Tsh metabolism in newborns.
Reading File
Finding Sources
Finding Sources
Searching PubMed
TSH metabolism newborn thyroid function
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from two authoritative textbooks plus key diagrams. Here is the full answer:
TSH Metabolism in Newborns
1. Fetal Thyroid Development and the HPT Axis
The thyroid gland forms at the base of the tongue from endodermal cells as early as week 3 of gestation and descends to the pretracheal position by weeks 5-7. The hypothalamic-pituitary-thyroid (HPT) axis matures progressively:
| Milestone | Gestational Age |
|---|---|
| TRH detectable in fetal CNS | ~5 weeks |
| Thyroid descent to neck | ~7 weeks |
| TRH in hypothalamus; TSH in pituitary/serum | ~10-14 weeks |
| Fetal thyroid functional (iodide trapping, T4 synthesis) | ~12 weeks |
| Hypothalamic-portal system active; fetal TSH and T4 begin rising | ~18-20 weeks |
| Fetal T3 becomes significant | ~30 weeks onward |
Before ~16 weeks, the fetus is entirely dependent on maternal thyroid hormone (T4). Maternal TRH does not significantly cross the placenta, and TSH does not cross the placenta at all.
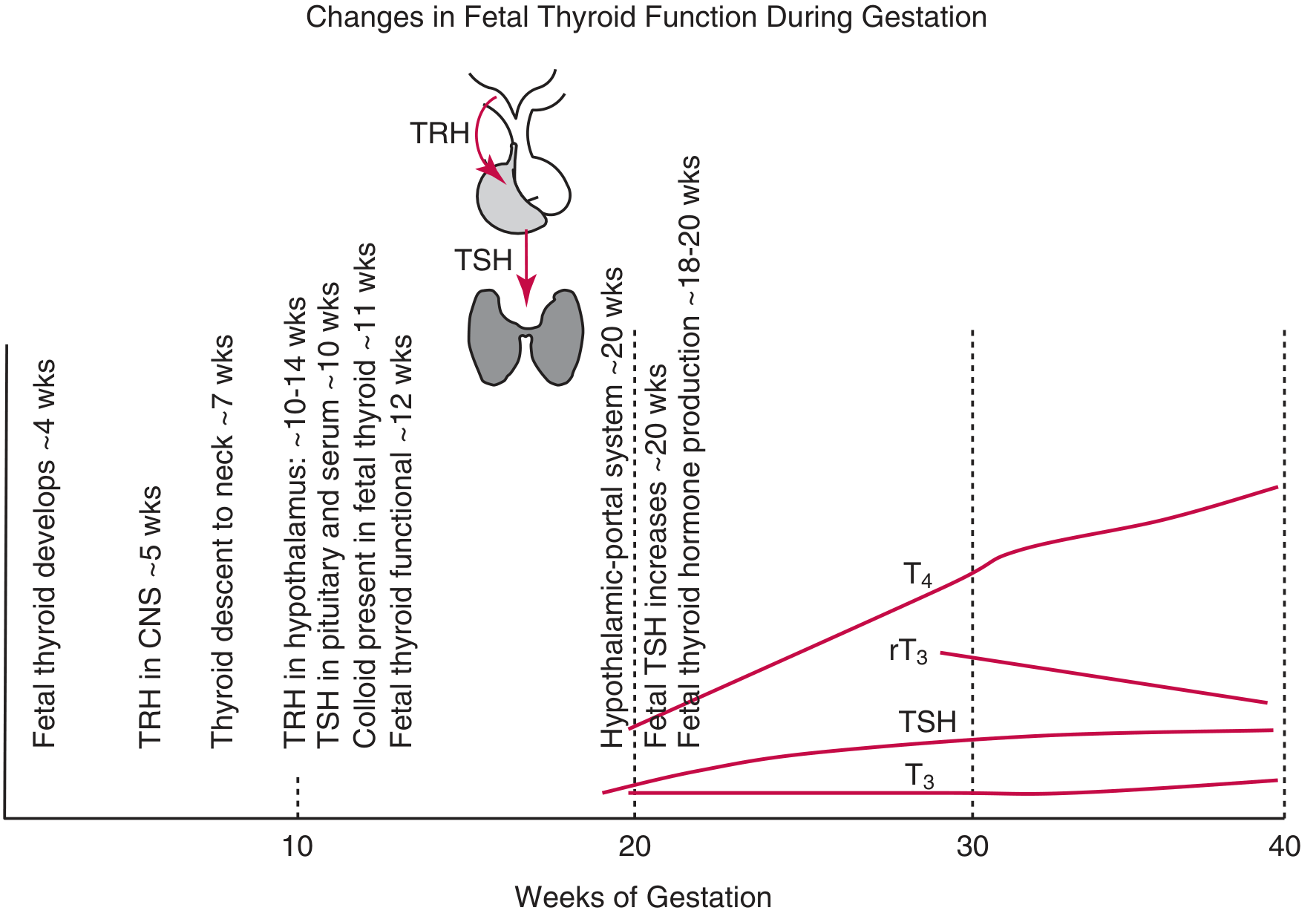
After 20 weeks, T4 steadily rises from ~2 µg/dL to adult levels of ~10 µg/dL at term, driven by pituitary TSH. Importantly, the rising T4 has minimal negative feedback on fetal TSH because the HPT axis remains immature and does not fully mature until 1-2 months after birth.
2. Fetal T3 and the Role of Deiodinases
The fetus maintains a high rT3 (reverse T3), low T3 environment deliberately:
- Type 3 deiodinase (D3) dominates in fetal tissues and the placenta - it inactivates T4 to rT3 (rather than to active T3). This protects the fetus from premature exposure to biologically active T3.
- Because of the high D3:D1 ratio, fetal serum T3 is negligible until ~30 weeks.
- Near term, increasing D1 activity allows rising T3 levels (up to ~50 ng/dL), paralleled by a progressive decline in rT3.
- Approximately 30-50% of T4 in cord blood is maternally derived, even at term.
3. The Postnatal TSH Surge - The Key Event
At birth, exposure to the cold extrauterine environment triggers a massive and rapid TRH surge from the hypothalamus, which drives an acute TSH release from the pituitary:
- TSH peaks at ~30 minutes after birth (the "neonatal TSH surge")
- This is the largest TSH rise seen at any point in human life
- By 2-3 days, TSH falls back toward adult levels under T3/T4 negative-feedback inhibition
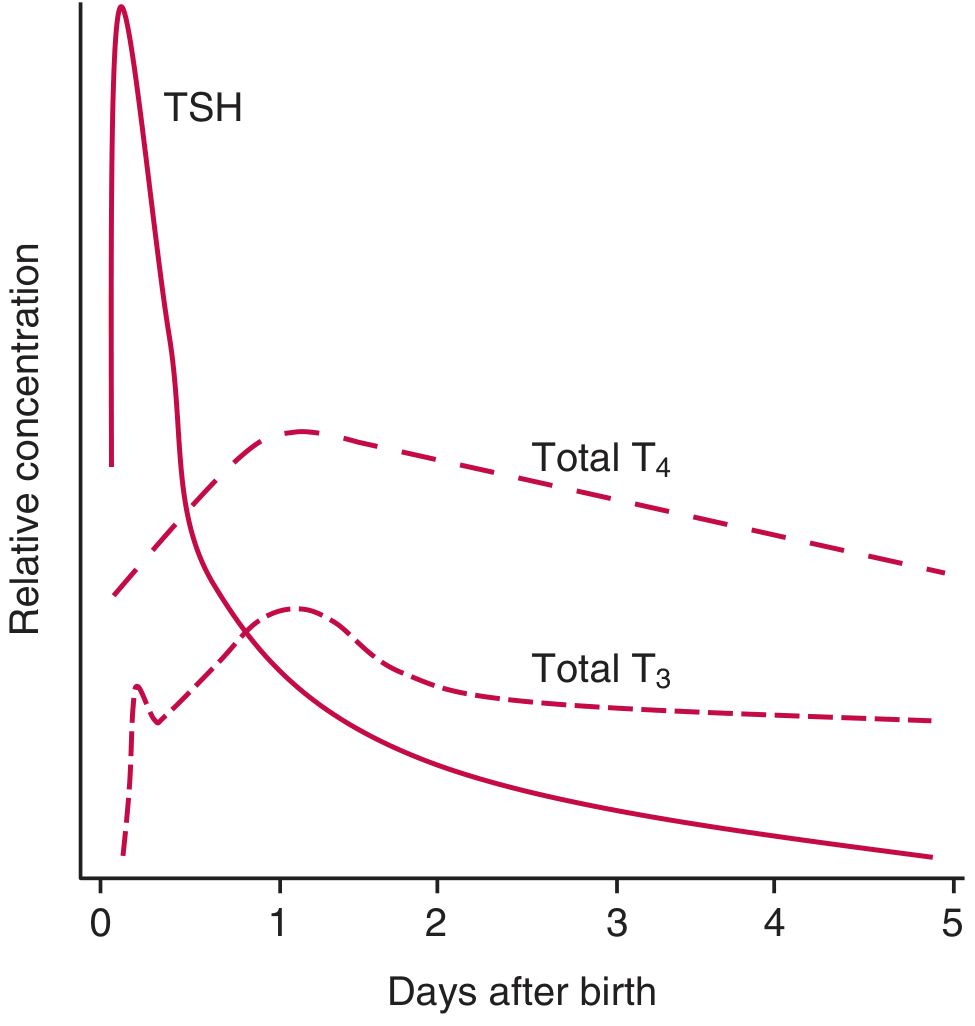
Downstream effects of the TSH surge:
- TSH stimulates the thyroid gland to massively increase T4 and T3 secretion
- T3 and T4 peak at ~24 hours after delivery
- The disproportionately greater rise in T3 vs T4 in the first 24 hours reflects acutely increased conversion of T4 → T3 via maturation of type I deiodinase (D1)
- T4 and T3 then gradually decline to stable adult-range concentrations by 4-6 weeks
- Transient hyperthyroxinemia can also be triggered by neonatal cooling and may represent a thermogenic adaptation to extrauterine life
4. The HPT Axis in Prematurity
In premature neonates, the HPT axis is immature and the physiological TSH surge is dramatically lower or absent:
- FT4 and FT3 levels are low despite "normal" TSH levels
- May take 3-8 weeks after birth to achieve levels similar to term infants
- Transient hypothalamic hypothyroidism of prematurity occurs in up to 50% of infants born before 28 weeks
- It can be difficult to distinguish from true central hypothyroidism
- Transient hypothyroxinemia in premature infants is associated with cognitive and neurological delays, but optimal treatment targets are not yet established
5. Clinical Relevance - Newborn Screening
Because TSH surges after birth, the timing of neonatal screening matters:
- Screening is ideally done at 2-4 days of age in term infants (after the physiological TSH surge has resolved)
- Within 7 days for preterm infants
- TSH-first strategy: most common - elevated TSH triggers reflex FT4
- Combined TSH + FT4: detects central hypothyroidism (low FT4 with normal or low TSH), thyroid hormone resistance, and conditions causing delayed TSH elevation
- Screening with TSH alone misses central hypothyroidism (1 in 25,000-50,000 newborns)
Congenital hypothyroidism (CH) now has an estimated incidence of 1 in 2,000-4,000 newborns (higher than the historical estimate of 1 in 7,000, due to lower TSH cut-offs). If levothyroxine is started within the first 2 weeks of life, mental retardation is preventable in over 90% of affected children. - Tietz Textbook of Laboratory Medicine, 7th Ed.; Creasy & Resnik's Maternal-Fetal Medicine, 8th Ed.
Summary Table
| Phase | TSH | T4 | T3 | Key Mechanism |
|---|---|---|---|---|
| <16 wks gestation | Low | Low (maternal) | Very low | Fetus dependent on maternal T4 |
| 16-40 wks | Gradually rising | Rising (2→10 µg/dL) | Low (D3 dominates → rT3) | Fetal HPT axis maturing |
| Birth (~30 min) | Massive surge (peak) | Rising | Rising | Cold-induced TRH release |
| Day 1 (~24 hrs) | Falling | Peak | Peak | TSH-driven secretion + D1 maturation (T4→T3) |
| Days 2-3 | Returns to normal | Plateaus then falls | Plateaus then falls | T3/T4 negative feedback |
| Weeks 4-6 | Adult levels | Adult levels | Adult levels | HPT axis fully mature |
Recent evidence note: A 2025 systematic review/meta-analysis (PMID 39954784) found that delivery mode influences neonatal TSH levels - vaginal delivery is associated with a more robust TSH surge compared to elective caesarean section, consistent with the cold-stress and catecholamine-driven mechanism of the postnatal surge.
All i need to know about migraine. From incidence among people of various age groups, pathophysiology, classification, clinical presentation, risk factors, triggers, investigations, management, prognosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
migraine pathophysiology treatment guidelines
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
That covers everything you asked for. Here is a brief orientation to the answer above:
What was covered:
-
Epidemiology - 12% 1-year global prevalence, peak in the 4th decade, 3:1 F:M ratio after puberty, childhood equivalents, chronification rates
-
Pathophysiology - The modern neurovascular model: cortical spreading depression (CSD) as the electrophysiological substrate of aura; trigeminovascular activation and neurogenic inflammation; the central role of CGRP and 5-HT; the migraine generator debate (hypothalamus + dorsal pons); central sensitization and allodynia; why the old "vascular theory" is obsolete
-
Classification - Full ICHD-3 spectrum: migraine without aura, with aura (visual/sensory/language/motor), chronic, hemiplegic, basilar/brainstem aura, retinal, status migrainosus, migrainous infarction, childhood equivalents; diagnostic criteria
-
Clinical presentation - All four phases in detail: prodrome, aura (the "marching" sensory/visual/language phenomena and how to distinguish them from TIA or seizure), headache phase, postdrome
-
Risk factors - Genetics (FHM genes, GWAS loci), sex, age, obesity, mood disorders, medication overuse, hormonal factors
-
Triggers - Stress, hormones, sleep, diet, sensory stimuli, weather, medications - and why susceptibility fluctuates daily
-
Investigations - Primarily clinical; red flags and when to image (MRI vs. CT) or perform LP; ESR/CRP, TSH
-
Management - Non-pharmacological; acute treatment stratified by severity (analgesics → triptans → lasmiditan/gepants → DHE/ergots → ED protocols → status migrainosus); preventive treatment (beta-blockers, antiepileptics, TCAs; CGRP monoclonal antibodies; botulinum toxin A for chronic migraine; gepants); special populations
-
Prognosis - Fluctuating lifelong course, improvement post-menopause, risk of chronification, MOH, rare migrainous infarction risk
This is a shared conversation. Sign in to Orris to start your own chat.