SLE
Reading File
Finding Sources
Searching PubMed
"systemic lupus erythematosus"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"lupus erythematosus" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Systemic Lupus Erythematosus (SLE):
Systemic Lupus Erythematosus (SLE)
Definition & Epidemiology
SLE is a chronic autoimmune disease in which overactive innate and adaptive immune responses cause tissue damage through autoantibodies and immune complex deposition. Multiple organ systems are affected, with cutaneous, musculoskeletal, and renal systems most prominently involved, followed by pulmonary, hematologic, cardiovascular, serosal, and central nervous system involvement.
- Prevalence (US): ~204,295 cases (CDC National Lupus Registry)
- Sex: ~90% female, predominantly childbearing age; female:male ratio is approximately 9:1 overall
- Race: Highest prevalence in Black women, followed by Hispanic, White, and Asian/Pacific Islander women
- 5-year survival: ~90% after diagnosis
- Genetics: Strong familial tendency; association with MHC genes DR2, DR3, DR4, DR5; deficiencies in complement (C1q, C2, C4) are risk factors
- Harrison's Principles of Internal Medicine 22E (2025), p. 2871
Pathogenesis
SLE reflects multiple immunoregulatory defects. Key mechanisms include:
- Autoantibody production - especially to nuclear antigens (anti-dsDNA, anti-Sm, ANA)
- Impaired clearance of apoptotic material (dead cells release nuclear debris that triggers immune activation)
- Type I interferon pathway dysregulation - excess IFN-α amplifies B and T cell activation
- Complement activation - immune complex deposition activates complement, causing tissue inflammation and vasculitis
- B and T cell abnormalities - loss of tolerance, excessive B cell activation, defective T regulatory cells
Environmental triggers include UV radiation (sunlight), infections, stress, and certain drugs.
Classification Criteria
ACR 11-Criterion System (≥4 required for diagnosis)
| # | Criterion | Detail |
|---|---|---|
| 1 | Malar rash | Fixed erythema over malar eminences, sparing nasolabial folds |
| 2 | Discoid rash | Erythematous raised plaques with keratotic scaling; may scar |
| 3 | Photosensitivity | Unusual skin reaction to sunlight |
| 4 | Oral ulcers | Usually painless; nasal/nasopharyngeal |
| 5 | Arthritis | Non-erosive, ≥2 peripheral joints |
| 6 | Serositis | Pleuritis or pericarditis |
| 7 | Renal disorder | Proteinuria >0.5 g/day OR cellular casts |
| 8 | Neurologic disorder | Seizures or psychosis (no other cause) |
| 9 | Hematologic disorder | Hemolytic anemia, leukopenia (<4000), lymphopenia (<1500), or thrombocytopenia (<100,000) |
| 10 | Immunologic disorder | Anti-dsDNA, anti-Sm, or antiphospholipid antibodies |
| 11 | Antinuclear antibody (ANA) | Abnormal titer by immunofluorescence |
The 2019 EULAR/ACR criteria require a positive ANA (≥1:80) as an entry criterion, then assign weighted points across clinical domains (≥10 points needed). These are classification criteria for clinical trials, not strict diagnostic criteria.
- Goldman-Cecil Medicine; Textbook of Family Medicine 9e
Clinical Features
1. Mucocutaneous (>90% of patients eventually affected)
- Malar/butterfly rash - in ~1/3 of patients; often precipitated by sun exposure
- Subacute cutaneous LE (SCLE) - annular or papulosquamous lesions on sun-exposed areas; associated with anti-Ro (70%); does NOT scar
- Discoid LE (DLE) - raised erythematous plaques with scaling; can scar with hypopigmented atrophic centers
- Alopecia - reversible in acute flare; permanent if due to discoid scarring
- Oral/nasal ulcers, photosensitivity, Raynaud phenomenon
2. Musculoskeletal
- Arthritis/arthralgia in ~90% - non-erosive (distinguishes from RA)
- Myositis, avascular necrosis (especially with steroid use)
3. Renal (Lupus Nephritis) - major determinant of prognosis
- Clinical renal disease in 15-75%; histologic evidence in most biopsy specimens
- WHO/ISN-RPS Classification:
- Class I: Minimal mesangial - no treatment needed
- Class II: Mesangial proliferative - no targeted renal therapy needed
- Class III: Focal proliferative - aggressive therapy for active/necrotizing lesions
- Class IV: Diffuse proliferative - always requires vigorous therapy
- Class V: Membranous - therapy varies by severity
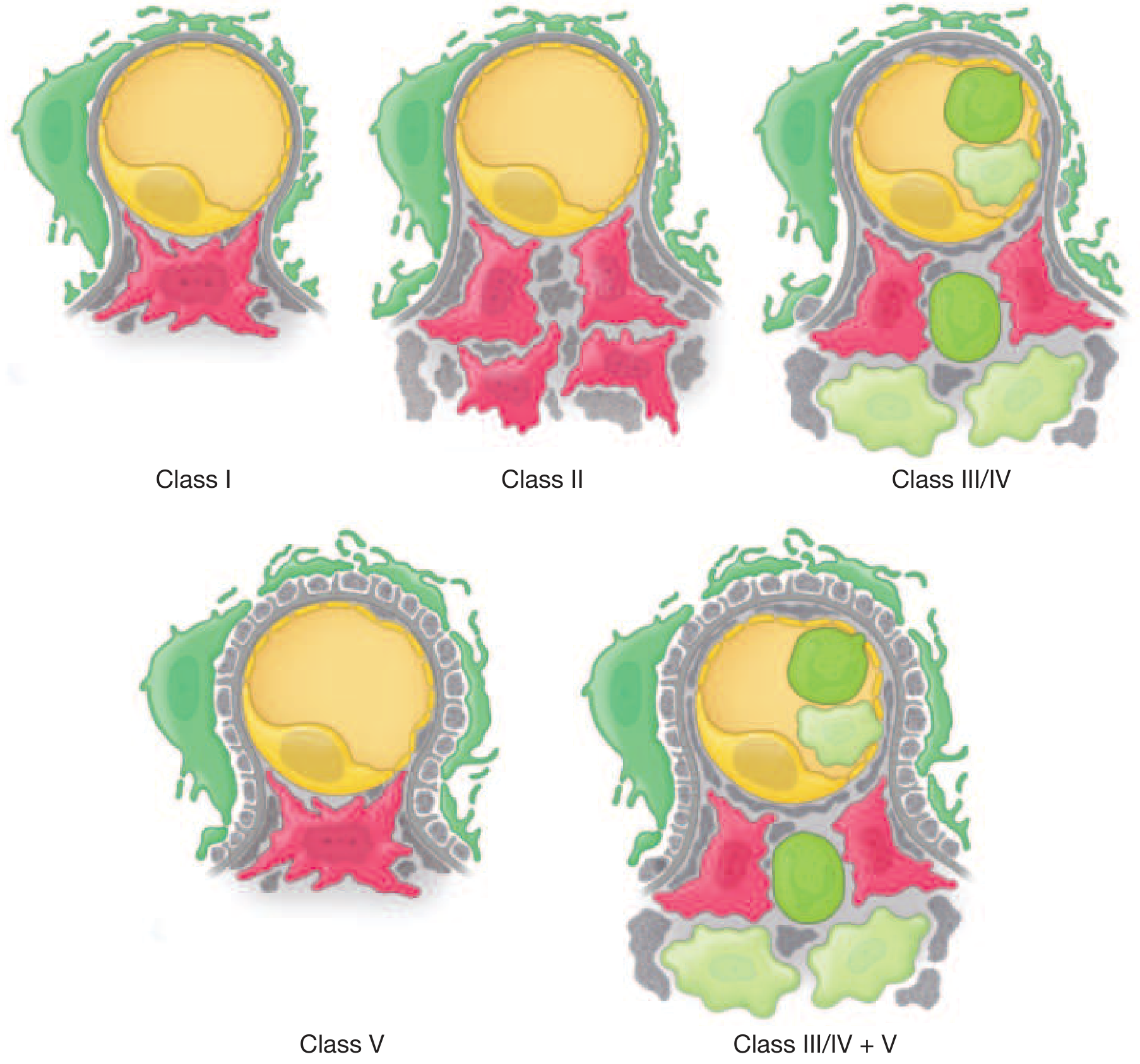
FIGURE: Ultrastructural features of lupus glomerulonephritis (Harrison's 22E, 2025)
4. Neuropsychiatric (NPSLE)
- Seizures, psychosis, stroke, cognitive dysfunction, peripheral neuropathy
- Depression and anxiety are common (may overlap with "type 2 lupus" symptoms)
5. Hematologic
- Anemia of chronic disease (most common), autoimmune hemolytic anemia, aplastic anemia
- Leukopenia (<4000/µL) in ~50%, mostly lymphopenia
- Thrombocytopenia - immune-mediated; may be severe (<50,000)
- Antiphospholipid syndrome (APS) - thrombosis, recurrent pregnancy loss
6. Cardiovascular
- Pericarditis (most common cardiac manifestation), myocarditis, Libman-Sacks endocarditis
- Accelerated atherosclerosis - major long-term cause of morbidity/mortality
7. Pulmonary
- Pleuritis/pleural effusion, lupus pneumonitis, pulmonary hypertension, shrinking lung syndrome
8. Gastrointestinal
- Nausea/vomiting, mesenteric vasculitis (can cause intestinal perforation), lupus peritonitis, elevated liver enzymes
9. Ocular
- Keratoconjunctivitis sicca, retinal vasculitis (rare but can cause blindness), uveitis, optic neuritis
Key Autoantibodies
| Antibody | Sensitivity | Specificity | Clinical Association |
|---|---|---|---|
| ANA | ~95% | Low | Screening test |
| Anti-dsDNA | ~70% | High | Correlates with disease activity, nephritis |
| Anti-Sm | ~25% | Very high (specific for SLE) | -- |
| Anti-Ro (SS-A) | ~30-40% | -- | Photosensitivity, SCLE, neonatal lupus |
| Anti-La (SS-B) | ~15% | -- | Often with anti-Ro |
| Anti-histone | ~70% | Low | Drug-induced lupus |
| Antiphospholipid | ~30% | -- | Thrombosis, recurrent miscarriage |
Treatment
General Principles
- Avoidance of triggers: Sun protection (all patients), avoid sulfonamides, procainamide, hydralazine
- All patients should be assessed for organ involvement at diagnosis and during flares
Drug Therapy by Indication
| Setting | Treatment |
|---|---|
| All patients | Hydroxychloroquine (HCQ) 400 mg/day (reduces flares, end-organ damage, thrombosis risk, mortality) |
| Cutaneous disease | Topical corticosteroids first-line; HCQ for persistent lesions |
| Arthritis/serositis/myositis | NSAIDs first-line; prednisone 0.5-1 mg/kg/day for refractory cases |
| Moderate systemic disease | Low-dose glucocorticoids + HCQ ± methotrexate, azathioprine |
| Severe disease (nephritis class III/IV, cerebritis, myocarditis) | High-dose glucocorticoids + cyclophosphamide OR mycophenolate mofetil (MMF) |
| Lupus nephritis (all classes) | HCQ (6.5 mg/kg ideal weight/day) - reduces risk of end-stage renal disease |
| Class III/IV nephritis induction | Methylprednisolone pulse + MMF OR cyclophosphamide (Euro-Lupus or NIH protocol) |
| Maintenance | MMF or azathioprine |
| Refractory/biologic therapy | Belimumab (anti-BLyS), anifrolumab (anti-IFN receptor), voclosporin (for nephritis) |
Recent evidence (EULAR 2023 update - PMID 38777375): The 2023 EULAR recommendations update reinforces treat-to-target strategies, minimizing glucocorticoid use, and expanding indications for biologics including anifrolumab.
Emerging (PMID 39754644): CAR-T cell therapy has shown early efficacy in refractory autoimmune diseases including SLE, representing a potential future treatment option.
Monitoring
- CBC, urinalysis, anti-dsDNA, complement (C3/C4) levels to assess disease activity
- Annual ophthalmologic exam for HCQ retinal toxicity (risk increases with >5 years use, >5 mg/kg/day)
Special Situations
- Drug-induced lupus: Procainamide, hydralazine, isoniazid, quinidine, phenytoin (ACLE); hydrochlorothiazide, CCBs, TNF antagonists (SCLE). Anti-histone antibodies are hallmark. Usually resolves with drug discontinuation.
- Neonatal lupus: Caused by transplacental passage of maternal anti-Ro/anti-La antibodies. Can cause congenital heart block.
- Pregnancy: SLE increases risk of preeclampsia, fetal loss, preterm birth. Disease should be in remission for ≥6 months before conception. HCQ should be continued; cyclophosphamide is contraindicated.
- Type 1 vs Type 2 lupus: Type 1 = inflammatory/immune (responds to immunosuppression); Type 2 = fatigue, pain, cognitive dysfunction (less immunosuppression-responsive).
Prognosis
- Bimodal mortality pattern: Early deaths from infection and active disease; late deaths from cardiovascular disease and damage accrual
- 5-year survival ~90%; 20-year survival significantly lower due to long-term complications
- Worse prognosis: Black/Hispanic race, male sex, early onset, lupus nephritis, neuropsychiatric involvement, APS, low socioeconomic status
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine International Edition; Textbook of Family Medicine 9e; Comprehensive Clinical Nephrology 7e; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.