Treatment of supracondylar humerus fracture in children
Reading File
Finding Sources
Searching PubMed
"supracondylar humerus fracture" AND children AND treatment
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have substantial content from three authoritative sources. Let me compile a comprehensive answer.
Supracondylar Humerus Fracture in Children
Overview
Supracondylar humerus fractures are the most common elbow fractures in children and the most common fracture requiring surgery by pediatric orthopedic surgeons. The peak incidence is at age 5-7 years. The vast majority (95-98%) are extension-type (posterior displacement of the distal fragment), caused by a fall on an outstretched hand with the elbow in hyperextension. Flexion-type fractures are rare (<5%) and occur from a direct blow to the posterior elbow.
- Rosen's Emergency Medicine, p. 3305
- Campbell's Operative Orthopaedics 15th Ed 2026
- Bailey and Love's Short Practice of Surgery 28th Ed, p. 462
Gartland Classification (Extension-Type)
| Type | Description |
|---|---|
| I | Non-displaced fracture |
| II | Displaced with intact posterior cortex |
| IIA | No rotational deformity |
| IIB | With rotational deformity |
| III | Displaced with NO cortical contact |
| IIIA | Posteromedial rotation of distal fragment |
| IIIB | Posterolateral rotation of distal fragment |
- Rosen's Emergency Medicine, Table 170.3
Initial Assessment - Neurovascular Examination (MANDATORY)
Before any treatment, a complete neurovascular exam is required. The elbow is in close proximity to the brachial artery and three major nerves:
- Anterior interosseous nerve (AIN) - branch of median nerve, most commonly injured in extension fractures (posterolateral displacement)
- Radial nerve - injured with posteromedial displacement
- Ulnar nerve - injured with flexion-type fractures; also at risk during medial pin placement
- Brachial artery - at risk with displaced fractures
Signs of vascular compromise: the 5 Ps - Pain, Pallor, Pulselessness, Paralysis, Paresthesias. Worsening pain or pain with passive finger extension is a warning sign of compartment syndrome and Volkmann ischemic contracture.
Imaging
- AP and lateral elbow X-rays are standard
- Look for fat pad signs: an anterior fat pad "sail sign" or posterior fat pad elevation indicates hemarthrosis and occult fracture even when bone displacement is not obvious
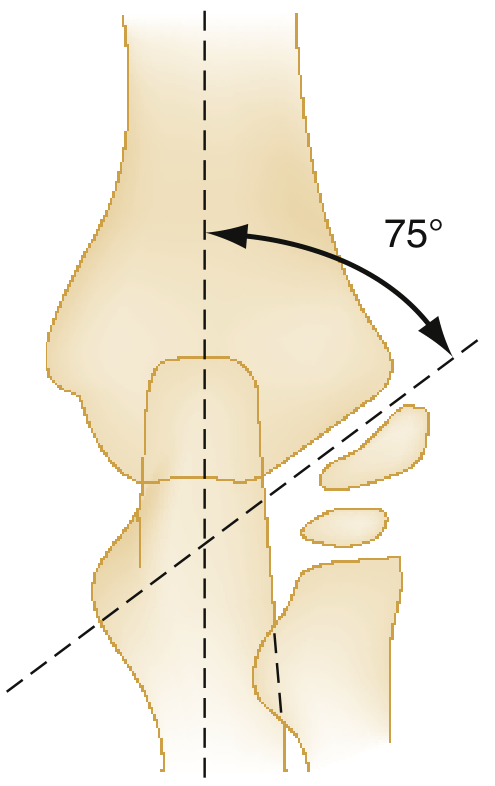
- The Baumann angle (normal ~70-75° on AP view) and the anterior humeral line (on lateral view, should pass through the middle third of the capitellum) are used to assess fracture alignment and reduction adequacy
The CRITOE mnemonic helps interpret ossification centers around the elbow:
| Center | Appears |
|---|---|
| Capitellum | 6-12 months |
| Radial head | 4-5 years |
| Internal (medial) epicondyle | 5-7 years |
| Trochlea | 8-10 years |
| Olecranon | 8-9 years |
| External (lateral) epicondyle | 9-13 years |
Treatment by Gartland Type
Type I - Non-displaced
- Posterior long-arm splint with elbow at 90° flexion, forearm in neutral or pronated position
- Immobilize for 3 weeks
- Follow-up with orthopedics within 24 hours for evaluation and casting
- Progressive mobilization after union
Type II - Displaced with intact posterior cortex
- Closed reduction is performed
- If reduction can be maintained with <90° of elbow flexion: above-elbow cast for 3-4 weeks
- If >90° flexion is required to hold reduction: percutaneous K-wire (Kirschner wire) fixation + above-elbow cast - deep flexion risks vascular compromise, especially with significant swelling
Type III - Completely displaced (no cortical contact)
- Admission and operative treatment
- Standard of care: Closed Reduction and Percutaneous Pinning (CRPP) under general anesthesia with fluoroscopic guidance
- If closed reduction fails: open reduction and internal fixation (ORIF)
Surgical Technique: Closed Reduction and Percutaneous Pinning (CRPP)
Reduction maneuver:
- Apply steady inline traction with forearm in neutral ("thumb-up" position) to restore length
- Correct medial/lateral displacement by pushing the fragment in the appropriate direction
- Place thumb over the anterior surface of the proximal fragment with fingers behind the olecranon and gently flex the elbow
- Immobilize with forearm pronated (for laterally displaced fractures) or supinated (for medially displaced fractures)
Pin configuration:
- Two lateral divergent pins - reduces ulnar nerve injury risk; most commonly used
- Cross-pin configuration (one lateral + one medial) - provides greater torsional stability but risks ulnar nerve injury if medial pin is placed without direct visualization of the nerve
Pins are typically removed at 3-4 weeks and active range of motion begins.
Special Situations: Vascular Injuries
White pulseless hand:
- Surgical emergency
- Requires immediate reduction to attempt to restore blood flow
- If pulse does not return after reduction: urgent vascular exploration by a vascular-trained surgeon
Pink pulseless hand (perfused but no radial pulse):
-
More controversial management
-
If there is satisfactory limb perfusion, no compartment syndrome, and no neurological injury: perform fracture reduction and stabilization with an expectant approach to the vascular injury
-
Pulse often returns within 24-48 hours as swelling resolves
-
Serial vascular monitoring is mandatory
-
Bailey and Love's, p. 462
Complications
| Complication | Notes |
|---|---|
| Volkmann ischemic contracture | Rare but devastating; from missed compartment syndrome due to excessive swelling, often from placing elbow in deep flexion |
| Cubitus varus ("gunstock deformity") | Most common long-term complication; due to malunion in varus; cosmetically deforming but rarely functionally significant. Requires corrective supracondylar osteotomy if severe |
| Cubitus valgus | Less common; risk of delayed ulnar nerve palsy |
| Neurological injury | Most are neuropraxia; resolve after reduction and swelling resolution |
| Pin-tract infection | Managed with pin removal at appropriate time |
| Elbow stiffness | Usually resolves with time and physiotherapy |
Key Surgical Timing Points
- Fractures with neurovascular compromise require emergency surgery
- For stable fractures with intact vasculature, surgery within 12-24 hours is acceptable and does not increase complication rates compared to immediate fixation
- Overnight observation with repeat neurovascular checks is appropriate for closed fractures with no vascular compromise
Recent Evidence (2023-2026)
A 2026 network meta-analysis (PMID 41076056) on biomechanical optimization of pediatric supracondylar humerus fracture fixation examined different pin configurations and supports that lateral-only pinning with appropriately placed divergent pins provides sufficient stability while minimizing ulnar nerve risk - consistent with current clinical practice guidelines.
Summary treatment algorithm:
-
Type I → Splint/cast, 3 weeks
-
Type II, stable → Closed reduction + cast
-
Type II, unstable / Type III → CRPP (gold standard)
-
Vascular compromise → Emergency reduction ± vascular exploration
-
Failed closed reduction → Open reduction
-
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, Rosen's Emergency Medicine, Bailey and Love's Short Practice of Surgery 28th Ed
This is a shared conversation. Sign in to Orris to start your own chat.