Emphysema
Reading File
Finding Sources
Searching PubMed
emphysema pathophysiology treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have enough comprehensive information to write a complete, well-cited answer on emphysema. Let me compile it now.
Emphysema
Definition
Emphysema is defined as permanent enlargement of airspaces distal to the terminal bronchioles, accompanied by destruction of alveolar walls without significant fibrosis. It is an anatomic diagnosis. Along with chronic bronchitis, it forms a major component of COPD.
- Robbins & Kumar Basic Pathology, p. 448
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 634
Types / Classification
Emphysema is classified by the part of the acinus (the terminal respiratory unit) that is involved. Recall: a lobule = cluster of 3-5 acini; an acinus = structures distal to the terminal bronchiole.
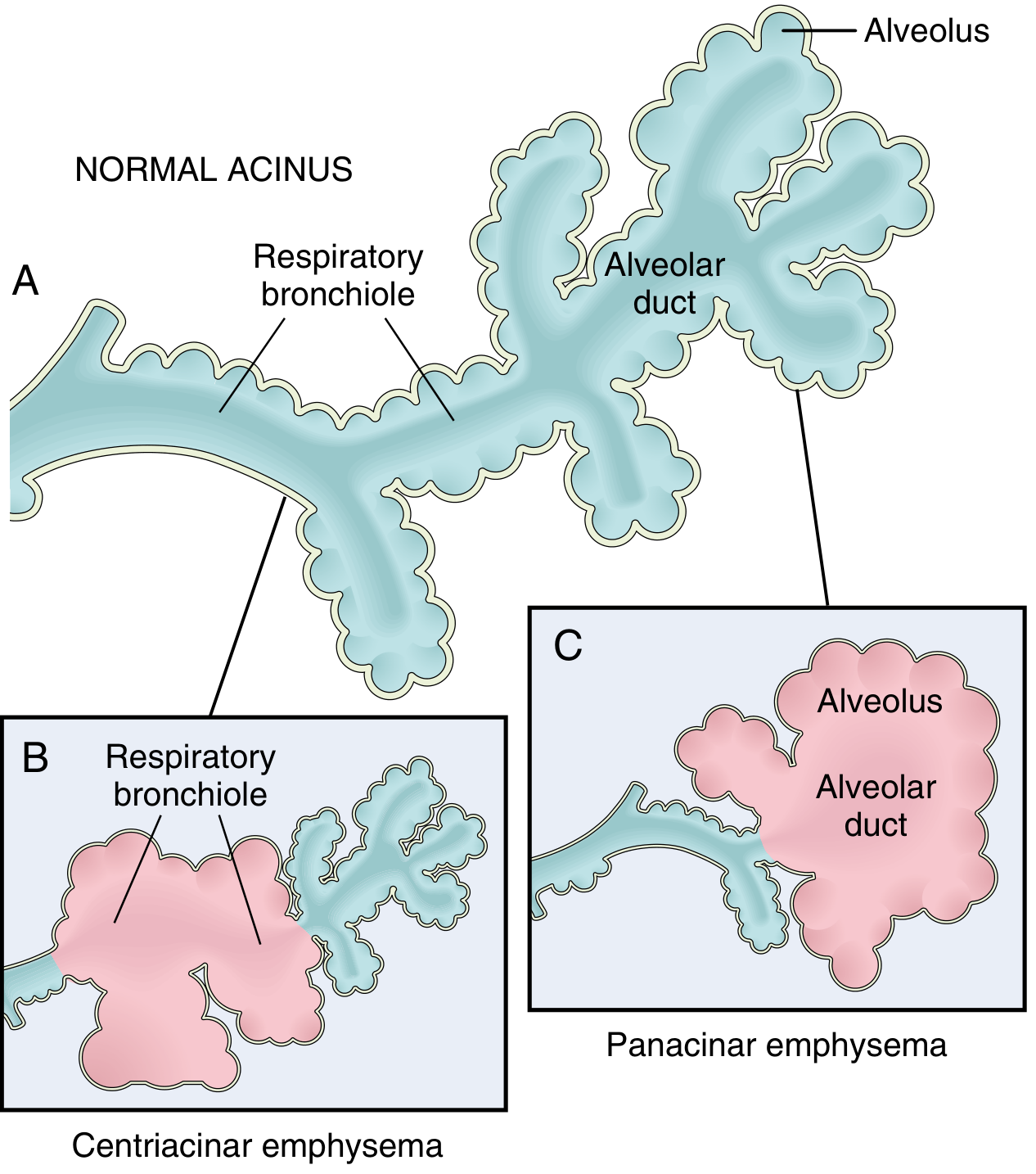
Fig. 15.6 - Major patterns of emphysema. (A) Normal acinus. (B) Centriacinar emphysema - dilation starts at the respiratory bronchioles. (C) Panacinar emphysema - distention of the entire acinus including alveolus and alveolar duct.
| Type | Area Involved | Key Associations | Location |
|---|---|---|---|
| Centriacinar (Centrilobular) | Central/proximal acinus - respiratory bronchioles first, distal alveoli spared | Most common (>95%); cigarette smoking; heavy smokers with COPD | Upper lobes, apical segments |
| Panacinar (Panlobular) | Entire acinus uniformly enlarged - from respiratory bronchiole to terminal blind alveoli | α1-antitrypsin deficiency (exacerbated by smoking) | Lower lobes, anterior margins |
| Distal Acinar (Paraseptal) | Distal part of acinus; proximal part normal | Spontaneous pneumothorax in young adults; bulla formation | Adjacent to pleura, lobular septa; upper lobes |
| Irregular (Paracicatricial) | Irregular involvement; associated with scarring | Usually clinically insignificant | Near scars/fibrosis |
Only centriacinar and panacinar types cause clinically significant airflow obstruction.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 634-635
Pathogenesis
The core mechanism is protease-antiprotease imbalance combined with oxidative stress and inflammation triggered by cigarette smoke and pollutants.
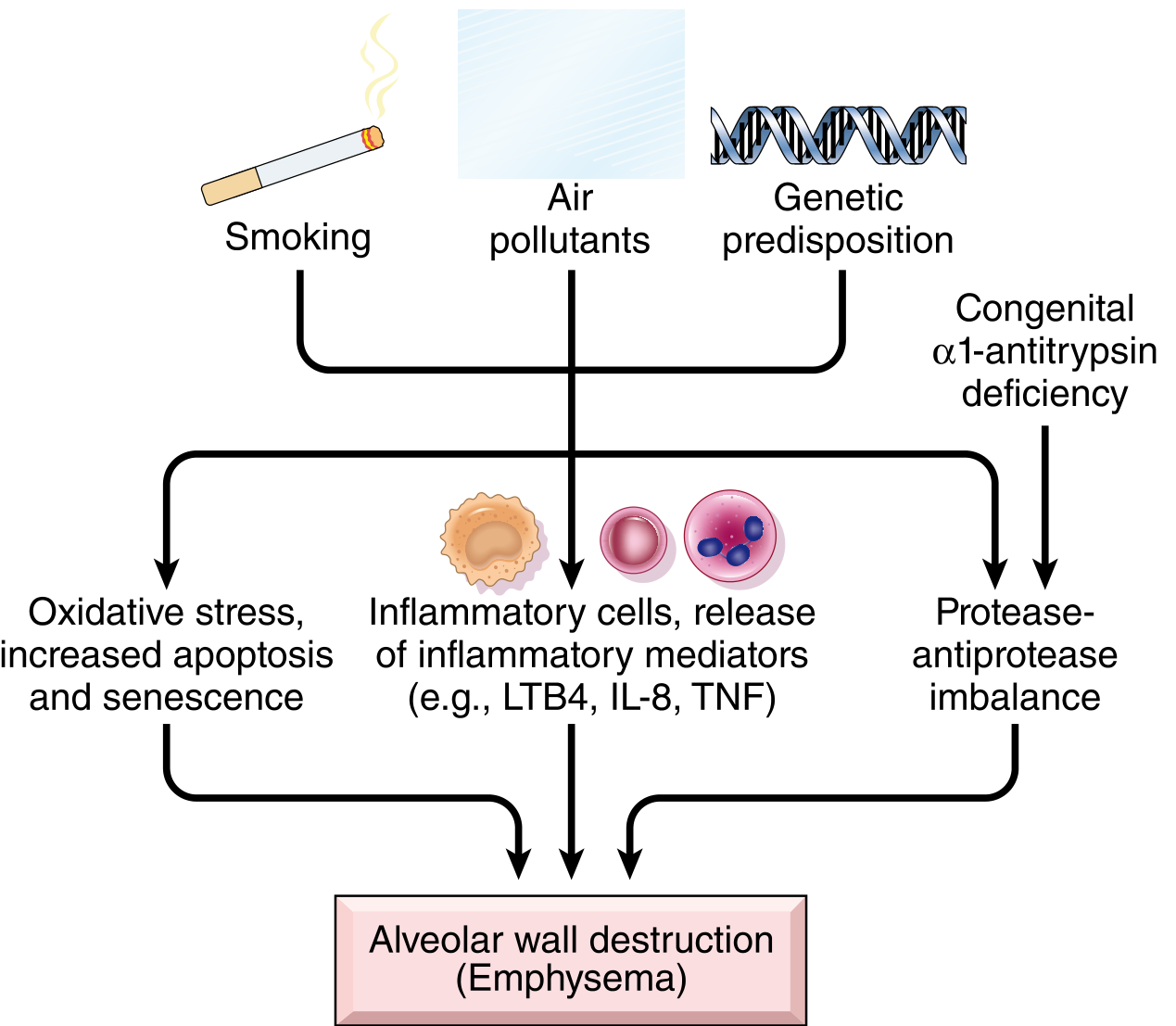
Fig. 15.8 - Pathogenesis of emphysema: Smoking, air pollutants, and genetic predisposition (α1-antitrypsin deficiency) converge through oxidative stress, inflammatory mediators (LTB4, IL-8, TNF), and protease-antiprotease imbalance to cause alveolar wall destruction.
1. Toxic Injury and Inflammation
- Cigarette smoke damages respiratory epithelium and activates macrophages and resident epithelial cells
- Inflammatory mediators released: LTB4, IL-8, TNF, and others
- Leads to accumulation of neutrophils, T cells, B cells in affected lung
- Role: chemotaxis, amplification of inflammation, structural changes via growth factors
2. Protease-Antiprotease Imbalance
- Inflammatory cells release elastases and other proteases that degrade connective tissue (especially elastin)
- In healthy individuals, α1-antitrypsin (encoded at the Pi locus, chromosome 14) inhibits these proteases - mainly neutrophil elastase
- When antiprotease defense is overwhelmed or deficient, elastin destruction proceeds unchecked
α1-Antitrypsin Deficiency:
- Accounts for ~1% of all emphysema cases
- Pi locus is polymorphic; ~0.012% of the US population is homozygous ZZ genotype (very low serum AAT)
-
80% of ZZ individuals develop symptomatic panacinar emphysema, earlier and more severe if they smoke
- Smoking compounds the deficiency by increasing protease load and inhibiting remaining AAT
3. Oxidative Stress
- Tobacco smoke and inflammatory cells generate reactive oxygen species (ROS)
- ROS cause tissue damage, endothelial dysfunction, and amplify inflammation
- NRF2 (encoded by NFE2L2) is the cellular oxidant sensor in alveolar epithelial cells - its inactivation in mice markedly increases susceptibility to smoke-induced emphysema
- Genetic variants in NRF2 and its regulators are associated with smoking-related lung disease in humans
4. Airway Obstruction Mechanism
-
Small airways are normally held open by elastic recoil of surrounding parenchyma
-
Destruction of elastic tissue reduces radial traction on respiratory bronchioles
-
Bronchioles collapse during expiration → functional airflow obstruction (not mechanical)
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 635-637
Morphology
Gross:
- Voluminous, pale lungs (especially in panacinar type) - often overlap the heart anteriorly at autopsy
- Upper two-thirds more severely affected in smoking-related disease
- Large alveoli visible on cut surface
- Apical blebs or bullae in advanced/irregular emphysema (spaces >1 cm when distended)
Microscopic:
- Abnormally large alveoli separated by thin septa
- Focal centriacinar fibrosis
- Loss of attachments between alveoli and outer wall of small airways
- Pores of Kohn markedly enlarged - septa appear to "float" or protrude blindly ("club-shaped")
- Decreased capillary bed area
- Inflammatory changes in small airways often superimposed
- Secondary pulmonary hypertension changes: from local hypoxemia and capillary loss
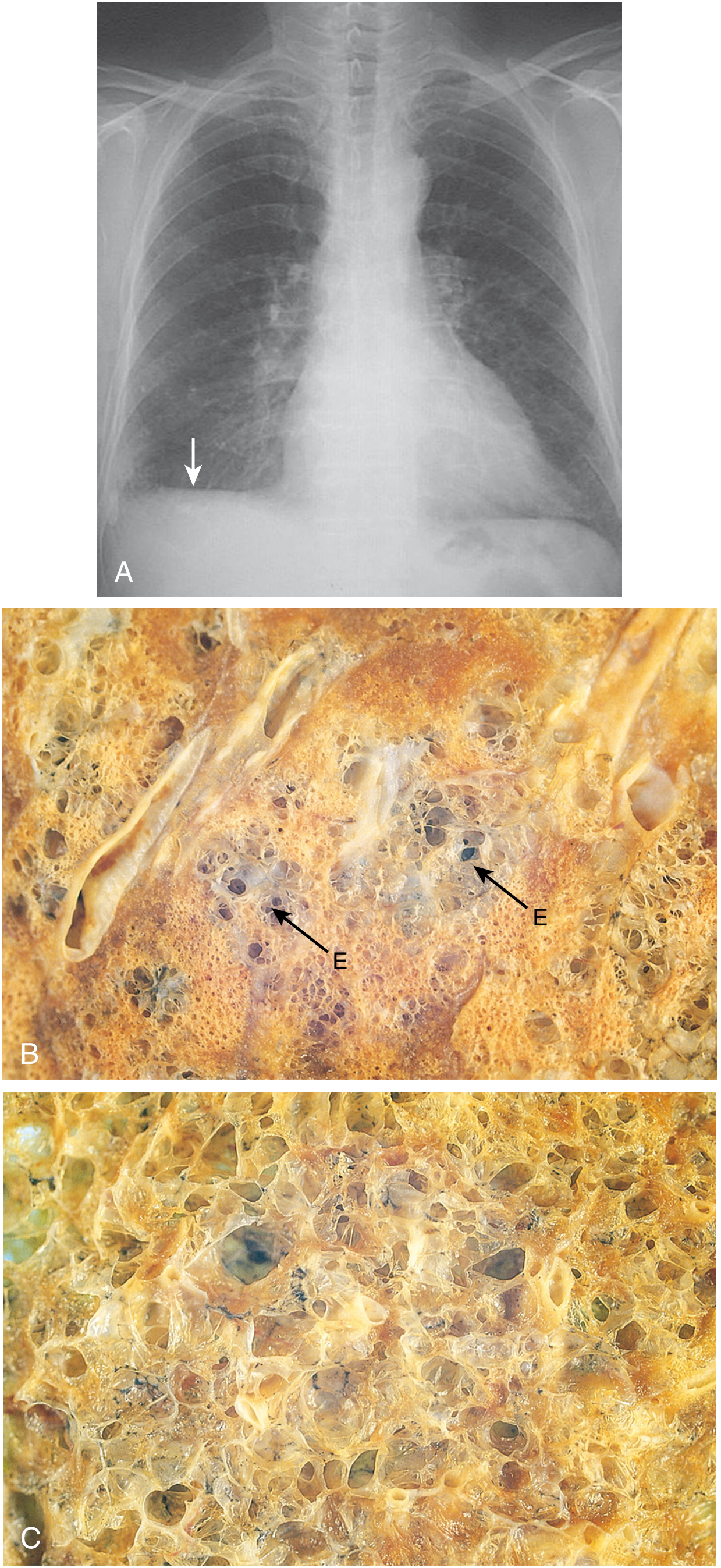
Fig. 15.7 - (A) Chest X-ray: hyperinflated lungs with flattened diaphragm. (B) Centriacinar emphysema - focal enlarged airspaces (E). (C) Panacinar emphysema - diffusely enlarged airspaces throughout the acinus.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 636
Clinical Features
Emphysema typically presents insidiously in long-term heavy smokers:
| Feature | Description |
|---|---|
| Dyspnea | Main symptom; initially on exertion, progresses to rest |
| Cough | Often mild (unlike chronic bronchitis); may be productive if coexisting bronchitis |
| Barrel chest | Increased AP diameter from lung hyperinflation |
| Pursed-lip breathing | Creates auto-PEEP to prevent airway collapse on expiration |
| Accessory muscle use | Tripod posture; scalene and sternocleidomastoid recruitment |
| "Pink Puffer" | Classic emphysema phenotype - thin, dyspneic, tachypneic, but relatively well-oxygenated; vs. "Blue Bloater" in chronic bronchitis |
| Diminished breath sounds | Hyperinflated lungs attenuate sounds |
| Percussion | Hyperresonant |
| Weight loss | Due to increased work of breathing and systemic inflammation |
PFTs:
- Obstructive pattern: reduced FEV1/FVC ratio
- Increased TLC, RV, FRC (air trapping)
- Reduced DLCO (loss of capillary surface area - distinguishes from asthma)
Complications:
- Cor pulmonale (right heart failure from pulmonary hypertension)
- Secondary polycythemia (from chronic hypoxemia)
- Spontaneous pneumothorax (especially with bullae or paraseptal type)
- Respiratory failure
Other Forms of Emphysema (Non-COPD)
- Compensatory hyperinflation - alveolar dilation compensating for lung tissue loss (e.g., post-lobectomy); not true destruction
- Obstructive overinflation - air trapping distal to a partial obstruction (tumor, foreign body); can be life-threatening
- Bullous emphysema - large subpleural blebs/bullae (>1 cm); can rupture causing pneumothorax
- Interstitial emphysema - air in connective tissue stroma, mediastinum, or subcutaneous tissue; from alveolar tears during coughing or from penetrating chest wounds
Management
Management is largely that of COPD:
| Category | Treatment |
|---|---|
| Smoking cessation | Single most important intervention to slow progression |
| Bronchodilators | SABAs, LABAs, LAMAs (tiotropium) - relieve symptoms |
| Inhaled corticosteroids | Combined with LABAs in moderate-severe disease |
| Pulmonary rehabilitation | Improves exercise tolerance and quality of life |
| Long-term oxygen therapy | When PaO2 <55 mmHg or SaO2 ≤88%; prolongs survival |
| α1-AT replacement | Weekly IV augmentation therapy for confirmed AAT deficiency |
| Lung volume reduction surgery (LVRS) | Selected patients with upper-lobe predominant, severe emphysema |
| Bronchoscopic LVR | Endobronchial valves, coils, thermal vapor ablation - less invasive options with growing evidence |
| Lung transplantation | End-stage disease |
Recent systematic reviews (2024-2025) confirm that bronchoscopic lung volume reduction (endobronchial valves in particular) significantly improves FEV1, 6-minute walk distance, and quality of life in patients with severe emphysema with low collateral ventilation:
- Bronchoscopic LVR network meta-analysis (2024) PMID: 39095948
- Extrapulmonary effects of LVR in severe emphysema (2025) PMID: 40174955
- LVR therapies network meta-analysis (2025) PMID: 41037331
Sources:
- Robbins & Kumar Basic Pathology, pp. 447-449
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 634-638
- Murray & Nadel's Textbook of Respiratory Medicine, p. 1413
- Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.