mmol/mol) |
| Fasting / Pre-meal glucose | 80-130 mg/dL (4.4-7.2 mmol/L) |
| Peak post-meal glucose (2h) | < 180 mg/dL (10 mmol/L) |
| Patient Type | HbA1c Target |
|---|---|
| Young, newly diagnosed, long life expectancy | < 6.5% |
| Standard - most adults | < 7% |
| Elderly, frail, multiple comorbidities | 7-8% |
| Severe hypoglycemia unawareness / advanced disease | < 8% (less stringent) |
- Time in range (70-180 mg/dL): > 70%
- Time below range (< 70 mg/dL): < 4% (< 1% below 54 mg/dL)
- Time above range (> 180 mg/dL): < 25%
- Pregnancy: Fasting < 95, 1h PP < 140, 2h PP < 120 mg/dL; HbA1c < 6%
- Children/Adolescents: HbA1c < 7% (< 6.5% if achievable without hypoglycemia risk)
- CKD/Dialysis: Individualized; HbA1c may be unreliable - use fructosamine or CGM
What is time in range ?
Time in Range (TIR)
How It's Measured
- TIR - % time glucose is within target
- Time Above Range (TAR) - % time glucose is too high
- Time Below Range (TBR) - % time glucose is too low
- GMI (Glucose Management Indicator) - correlates with HbA1c
- Glucose variability
Target Ranges and Goals
| Zone | Glucose Range | Target |
|---|---|---|
| Time in Range (TIR) | 70-180 mg/dL (3.9-10 mmol/L) | > 70% |
| Time Below Range (TBR) | < 70 mg/dL | < 4% |
| Time Very Low | < 54 mg/dL | < 1% |
| Time Above Range (TAR) | > 180 mg/dL | < 25% |
70% TIR = approximately 16.8 hours/day in range
Why TIR Matters - vs HbA1c
| Feature | HbA1c | TIR |
|---|---|---|
| Reflects | Average glucose over 2-3 months | Daily glucose fluctuation in real time |
| Captures hypoglycemia | No | Yes |
| Captures glucose variability | No | Yes |
| Affected by anemia/hemoglobinopathy | Yes | No |
| Actionable same day | No | Yes |
Special Population TIR Targets
| Population | TIR Target | Range |
|---|---|---|
| Most adults with T1/T2 DM | > 70% | 70-180 mg/dL |
| Pregnancy | > 70% | 63-140 mg/dL (tighter range) |
| Elderly / High hypoglycemia risk | > 50% | 70-180 mg/dL |