Botulism- Pediatrics
Reading File
Finding Sources
Searching PubMed
botulism pediatric infant
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have all the content needed. Here is the complete, structured answer on Botulism in Pediatrics:
Botulism - Pediatrics
Overview
Botulism is a toxin-mediated neuromuscular junction disorder caused by the neurotoxins of Clostridium botulinum (and rarely C. butyricum or C. baratii). Infant botulism is the most common form in the United States, accounting for ~77% of all reported botulism cases. The core mechanism is irreversible blockade of acetylcholine release at peripheral and autonomic neuromuscular junctions, resulting in flaccid paralysis.
Forms of Botulism
| Form | Mechanism | Age |
|---|---|---|
| Infant (intestinal toxemia) | Ingested spores germinate in the gut and produce toxin in vivo | 1 day - 12 months (peak: 1-6 months) |
| Foodborne | Preformed toxin ingested | Any age |
| Wound | Toxin produced in contaminated wound | Any age |
| Adult intestinal colonization | Same as infant form, rare | Post-GI surgery / antibiotic-altered flora |
| Iatrogenic | Therapeutic/cosmetic toxin injection | Any age |
Infant Botulism (Most Important Pediatric Form)
Pathophysiology
- Infant ingests spores (not preformed toxin) from soil/dust or honey
- Because the infant gut lacks mature competitive microbiota, spores germinate, colonize the large intestine, and produce botulinum toxin in situ
- Toxin is absorbed into the circulation and transported to peripheral cholinergic nerve terminals
- Toxin irreversibly cleaves SNARE proteins, preventing vesicular release of acetylcholine
- Recovery only occurs when new nerve terminals sprout (weeks to months)
Why infants are uniquely susceptible
- Immature intestinal microflora cannot competitively exclude C. botulinum
- Adults have established gut flora that prevents colonization
Epidemiology
- Between 2001 and 2019, 2,172 infant botulism cases were reported in the US
- Toxin serotypes: B (58%), A (40%), rarely E or F
- Rare strains producing two serotypes (A+B or B+F) have been documented
- Mortality in documented infant cases: 1-2% (with good supportive care)
- Some SIDS deaths may represent unrecognized rapidly progressive infant botulism
Sources of Spore Exposure
- Soil and household dust - now the most common identified source
- Honey - a well-established, avoidable source; honey should never be given to infants under 1 year
- Infant milk powder (rare)
- No case of infant botulism has been proven to result from corn syrup
Clinical Features
Infant Botulism Presentation
The classic presentation is the "floppy baby":
- Constipation - often the first sign (3-30 days incubation after spore ingestion)
- Poor feeding - weak suck
- Weak cry
- Loss of facial expression (cranial nerve VII palsy)
- Diminished gag reflex
- Ocular palsies - ptosis, ophthalmoplegia (diplopia if older child)
- Loss of head control
- Progressive descending, symmetric, flaccid paralysis
- Hypotonia - generalized
- Autonomic signs - dilated pupils, dry mouth, urinary retention, hyperthermia
Key features: Afebrile, alert, no sensory deficits, descending paralysis
Distinction from Myasthenia Gravis
- Botulism does affect the pupils (dilated, unreactive) - MG does not
- Botulism produces autonomic signs - MG does not
Progression
- Paralysis descends: cranial nerves → neck/shoulders → upper limbs → lower limbs
- Proximal muscle groups affected before distal
- Respiratory failure from diaphragm and accessory muscle paralysis is the life-threatening complication
Diagnosis
Clinical Basis
- Diagnosis is primarily clinical - symmetric descending flaccid paralysis, afebrile, alert
- Do not wait for lab confirmation before starting treatment
Laboratory Tests
| Test | Notes |
|---|---|
| Stool culture for C. botulinum | Preferred for infant botulism; organism detected in >90% of infant cases |
| Stool toxin assay | Mouse bioassay (toxin neutralization) or mass spectrometry; reference lab |
| Serum toxin | Toxin detected in serum of >90% of infants with botulism (vs. <60% sensitivity in foodborne) |
| If constipated - give sterile water enema | To obtain stool specimen promptly |
| EMG | Incremental response at high-frequency stimulation (20-50 Hz); brief, small, abundant motor unit potentials ("BSAP pattern") |
If suspected, contact state health department (24-hour service) immediately - they coordinate testing and antitoxin release.
Treatment
1. Supportive Care (Foundation of Management)
- Airway and respiratory support - mechanical ventilation may be required for months
- Nutritional support (NG/NJ feeds)
- Recovery takes weeks to months
2. Antitoxin - Infant Botulism (< 1 year)
BabyBIG (Human Botulism Immune Globulin IV - BIG-IV)
- FDA-licensed specifically for infant botulism caused by type A or type B
- Human-derived - eliminates serum sickness risk
- Produced and distributed by the California Department of Public Health (24-hr: 510-231-7600; infantbotulism.org)
- Significantly reduces: days of mechanical ventilation, ICU stay, and total hospital stay by ~1 month
- Cost-saving
- First-line therapy for naturally occurring infant botulism
- Delay live-virus vaccines for 6 months after BabyBIG (interference with immune response)
BAT (Heptavalent Botulinum Antitoxin - equine)
- FDA-licensed 2013 for adult and pediatric botulism
- Covers serotypes A-G
- Used for type F infant botulism (not covered by BabyBIG)
- Available through the CDC Emergency Operations Center (770-488-7100)
- "Despeciated" product (>90% Fab/F(ab')2 fragments) to reduce serum sickness
Key principle: Antitoxin ends toxemia and prevents further toxin uptake, but does NOT reverse existing paralysis - administer as early as possible.
3. Antibiotics
- Do NOT use antibiotics in infant botulism unless there is a clear concurrent infection
- Aminoglycosides are contraindicated - potentiate the paralytic effects of botulinum toxin
- For wound botulism: consider delaying antibiotics until antitoxin is given (theoretical risk of toxin release from bacterial cell lysis)
4. GI Decontamination
- If contaminated food may still be in the GI tract: enema to remove residual toxin/spores
- Cathartics/laxatives are not recommended
Differential Diagnosis of "Floppy Infant"
- Infant botulism
- Spinal muscular atrophy (SMA type 1)
- Myasthenia gravis (neonatal or congenital)
- Guillain-Barre syndrome (ascending, not descending)
- Hypotonic cerebral palsy
- Sepsis/meningoencephalitis
- Hypothyroidism
- Metabolic disorders (hypocalcemia, hypomagnesemia)
Prevention
- Never give honey to infants under 1 year of age
- No established prevention for soil/dust exposure (universal)
- No vaccine currently available for general use
- Breastfeeding does not prevent infant botulism (cases occur in breastfed infants), but breast milk may offer some protective microbiome effect
Key Summary Points for Exams
| Feature | Detail |
|---|---|
| Most common form in US | Infant botulism |
| Organism | Clostridium botulinum (anaerobic, spore-forming, gram-positive rod) |
| Toxin types in infants | A and B (>98% of cases) |
| Mechanism | Inhibits ACh release at NMJ (SNARE protein cleavage) |
| First symptom in infant | Constipation |
| Classic presentation | Floppy baby with descending flaccid paralysis, afebrile, alert |
| Key diagnostic clue | Pupil involvement (dilated, unreactive) - distinguishes from MG |
| Gold-standard lab | Stool toxin / culture (mouse bioassay) |
| Best EMG finding | Incremental response at high-frequency (20-50 Hz) stimulation |
| Antitoxin for infant | BabyBIG (human-derived, types A/B) |
| Antitoxin for other forms | BAT (equine, types A-G) |
| Antibiotic precaution | No aminoglycosides |
| Honey risk | Do not give to infants < 1 year |
| Prognosis | Mortality 1-2%; full recovery expected with supportive care |
Sources: Red Book 2021 (AAP Committee on Infectious Diseases), pp. 467-470 | Harrison's Principles of Internal Medicine 22E (2025), pp. 1277-1279 | Medical Microbiology 9e, pp. 356-357 | Tintinalli's Emergency Medicine | Rosen's Emergency Medicine
Recent literature note: A 2026 review (PMID 41964486) in Acta Paediatrica specifically addresses infant botulism and honey exposure, global epidemiology, and prevention communication strategies - consistent with the above guidance.
SSPE - Pediatrics
Reading File
Finding Sources
Finding Sources
Searching PubMed
"subacute sclerosing panencephalitis" pediatric
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have all the material needed for a comprehensive answer. Let me compile it.
Subacute Sclerosing Panencephalitis (SSPE) - Pediatrics
Definition
SSPE is a rare, fatal, chronic progressive demyelinating encephalitis of the CNS caused by persistent non-permissive infection of neurons and glial cells with a mutant measles virus. It represents a slow virus infection - the measles virus, acquired years earlier, reactivates in a defective form that cannot produce infectious particles but continues to cause progressive neural destruction.
Etiology and Pathogenesis
Causative agent: Measles virus (RNA virus, genus Morbillivirus, family Paramyxoviridae) - a defective/mutant form
Key molecular mechanism:
- After primary measles infection, the virus persists in neurons and glial cells in an intracellular, non-productive form
- Defective Matrix (M) protein and other envelope proteins are defective or absent - the virus cannot assemble and bud properly
- As a result, the virus cannot produce infectious virions - it spreads only by cell-to-cell contact
- The virus evades immune clearance by remaining intracellular
- Large numbers of viral nucleocapsids accumulate in neurons and glia
- Antibody to M protein is characteristically absent in patients' serum (unlike other measles antibodies which are markedly elevated)
- The restricted viral gene expression in differentiated brain cells is key to maintaining the persistent infection
Why measles vaccine prevents SSPE: Vaccination prevents primary measles infection, eliminating the reservoir of viral persistence. Since widespread MMR vaccination, SSPE has nearly disappeared in vaccinated populations.
Epidemiology
| Parameter | Detail |
|---|---|
| Incidence | 4-11 per 100,000 measles cases; up to ~1:1,000 in recent outbreaks |
| US cases | Average ~5 cases/year (post-vaccine era) |
| Age at diagnosis | 85% between 5 and 15 years |
| Sex | Male predominance (male:female = 3:1) |
| Latent period | Mean 7-8 years after primary measles (range 2-12 years) |
| Primary infection age | Most had measles before age 2 years (highest risk group) |
| Spontaneous remission | ~5% |
| Mortality | Fatal in virtually all cases; death within 1-3 years of onset |
Important: Risk of SSPE is highest when measles occurs in infancy (<2 years). This is a major reason for timely measles vaccination.
A 2024 review (PMID 38477320) in J Child Neurol and a 2025 review (PMID 40701692) in Semin Pediatr Neurol both warn that rising vaccine hesitancy may lead to a resurgence of SSPE cases in coming decades.
Clinical Stages
SSPE evolves through 4 classic stages (Jabbour staging):
Stage I - Behavioral/Cognitive Changes
- Declining school performance
- Personality and mood changes, temper outbursts
- Difficulty with language
- Loss of interest in usual activities
- No fever, no headache (distinguishes from acute viral encephalitis)
Stage II - Motor/Neurological
- Myoclonus - the hallmark; often bilateral, massive, shock-like jerks
- Focal or generalized seizures
- Progressive intellectual deterioration
- Ataxia
- Chorioretinitis - visual disturbances, retinal lesions
- Choreoathetoid or ballistic movements
- Spasticity begins
Stage III - Deterioration
- Optic atrophy
- Quadriparesis
- Autonomic instability
- Progressive unresponsiveness
- Akinetic mutism
Stage IV - Terminal
- Coma - child lies insensate, virtually "decorticated"
- Vegetative state
- Death (usually from intercurrent infection or autonomic failure)
Diagnosis
Clinical
- History of primary measles before age 2, followed by 6-8 year asymptomatic period
- Progressive neurological decline beginning with behavioral changes and myoclonus
- Absence of fever (key distinguishing feature)
EEG - Pathognomonic Pattern
Radermecker complexes (periodic complexes):
- Bursts of high-voltage, generalized sharp-slow wave complexes
- Occurring every 3-8 seconds (some sources: every 5-8 seconds)
- Each complex lasting up to 3 seconds
- Against a background of depressed/flat activity
- Initially only nonspecific slowing; periodic complexes appear in Stage II
- Bisynchronous (both hemispheres simultaneously)
CSF Analysis
| Parameter | Finding |
|---|---|
| Cells | Acellular (no pleocytosis) |
| Glucose | Normal |
| Total protein | Normal or mildly elevated |
| Gamma globulin | Markedly elevated (>20% of total CSF protein) |
| IgG | Elevated - predominantly antimeasles antibody |
| Oligoclonal bands | Present (measles-specific) - indicates intrathecal synthesis |
| CSF/serum antibody ratio | Elevated, consistent with high intrathecal synthesis |
Serology
- Markedly elevated measles antibody titers in both serum and CSF
- Anti-M (matrix) protein antibody is characteristically absent
- The elevated antibody paradoxically coexists with progressive disease (immune response cannot clear the infection)
MRI
- Often normal early in disease
- As disease progresses: high T2/FLAIR signal in gray matter and subcortical/periventricular white matter, beginning in posterior hemispheres
- Cortical atrophy in advanced cases
Histopathology (Brain Biopsy/Autopsy)
Macroscopic: Cerebral cortex and white matter involvement; brainstem affected; cerebellum usually spared
Microscopic:
- Eosinophilic intranuclear and intracytoplasmic inclusions in neurons and glial cells (Cowdry type A inclusions) - the histopathologic hallmark
- Destruction of nerve cells and neuronophagia
- Perivascular cuffing with lymphocytes and mononuclear cells
- Demyelination of white matter (hence "sclerosing")
- Fibrous gliosis
- Electron microscopy: viral nucleocapsids in inclusion-bearing cells
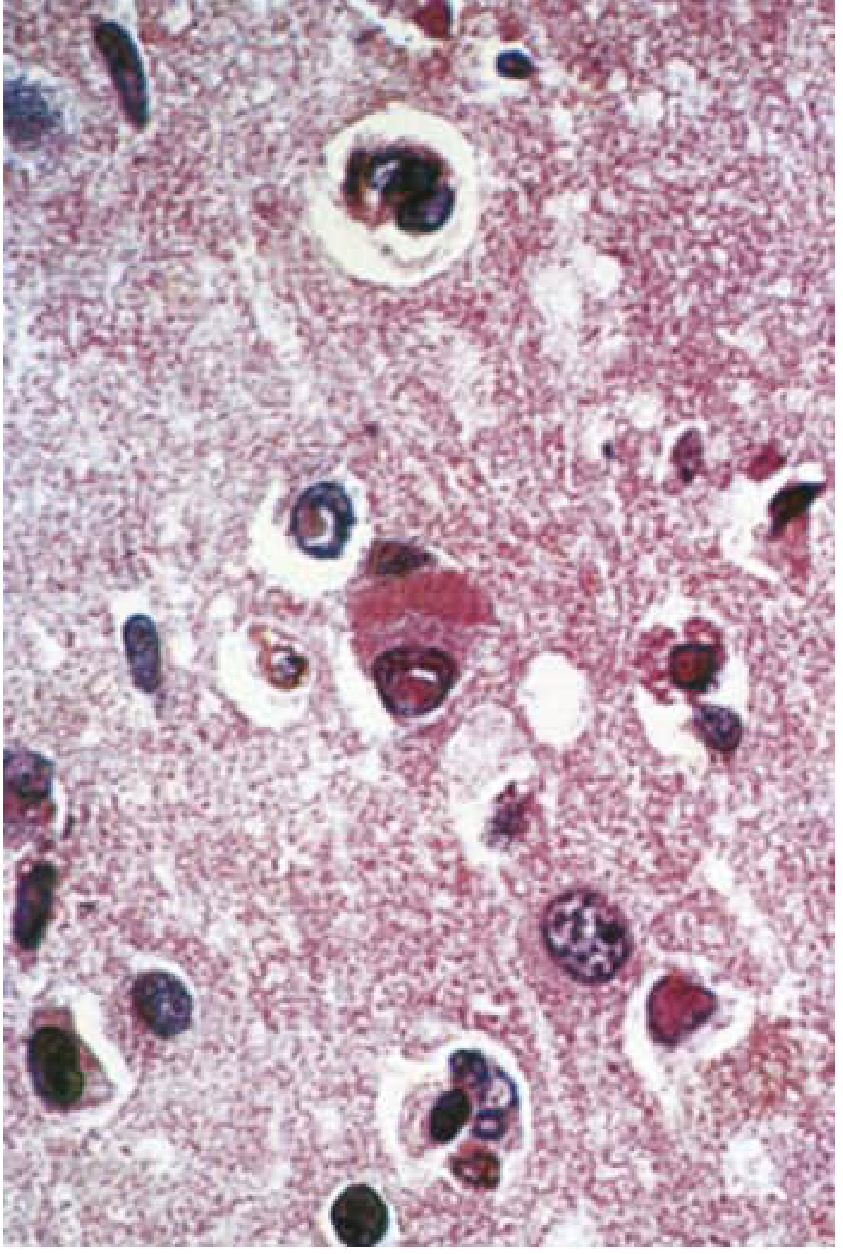
Cerebral cortex in SSPE: A pyramidal neuron with both a Cowdry-type A intranuclear inclusion and a cigar-shaped cytoplasmic inclusion. Cowdry A inclusions are also present in nuclei of nearby glial cells. (H&E stain, x350) - Bradley & Daroff's Neurology
Diagnostic Criteria (Presumptive)
The combination of:
- Periodic complexes on EEG
- Elevated CSF gamma globulin and oligoclonal bands
- Elevated measles antibody titers in serum and CSF
...is sufficient to make the diagnosis without brain biopsy in a compatible clinical setting.
Confirmatory (research/unusual cases):
- Measles virus culture from brain tissue (special cocultivation techniques)
- Viral antigen by immunocytochemistry
- Viral genome by in situ hybridization or PCR
Treatment
There is no definitive curative therapy for SSPE.
Available Treatments (Palliative/Disease-Modifying)
| Treatment | Route | Details |
|---|---|---|
| Isoprinosine (Inosiplex / inosine pranobex) | Oral | 100 mg/kg/day (max 3 g/day) in 3 divided doses; immunomodulatory and antiviral properties |
| Interferon-alfa | Intraventricular (via Ommaya reservoir) or intrathecal | Starting 100,000 U/m² body surface area/day, incrementing up to 10⁶ U/m²/day over 5 days, then 10⁶ U/m² twice weekly for 6 months |
| Combination: Isoprinosine + Intraventricular IFN-alfa | Oral + intraventricular | ~30-35% of patients show improvement or stabilization |
| Ribavirin + Intrathecal IFN-alfa | IV + intrathecal | Response reported in some cases |
| Levetiracetam | Oral | Symptomatic improvement in myoclonus and encephalopathy |
| Amantadine | Oral | Some reports of benefit; not consistently corroborated |
No treatment has been subjected to a controlled clinical trial. The laboratory endpoint of treatment is eradication of detectable measles antigen from the CSF.
Risks of interferon therapy: Meningitis, interferon-induced encephalopathy, upper and lower motor neuron toxicity.
Systemic (subcutaneous) IFN-alfa can be combined with intraventricular IFN to simultaneously treat peripheral reservoirs of measles virus in lymphoid and glandular tissue.
Supportive Care
- Anticonvulsants for seizures
- Nutritional support
- Prevention of complications (aspiration, pressure ulcers, infections)
Prevention
MMR vaccination is the only effective prevention.
- First dose at 12-15 months of age
- Second dose at 4-6 years
- MMRV (measles, mumps, rubella, varicella) is an alternative combination
- The introduction and widespread use of measles vaccine has practically eliminated SSPE in vaccinated populations
Because SSPE risk is highest in infants who get measles before age 2, timely vaccination of infants is critical. Children of vaccine-hesitant parents who contract measles are at the highest risk of developing SSPE years later.
Differential Diagnosis
| Condition | Key Differentiating Features |
|---|---|
| Lipid storage diseases (e.g., NCL, GM2) | Enzyme assays, cherry-red spot, different inclusions |
| Prion disease (CJD) | Older age, 14-3-3 protein in CSF, different EEG pattern |
| Schilder disease | Demyelination pattern, no measles antibodies |
| Progressive rubella panencephalitis | History of congenital rubella, older age at onset, no myoclonus, no periodic EEG bursts, CSF shows mild pleocytosis |
| MIBE (measles inclusion body encephalitis) | Occurs in immunocompromised patients, 1-6 months after measles (not years), no measles antibody rise |
| Autoimmune encephalitis | NMDAR/other antibodies, usually responds to immunotherapy |
| Rett syndrome | Girls only, different EEG, no measles history |
Key Summary Points for Exams
| Feature | Detail |
|---|---|
| Causative agent | Defective measles virus (mutant M protein) |
| Virus family | Paramyxoviridae, genus Morbillivirus |
| Mechanism | Non-productive CNS infection; cell-to-cell spread; defective M protein |
| Age of primary measles | Usually < 2 years |
| Latent period | 6-8 years (range 2-12 years) |
| Age at SSPE onset | 5-15 years (85% of cases) |
| Sex ratio | Male >> Female (3:1) |
| First symptoms | Behavioral change, poor school performance |
| Hallmark motor sign | Myoclonus |
| Pathognomonic EEG | Radermecker complexes - periodic high-voltage bursts every 3-8 s on flat background |
| CSF | Acellular, elevated gamma globulin, oligoclonal measles antibodies |
| Histologic hallmark | Cowdry type A inclusions in neurons and glia |
| Region spared | Cerebellum |
| Missing antibody | Anti-M protein antibody |
| Treatment | Isoprinosine ± intraventricular IFN-alfa (no cure) |
| Prevention | MMR vaccination |
| Prognosis | Invariably fatal; 1-3 years from diagnosis |
| Key prevention message | Vaccinate before age 2 - risk is highest in infants with early measles |
Sources: Bradley and Daroff's Neurology in Clinical Practice | Harrison's Principles of Internal Medicine 22E (2025) pp. 1161, 1278 | Adams and Victor's Principles of Neurology 12E, pp. 773-774 | Red Book 2021 (AAP), pp. 799 | Robbins, Cotran & Kumar Pathologic Basis of Disease | Jawetz, Melnick & Adelberg's Medical Microbiology 28E | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.