Pyelolithotomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
pyelolithotomy kidney stone surgery
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the content needed for a thorough answer. Here it is:
Pyelolithotomy
Pyelolithotomy is a surgical procedure in which the renal pelvis is incised (pyelotomy) to remove renal calculi directly, without cutting into the renal parenchyma. It is one of the oldest approaches to renal stone disease and historically was a preferred alternative to nephrolithotomy because it avoided renal parenchymal incision and the associated hemorrhagic morbidity.
Historical Background
The operation evolved over centuries. Heinecke in 1879 first described a pyelotomy incision for calculus extraction. The technique was refined by Josef Hyrtl (1882) and Max Brödel (1902), who identified the relatively avascular plane near the midline of the convex border of the kidney. A landmark advance was the Gil-Vernet intrasinusally extended pyelolithotomy (1965), which allowed wide access to the collecting system with minimal morbidity, making it the dominant open surgical approach for renal calculi through the 1970s. Lower (1913) had previously revived interest in pyelolithotomy, noting it was safer and simpler than nephrolithotomy, though some series suggested a higher incidence of retained stone fragments with pyelolithotomy alone.
- Campbell Walsh Wein Urology, p. 254-257
Current Indications
Modern endourology (PCNL, ureteroscopy, ESWL) has largely supplanted open surgery for most renal stones. As stated in Harrison's Principles of Internal Medicine 22e, "advances in urologic approaches and instruments have nearly eliminated the need for open surgical procedures such as ureterolithotomy or pyelolithotomy."
Pyelolithotomy (open or laparoscopic/robotic) is now reserved for:
-
Complex stones with anatomical abnormalities (e.g., horseshoe kidney, ectopic kidney, pelviureteric junction obstruction [UPJO])
-
Infected staghorn calculi not accessible by PCNL
-
Concomitant reconstructive procedures (e.g., pyeloplasty for UPJO with calculi)
-
Patients with prior failed endourological attempts
-
The procedure cannot be performed if the patient has an intrarenal pelvis (the pelvis must be extrarenal to allow safe incision)
-
Bailey and Love's Short Practice of Surgery 28e, p. 4232
-
Hinman's Atlas of Urologic Surgery, p. 221
Preoperative Preparation
- Urine culture - treat any infection prior to surgery
- Axial imaging (CT urogram) - define stone burden, collecting system anatomy
- Basic labs - renal function, coagulation
- Patient positioned in the flank position
- A flank incision is made below the 11th or 12th rib depending on kidney position
Operative Technique
Step 1 - Exposure
Gerota's fascia is opened in a cranial-caudal direction. Perinephric fat is dissected off the kidney carefully, avoiding the subscapular plane. The proximal ureter is identified and dissected proximally to the renal pelvis.
Key anatomical caution: The posterior segmental artery crosses just inside the posterior renal sinus - avoid injuring it during dissection.
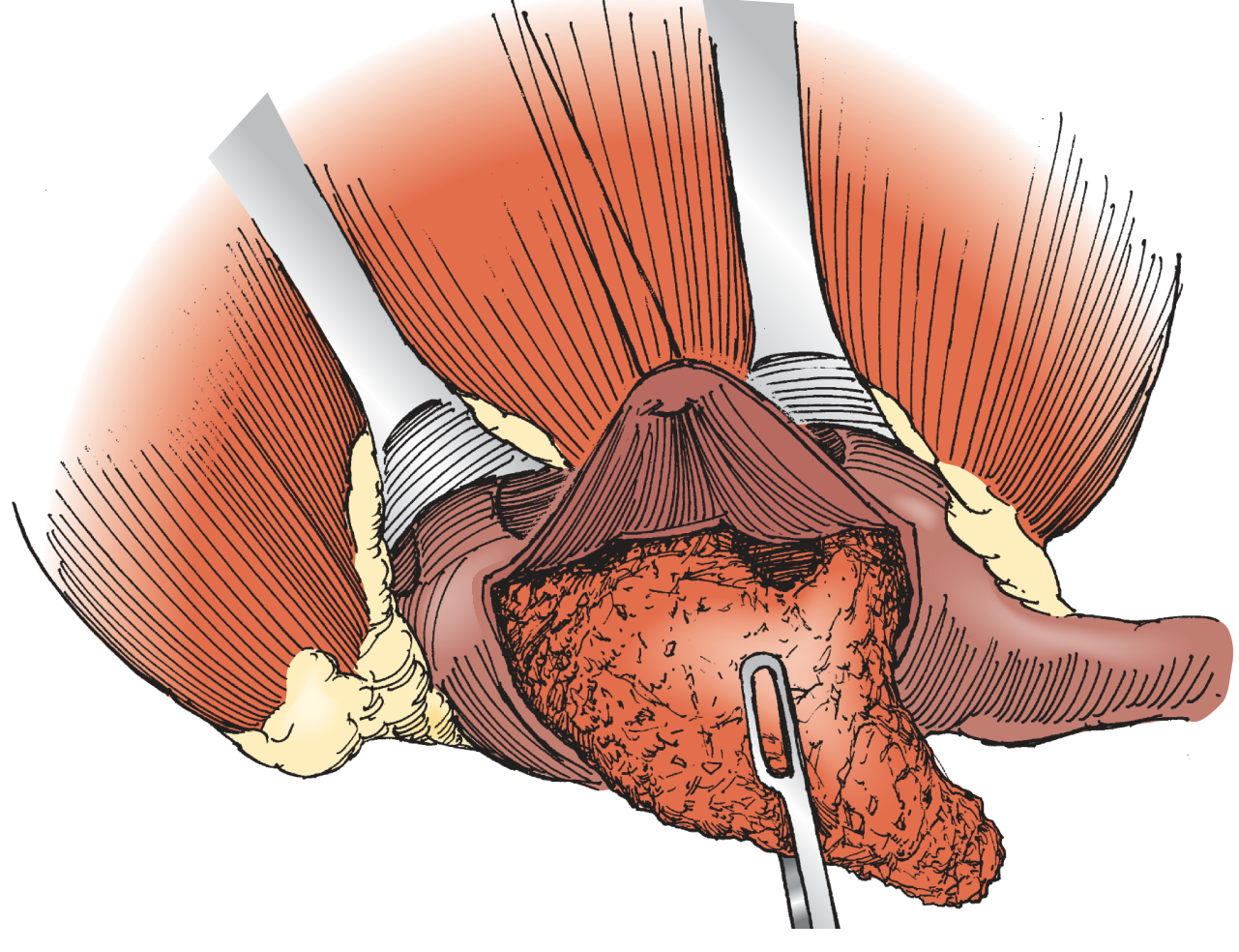
Step 2 - Pyelotomy Incision
A U-shaped incision is made in the renal pelvis over the stone using a hooked 12-blade scalpel or Potts scissors. The apex of the incision must be placed at least 1 cm away from the ureteropelvic junction to avoid UPJ stenosis.

If multiple small stones are present, an 8-French feeding tube is passed down the ureter to prevent stone migration distally.
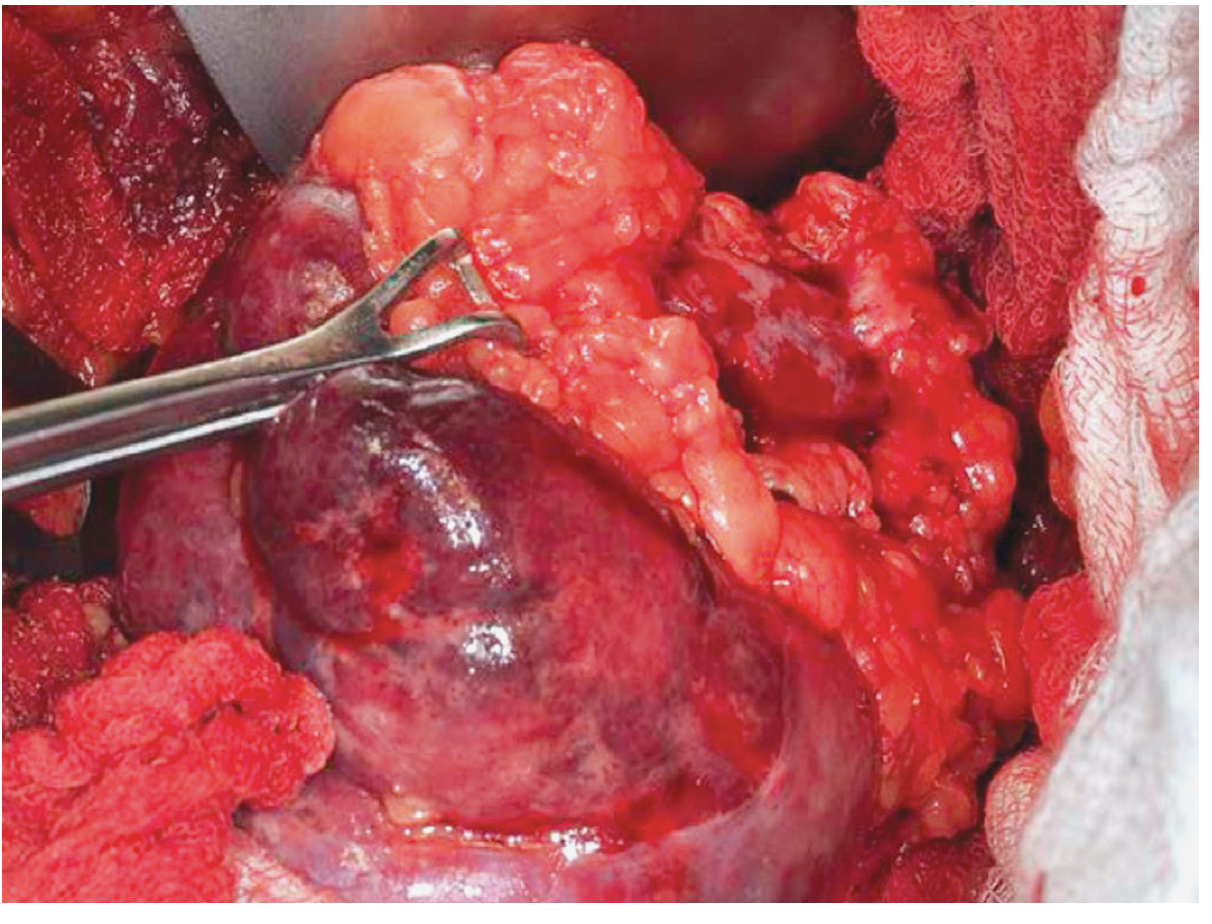
Step 3 - Stone Extraction
The U-shaped ureteral flap is retracted to expose the stone. A blunt Randall forceps is used to gently grasp and extract the stone.
Extended Pyelolithotomy
If stone ramifications extend into a calyx making complete removal difficult through the pyelotomy alone:
- The pyelotomy incision is extended superiorly into the respective infundibulum
- The renal parenchyma is reflected away to expose the calyceal stone
- If a calyceal stone still cannot be retrieved through the infundibulum: locate it by palpation, push it toward the capsule, sharply incise the capsule circumferentially, and bluntly dissect the parenchyma using a Penfield dissector
- Extract via blunt Randall forceps through the resulting nephrotomy
- Close the nephrotomy with horizontal mattress 3-0 polyglactin sutures over a fat bolster
- If parenchymal incision is required and clamping will be prolonged: temporary renal artery bulldog clamp + cold ischemia + IV mannitol
Coagulum Technique
A useful adjunct for multiple small stones or when preventing stone migration during manipulation:
- Two bags of thawed cryoprecipitate (~30 mL total, stained with methylene blue) are prepared
- The ureter is occluded with a wrapped Penrose drain
- Residual urine is aspirated from the pelvis via Angiocath
- 1 mL of 10% calcium chloride is mixed into the cryoprecipitate immediately before injection
- The mixture is injected to fill (not overfill) the renal pelvis
- After 5 minutes, the pelvis is opened with a U-shaped incision and the intact coagulum (with entrapped stones) is carefully extracted
- The pelvis and ureter are then thoroughly irrigated
Closure
- A nephroscope (flexible cystoscope or ureteroscope) is used to inspect all calyces for residual fragments
- An antegrade double-J stent is placed for urinary drainage
- The renal pelvis is closed with a running 5-0 polyglactin suture
- Gerota's fascia is re-approximated with 2-0 polyglactin sutures
- A Jackson-Pratt drain is placed posterior to the kidney through a separate stab incision
- Standard fascial and skin closure
Postoperative Care and Complications
Postoperative care is similar to anatrophic nephrolithotomy, but pyelolithotomy carries significantly less risk of bleeding or transfusion since no parenchymal incision is required for straightforward cases. Acute tubular necrosis rates are also lower because renal blood flow is not interrupted.
| Complication | Notes |
|---|---|
| Urinary leak | Drain output monitored; usually resolves with stent in place |
| Residual stone | Persistent infection signals retained fragments; treat with antibiotics + secondary PCNL/retrograde URS (wait ≥6 weeks) |
| UPJ obstruction | Rare late complication if incision is too close to UPJ |
| Hemorrhage | Less common than after nephrolithotomy |
| ATN | Rare unless prolonged ischemia required |
Laparoscopic and Robotic Pyelolithotomy
Minimally invasive approaches are now available and well-described:
-
Laparoscopic pyeloplasty + concomitant pyelolithotomy: In a series by Ramakumar et al. (2002), 20 cases with UPJO + calculi were managed laparoscopically; 90% stone-free rate at 3 months, using laparoscopic graspers and a flexible cystoscope through a 10-12 mm port.
-
Robotic-assisted pyeloplasty + pyelolithotomy: Demonstrated in 8 patients by Atug et al. (2005), with one robotic arm temporarily undocked to facilitate stone extraction. Overall stone-free rate 80%.
-
A 2024 systematic review and meta-analysis on robotic pyelolithotomy (Wang et al., PMID 39120845) confirms its efficacy for large renal stone disease.
-
Laparoscopic pyelolithotomy is also listed among "miscellaneous" minimally invasive urological procedures for complex indications. - Smith and Tanagho's General Urology 19e
-
Campbell Walsh Wein Urology, p. 2611
Summary
| Feature | Detail |
|---|---|
| Definition | Incision of renal pelvis to remove calculi |
| Access | Flank incision (below 11th/12th rib) |
| Incision | U-shaped pyelotomy, apex ≥1 cm from UPJ |
| Contraindication | Intrarenal pelvis |
| Key instrument | Blunt Randall forceps |
| Adjunct | Coagulum technique for multiple stones |
| Drainage | Double-J stent + Jackson-Pratt drain |
| Current role | Reserved for complex stones, anatomical anomalies, concomitant reconstruction |
| Advantage over nephrolithotomy | Less bleeding, no ATN risk (no vascular clamping needed for standard cases) |
Primary sources: Hinman's Atlas of Urologic Surgery; Campbell Walsh Wein Urology 3-Volume Set; Bailey and Love's Short Practice of Surgery 28e; Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.