Antithyroid drugs classify pharmacokinetics adverse effect uses Carbimazole therapeutic uses adverse effect moa Propranolol in treatment of thyrotoxicosis pharmacological basis and treatment Radioactive Iodine advantage and disadvantage All answer in detail for 2nd yr mbbs pharmacology refer kd tripathi with flowcharts and diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Now I have everything needed. Let me compile the comprehensive answer:
Antithyroid Drugs - Complete 2nd Year MBBS Pharmacology
(Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, Katzung's Basic & Clinical Pharmacology - equivalent to KD Tripathi coverage)
PART 1: ANTITHYROID DRUGS - Classification, Pharmacokinetics, Adverse Effects, Uses
Classification of Antithyroid Drugs
ANTITHYROID DRUGS
│
├── 1. THIOAMIDES (Thioureylenes)
│ ├── Propylthiouracil (PTU)
│ ├── Methimazole (MMI)
│ └── Carbimazole* → converted to Methimazole
│ (* used in India, UK, Europe)
│
├── 2. IONIC INHIBITORS (Anion Inhibitors)
│ ├── Potassium Perchlorate
│ ├── Thiocyanate
│ └── Pertechnetate
│
├── 3. IODINE / IODIDES
│ ├── Lugol's iodine (5% I₂ + 10% KI)
│ └── Potassium iodide (SSKI)
│
├── 4. RADIOACTIVE IODINE
│ └── ¹³¹Iodine (¹³¹I)
│
└── 5. ADJUVANT DRUGS
├── Beta-blockers (Propranolol)
├── Calcium channel blockers
└── Glucocorticoids (in thyroid storm)
Mechanism of Action of Thioamides
Normal thyroid hormone synthesis:
Iodide (I⁻) → [TPO + H₂O₂] → Active Iodine (I⁰)
↓
Tyrosyl residues on Thyroglobulin + I⁰ → MIT, DIT
↓
MIT + DIT → [TPO coupling] → T₃, T₄
WHERE THIOAMIDES ACT:
✦ Block TPO (thyroid peroxidase) → inhibit oxidation of I⁻
✦ Block organification (iodination of tyrosines)
✦ Block coupling of MIT + DIT → no T₃/T₄ formed
✦ PTU ONLY: also blocks peripheral conversion of T₄→T₃
(via inhibition of deiodinase type 1)
✦ No effect on already-stored thyroglobulin
→ onset of action delayed 3-4 weeks
(until preformed hormone stores are depleted)
Pharmacokinetics of Thioamides
| Parameter | PTU (Propylthiouracil) | Methimazole | Carbimazole |
|---|---|---|---|
| Oral absorption | Rapid (20-30 min) | Rapid | Rapid |
| Plasma protein binding | ~75% | Nil | - |
| Plasma t½ | 75 min | 4-6 h | Converted to MMI |
| Volume of distribution | ~0.4 L/kg | ~0.7 L/kg | - |
| Duration of action | 2-3 h (100 mg dose) | Up to 24 h (10-25 mg) | - |
| Concentrated in thyroid | Yes | Yes | Yes |
| Dosing frequency | 3-4 times daily | Once or twice daily | Once or twice daily |
| Transplacental passage | Low | Low | Low |
| Breast milk levels | Low | Low | Low |
| Metabolism in liver disease | Normal | Decreased | - |
| Blocks T₄→T₃ conversion | YES | No | No |
Key Point: Methimazole's longer t½ allows once-daily dosing → better patient adherence.
Therapeutic Uses of Thioamides
- Graves' disease - primary antithyroid drug therapy (12-18 months); only treatment that preserves thyroid gland
- Preparation for thyroid surgery - render patient euthyroid preoperatively
- Adjunct before/after radioiodine - hasten control while awaiting RAI effect
- Thyroid storm - PTU preferred (also blocks T₄→T₃)
- Toxic nodular goiter
- Neonatal Graves' disease - PTU/MMI in short course
Drug of choice: Methimazole is preferred over PTU in most situations because:
- Lower risk of serious liver injury
- Once-daily dosing
- Faster onset to euthyroid state
Exception: PTU is preferred in:
- First trimester of pregnancy (methimazole is teratogenic - "aplasia cutis" + choanal atresia)
- Thyroid storm (dual action - also inhibits T₄→T₃)
Starting doses:
- Methimazole: 15-40 mg/day (mild-moderate), up to 60-80 mg/day (severe)
- PTU: 100 mg every 6-8 hours (up to 1200 mg/day in thyroid storm)
Adverse Effects of Thioamides
ADVERSE EFFECTS (occur in 3-12% of patients)
COMMON (mild):
├── Maculopapular pruritic rash (4-6%) - most common
├── Urticaria
├── Nausea, GI distress
├── Arthralgia / joint pain
├── Altered taste/smell (methimazole)
└── Mild fever
UNCOMMON (moderate):
├── Vasculitis
├── Lupus-like syndrome
├── Lymphadenopathy
└── Hypoprothrombinemia
RARE BUT SERIOUS (dangerous):
├── AGRANULOCYTOSIS ⚠️ (0.1-0.5%)
│ - Granulocyte count <500 cells/mm³
│ - Usually within first 90 days
│ - Risk ↑ with MMI >40 mg/day and in elderly
│ - Rapidly reversible on stopping drug
│ - Treat with broad-spectrum antibiotics + G-CSF
│ - 50% cross-sensitivity between PTU and MMI
│
├── HEPATOTOXICITY ⚠️
│ - PTU: Severe hepatitis, potentially fatal acute
│ liver failure (BLACK BOX WARNING)
│ - MMI: Cholestatic jaundice (less severe)
│ - Asymptomatic transaminase elevation possible
│
└── Polyserositis, exfoliative dermatitis
Onset of Action - Important for Exams
WHY IS ONSET DELAYED?
Thioamides block NEW hormone synthesis
BUT do NOT affect stored hormone in thyroglobulin
Timeline:
Day 1 → Drug blocks TPO → no new hormone made
Week 1-3 → Stored thyroglobulin still releasing T₃/T₄
Week 3-4 → Stores depleted → clinical effect appears
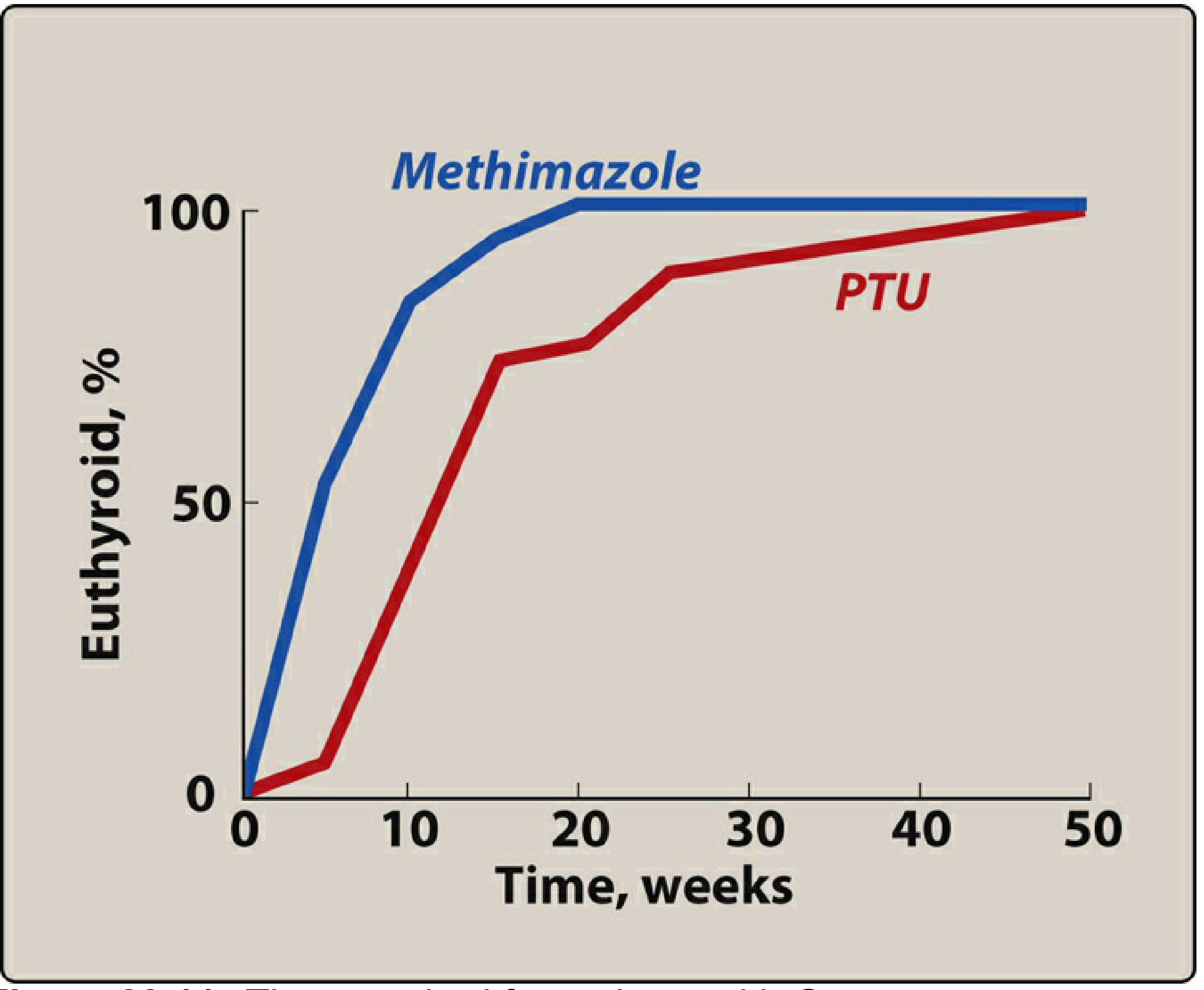
PTU onset: slightly slower (no intrathyroidal accumulation)
Methimazole onset: faster (accumulates in gland)
PART 2: CARBIMAZOLE - MOA, Therapeutic Uses, Adverse Effects
What is Carbimazole?
Carbimazole
│
│ (Carbethoxy derivative of methimazole)
│ Available in India, UK, Europe
│
▼
Absorbed orally
│
▼
Converted in liver to METHIMAZOLE (active form)
│
▼
All antithyroid activity is due to METHIMAZOLE
Carbimazole is a prodrug - it has no direct antithyroid activity itself. Its entire action comes from its active metabolite methimazole.
Mechanism of Action (Carbimazole → Methimazole)
MECHANISM OF CARBIMAZOLE (via Methimazole):
Step 1: Absorption
Carbimazole →[gut/liver]→ METHIMAZOLE
Step 2: Methimazole acts on thyroid peroxidase (TPO)
Iodide (I⁻)
↓ [TPO + H₂O₂]
× ← BLOCKED by Methimazole
↓
Active iodine (I⁰) -- NOT FORMED
Result:
• No organification (iodination of tyrosines)
• No coupling of MIT + DIT
• T₃ and T₄ synthesis halted
Step 3: Does NOT block T₄→T₃ conversion
(Unlike PTU, methimazole/carbimazole does not
inhibit peripheral deiodinase)
Step 4: IMMUNOSUPPRESSIVE effect (unique to thioamides)
• Reduces TSH-receptor antibody titers in Graves' disease
• May contribute to long-term remission
Therapeutic Uses of Carbimazole
- Graves' disease (diffuse toxic goiter) - first-line in UK, India
- Toxic multinodular goiter
- Toxic adenoma
- Preoperative preparation for thyroidectomy (render euthyroid + reduce gland vascularity when combined with iodine)
- Adjunct to radioiodine - used before/after RAI to hasten control
- Thyrotoxicosis in pregnancy - switched to PTU in first trimester
Dosing: Starting dose 20-60 mg/day in divided doses; maintenance 5-15 mg/day once euthyroid.
Adverse Effects of Carbimazole
These are identical to methimazole (since it IS methimazole):
CARBIMAZOLE ADVERSE EFFECTS
COMMON:
├── Rash (maculopapular, urticarial)
├── Nausea, GI upset
├── Headache
├── Altered taste/smell
└── Joint pains (arthralgia)
SERIOUS:
├── Agranulocytosis (0.1-0.5%)
│ ⚠️ Warn patient: report sore throat/fever immediately
│ → Stop drug → Do WBC count
│
├── Cholestatic jaundice
│ (less severe than PTU-related hepatotoxicity)
│
└── Aplasia cutis (scalp skin defect in neonate)
← If used in first trimester → switch to PTU
TERATOGENICITY:
Choanal atresia + aplasia cutis syndrome
Risk: First trimester exposure
→ PTU preferred in first trimester
→ Switch back to carbimazole/MMI in 2nd/3rd trimester
PART 3: PROPRANOLOL IN THYROTOXICOSIS - Pharmacological Basis and Treatment
Why Use Propranolol in Thyrotoxicosis?
PATHOPHYSIOLOGY OF THYROTOXICOSIS SYMPTOMS:
Excess T₃/T₄
│
├── Upregulation of β-adrenergic receptors
│ ↓
│ SYMPATHOMIMETIC EFFECTS:
│ • Tachycardia / palpitations
│ • Tremor
│ • Anxiety / nervousness
│ • Sweating
│ • Heat intolerance
│ • Lid lag / lid retraction (stare)
│ • Atrial fibrillation
│
└── Increased sensitivity to catecholamines
↓
All symptoms exacerbated
PROPRANOLOL → Blocks β₁ and β₂ receptors → Rapid symptomatic relief
Pharmacological Basis of Propranolol in Thyrotoxicosis
PROPRANOLOL: NON-SELECTIVE β-BLOCKER (β₁ + β₂)
1. β₁ BLOCKADE (cardiac):
├── ↓ Heart rate → controls tachycardia
├── ↓ Cardiac output
└── Controls palpitations, arrhythmias (AF)
2. β₂ BLOCKADE (peripheral):
├── ↓ Tremor
├── ↓ Anxiety
└── ↓ Sweating
3. UNIQUE EFFECT (beyond beta-blockade):
Propranolol INHIBITS peripheral conversion of T₄ → T₃
(deiodinase type 1 inhibition)
├── This reduces levels of active T₃
├── Also seen with PTU (additive effect)
└── High doses required (>160 mg/day)
4. Does NOT affect:
├── Thyroid hormone synthesis
├── Thyroid hormone release
└── Underlying disease process
Role in Treatment
WHEN TO USE PROPRANOLOL:
A. ADJUVANT THERAPY (most common use):
Given ALONGSIDE thioamides while waiting for
antithyroid drugs to work (3-4 week delay)
↓
Rapid symptomatic relief in first 2-4 weeks
B. THYROID STORM:
Essential component of treatment
High doses: 40-80 mg every 4-6 hours
Controls dangerous tachycardia/arrhythmias
C. PREOPERATIVE PREPARATION:
When surgery needed urgently
Used with iodine to reduce gland vascularity
D. RAI PREPARATION/POST-RAI:
Controls symptoms before and after radioiodine
(RAI takes 6-12 weeks to work)
E. THYROTOXIC CRISIS / STORM:
IV propranolol: 0.5-1 mg slowly IV (monitored)
Oral: 40-80 mg every 4-6 hours
DOSES:
Mild thyrotoxicosis: 40-120 mg/day in divided doses
Thyroid storm: up to 240-480 mg/day
Contraindications of Propranolol in Thyrotoxicosis
CONTRAINDICATIONS:
├── Asthma / COPD (β₂ blockade causes bronchospasm)
├── Heart failure / cardiac decompensation
├── Heart block (2nd/3rd degree)
├── Severe bradycardia
└── Raynaud's phenomenon (peripheral vascular disease)
ALTERNATIVES when propranolol contraindicated:
├── Atenolol (β₁ selective) - safer in mild respiratory disease
├── Metoprolol (β₁ selective)
├── Diltiazem (Ca²⁺ channel blocker) - for rate control
└── Verapamil - when beta-blockers absolutely contraindicated
Mechanism Summary - Propranolol vs. Thioamides
COMPARISON OF ACTION:
Propranolol PTU/MMI
----------- -------
Blocks TPO No YES
Stops T₃/T₄ synthesis No YES
Blocks T₄→T₃ YES PTU only
Symptomatic relief RAPID Delayed 3-4 wks
Controls tachycardia YES Indirect only
Treats underlying cause No No
Reduces TSH-RAb No YES (partial)
→ Used TOGETHER for optimal early management
PART 4: RADIOACTIVE IODINE (¹³¹I) - Advantages and Disadvantages
Mechanism of Action of ¹³¹I
RADIOACTIVE IODINE (¹³¹I):
Physical Properties:
├── Half-life: 8 days
├── Emits: β-particles (90%) + γ-rays (10%)
├── β-particles: tissue penetration 0.5-2 mm
│ → THERAPEUTIC EFFECT (local destruction)
└── γ-rays: for scanning/imaging
HOW IT WORKS:
Oral ¹³¹I
↓
Absorbed → enters blood
↓
Taken up by thyroid via NIS
(sodium/iodide symporter)
↓
¹³¹I concentrated in follicular cells
↓
β-radiation → DNA damage → follicular cell death
↓
Gland shrinks → hormone production ↓
↓
Euthyroid/hypothyroid state achieved
Duration: Effect takes 6-12 weeks to manifest
Cure rate: 80% after single dose; ~20% need 2nd dose
Dosing / Administration
- Standard dose for Graves': 5-15 mCi (185-555 MBq) orally as a single dose
- Larger doses for toxic multinodular goiter
- Thyroid cancer: 30-150 mCi ablative doses (higher)
- Patient is euthyroid within 6-12 weeks in most cases
Advantages of Radioactive Iodine
ADVANTAGES OF ¹³¹I:
1. SIMPLICITY
└── Single oral dose (tablet/liquid)
2. NO SURGERY
└── Avoids operative risks (recurrent laryngeal
nerve injury, hypoparathyroidism, bleeding)
3. COST-EFFECTIVE
└── Cheaper than surgery overall
4. OUTPATIENT PROCEDURE
└── No hospitalization required in most countries
5. HIGH EFFICACY
└── 80% cured with one dose
└── ~99% cured with repeat doses
6. PREFERRED FOR:
├── Elderly patients (poor surgical candidates)
├── Recurrent hyperthyroidism after surgery
├── Cardiac disease complicating thyrotoxicosis
├── Failure of antithyroid drug therapy
└── Allergic to thioamides
7. PERMANENT CURE
└── Eliminates the relapse rate seen with drug therapy
8. NO GENERAL ANESTHESIA REQUIRED
9. DOES NOT WORSEN exophthalmos significantly
(though mild worsening possible)
Disadvantages of Radioactive Iodine
DISADVANTAGES OF ¹³¹I:
1. DELAYED EFFECT (MAJOR)
└── Takes 6-12 weeks to achieve euthyroid state
└── Bridging therapy with propranolol ± thioamides needed
2. HYPOTHYROIDISM (MOST COMMON CONSEQUENCE)
├── High incidence of permanent hypothyroidism
├── ~80% at 10 years, ~100% eventually
└── Lifelong levothyroxine replacement required
3. RADIATION THYROIDITIS
├── Release of stored T₃/T₄ into circulation
├── Worsening of hyperthyroid symptoms
├── Rarely → thyroid storm
└── Prevented by pretreatment with thioamides
4. RISK OF MALIGNANCY (controversial)
├── Some studies: small ↑ risk of stomach, kidney,
│ breast cancer (all express NIS transporter)
└── Overall cancer death rate NOT increased
5. CONTRAINDICATED IN PREGNANCY ⚠️ (ABSOLUTE)
├── After 1st trimester: fetal thyroid concentrates ¹³¹I
├── → Fetal hypothyroidism + cretinism
└── Even in 1st trimester: radiation to fetal tissues
6. CONTRAINDICATED IN BREASTFEEDING
└── ¹³¹I excreted in breast milk
7. CONTROVERSIAL IN CHILDREN
├── Theoretical neoplastic risk in developing thyroid
└── Most centers avoid in patients <25-30 years
8. WORSENING OF GRAVES' OPHTHALMOPATHY
└── Radioiodine may worsen pre-existing eye disease
└── Prophylactic glucocorticoids recommended in
those with significant ophthalmopathy
9. RADIATION PRECAUTIONS NEEDED
├── Limit close contact with young children, pregnant women
└── For 7-14 days post-treatment
10. NOT SUITABLE FOR LARGE GOITERS
└── Very large/retrosternal goiters: surgery preferred
(poor ¹³¹I access + risk of airway compromise)
Summary Table: Three Treatment Modalities for Thyrotoxicosis
┌─────────────────┬────────────────┬──────────────┬──────────────┐
│ Feature │ Antithyroid │ Radioiodine │ Surgery │
│ │ Drugs │ (¹³¹I) │ (Thyroidecto-│
│ │ │ │ my) │
├─────────────────┼────────────────┼──────────────┼──────────────┤
│ Mechanism │ Block TPO │ Radiation │ Physical │
│ │ ± T₄→T₃ │ cell death │ removal │
├─────────────────┼────────────────┼──────────────┼──────────────┤
│ Onset │ 3-4 weeks │ 6-12 weeks │ Immediate │
├─────────────────┼────────────────┼──────────────┼──────────────┤
│ Relapse rate │ 50-60% │ Very low │ Low (5-10%) │
├─────────────────┼────────────────┼──────────────┼──────────────┤
│ Hypothyroidism │ If overdosed │ ~80-100% │ Common │
│ risk │ │ long term │ │
├─────────────────┼────────────────┼──────────────┼──────────────┤
│ Pregnancy │ PTU (1st tri) │ Contraindic- │ 2nd trimester│
│ │ MMI (2nd/3rd) │ ated │ only │
├─────────────────┼────────────────┼──────────────┼──────────────┤
│ Preferred in │ Young pts, │ Elderly, │ Large goiter,│
│ │ pregnancy, │ failed drugs,│ malignancy │
│ │ mild disease │ post-surgery │ suspected │
└─────────────────┴────────────────┴──────────────┴──────────────┘
Quick Flowchart: Management of Thyrotoxicosis (Graves')
GRAVES' DISEASE DIAGNOSED
│
▼
Start Propranolol → IMMEDIATE symptom control
+ Start Methimazole/Carbimazole
│
▼ (3-4 weeks)
Euthyroid?
/ \
YES NO
│ ↑ dose or switch
│
▼
Continue 12-18 months
(check for remission)
│
Remission?
/ \
YES NO → Choose Definitive Rx
Stop Rx │
┌────┴─────┐
▼ ▼
Radioiodine Thyroidectomy
(if >25 yr, (if large goiter,
no pregn.) malignancy
suspected)
Key Points for 2nd Year MBBS Exam
| Drug | Key Fact |
|---|---|
| Carbimazole | Prodrug → converted to methimazole |
| PTU | ONLY thioamide that also blocks T₄→T₃ |
| Methimazole | Drug of choice in Graves' (once daily, less toxic) |
| PTU | Preferred in 1st trimester pregnancy + thyroid storm |
| Propranolol | Controls symptoms rapidly; also blocks T₄→T₃ at high doses |
| ¹³¹I | Contraindicated in pregnancy; delayed effect 6-12 weeks |
| Agranulocytosis | Most dangerous ADR of thioamides (0.1-0.5%) |
| Wolff-Chaikoff effect | High iodide transiently inhibits organification |
| Iodine (Lugol's) | Used pre-op; reduces gland vascularity; NOT for long-term use |
References:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, 13th Ed., Chapter 47 (Thyroid & Antithyroid Drugs), Tables 47-5
- Katzung's Basic & Clinical Pharmacology, 16th Ed., Chapter 38 (Thyroid & Antithyroid Drugs)
- Lippincott Illustrated Reviews: Pharmacology, Chapter 23
This is a shared conversation. Sign in to Orris to start your own chat.