types of incision used in tympanomastoid surgery with photo
Reading File
Finding Sources
Finding Sources
Searching the Web
types of incisions tympanomastoid surgery postauricular endaural
Finding Sources
Reading Web Page
https://entokey.com/incisions-and-approaches
Loading Image
Loading Image
Finding Sources
Loading Image
Loading Image
Loading Image
Searching the Web
postauricular incision mastoidectomy tympanomastoid surgery diagram photo
Loading Image
Loading Image
I now have excellent images and detailed content. Let me compile the comprehensive answer.
Incisions Used in Tympanomastoid Surgery
Three main incisions are used for tympanomastoid surgery, each with specific indications, advantages, and limitations. A fourth group - extended incisions for skull base access - is used for complex lateral cranial base work.
1. Transcanal (Endomeatal) Incision
The transcanal approach is performed entirely through the external auditory canal without any external skin incision. It is appropriate for procedures limited to the tympanic membrane and the posterior tympanic compartment.
Technique:
- Canal incisions are made with a tympanomeatal flap
- A posteriorly based flap (Rosen incision) is typical - the posterior canal skin is elevated and folded forward to expose the middle ear
Indications:
- Myringotomy and grommet insertion
- Stapedectomy / stapedotomy
- Small posterior tympanic membrane perforations
- Ossiculoplasty with limited disease
- Small posterior glomus tympanicum tumors
Advantages: No external scar, least invasive, suitable for outpatient procedures
Limitation: Restricted posterior and mastoid access
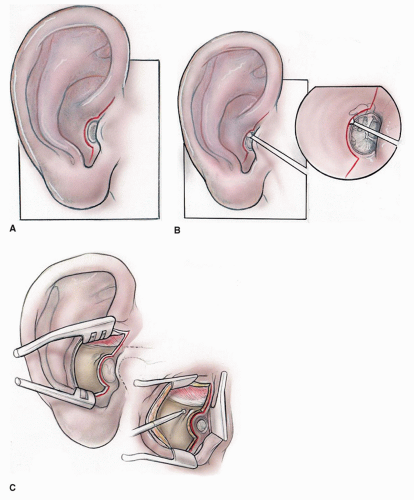
2. Endaural Incision
The endaural incision was first described over 100 years ago. It has three segments:
- Circumferential (meatal) limb - runs circumferentially around the canal entrance
- Intercartilaginous limb - passes between the helical crus and the tragus (between the two cartilaginous portions)
- Vertical (superior) limb - extends superiorly through the skin toward the temporalis fascia


Indications:
- Tympanoplasty (especially anterior and total perforations)
- Canalplasty for exostoses
- Anterior atticotomy
- Epitympanic procedures
- Can be extended (Heermann modification) for mastoidectomy in narrow canals
- Preferred when the external canal or meatus is abnormally small
Advantages:
- Does not interrupt the majority of cutaneous innervation of the pinna → no postoperative hypesthesia of the auricle
- Generally no mastoid dressing needed → ideal for day surgery
- Auricle does not migrate anteriorly postoperatively (avoids collapsing canal)
- Direct access to the epitympanum
Limitations:
- Visible scar (between helical crus and tragus)
- Limited posterior exposure compared to postauricular approach
- Less commonly used today than postauricular due to scar visibility and restricted access when mastoid work is extensive
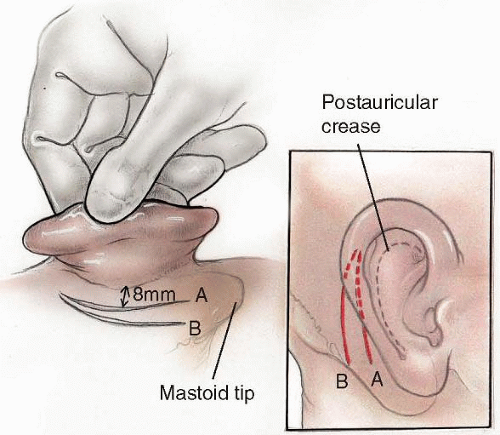
3. Postauricular Incision
The postauricular incision is the workhorse of tympanomastoid surgery. It is made in the postauricular sulcus (the crease behind the ear), running parallel to and approximately 5-8 mm behind the postauricular crease from above the auricle down to the mastoid tip.
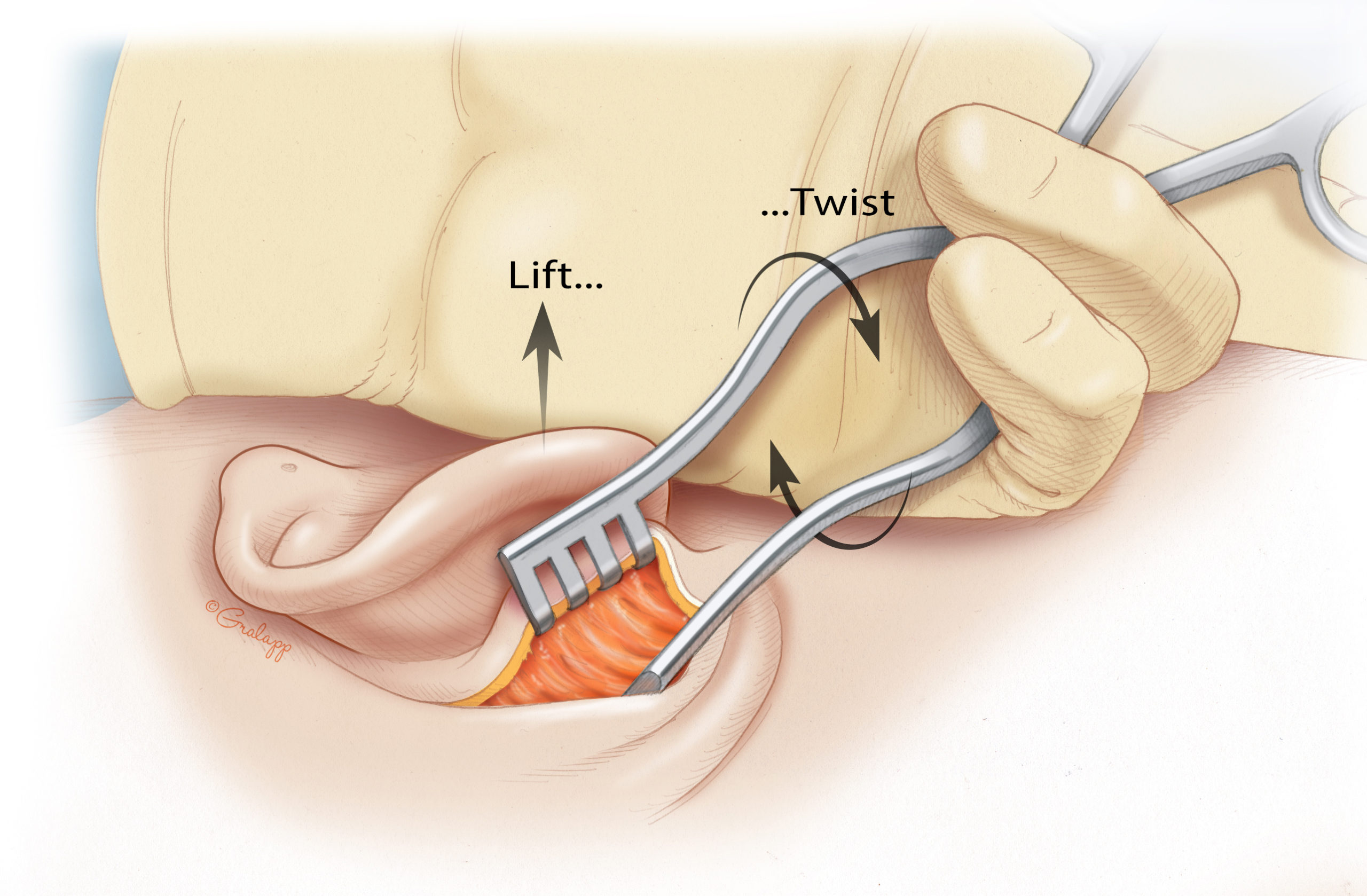
Technique steps:
- Incision through skin in the postauricular sulcus
- Superior limb carried forward to allow the ear to rotate anteriorly
- Identify temporalis fascia and linea temporalis
- Periosteal incision along linea temporalis extended to the anterior aspect of the canal
- Soft tissues rotate forward for full view down the canal to the middle ear
- Periosteum is opened over the mastoid cortex to the mastoid tip
Indications:
- Mastoidectomy (cortical, modified radical, radical)
- Tympanoplasty with mastoid disease
- Ossiculoplasty with extensive middle ear pathology
- Cholesteatoma surgery
- Cochlear implantation (modified postauricular with superior extension)
- Any procedure requiring combined tympanomastoid access
Advantages:
- Excellent exposure of the tympanomastoid compartment
- Scar hidden behind the ear
- Allows harvesting of temporalis fascia graft (through the same incision)
- Allows periosteal graft harvest
- Most versatile for complex cases
Limitations:
- More invasive than endaural or transcanal
- Risk of auricle migrating anteriorly postoperatively → possible collapsing canal
- Cutaneous innervation of the pinna interrupted → temporary or permanent hypesthesia of auricle
- Mastoid dressing usually required postoperatively
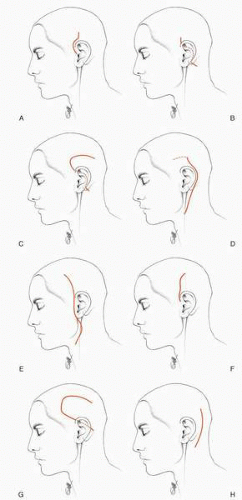
4. Extended and Skull Base Incisions
For lateral cranial base procedures, the postauricular incision is modified:
| Incision | Access |
|---|---|
| Modified postauricular (with superior extension) | Temporal fossa; cochlear implantation |
| Extended postauricular | Tympanomastoid + upper neck + infratemporal fossa |
| Preauricular (lateral facial) | Upper neck and infratemporal fossa |
| Postauricular transtemporal | Middle fossa surface of temporal bone |
| Suboccipital | Posterior fossa |
The figure below shows these variants:
Comparison Summary
| Feature | Transcanal | Endaural | Postauricular |
|---|---|---|---|
| External scar | None | Yes (inter-cartilaginous) | No (hidden) |
| Mastoid access | None | Limited (Heermann extension) | Full |
| Epitympanum access | Limited | Excellent | Excellent |
| Postop dressing | None | Usually none | Usually required |
| Auricle hypesthesia | None | None/minimal | Yes |
| Graft harvest (temporalis fascia) | No | Yes (limited) | Yes (full) |
| Ideal for | Minor TM/ossicular work | Canal, epitympanum, anterior perforations | Mastoidectomy, cholesteatoma, cochlear implant |
Sources:
- Incisions and Approaches - Ento Key (Jackler's chapter on ear surgery)
- Endaural Incision - Stanford Oto Surgery Atlas (Jackler & Gralapp)
- Postauricular Incision - Stanford Oto Surgery Atlas
- Illustrations: Gralapp / Stanford Oto Surgery Atlas (educational use)
This is a shared conversation. Sign in to Orris to start your own chat.