Amenorrhea
Reading File
Finding Sources
Searching PubMed
amenorrhea diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material to write a complete, well-organized response on amenorrhea. Let me compile the full answer.
Amenorrhea
Definition
Primary amenorrhea is defined as:
- Absence of menses by age 13 with no secondary sexual characteristics (no breast development), OR
- Absence of menses by age 15 in the presence of normal secondary sexual development.
Secondary amenorrhea is cessation of menses for 3 months in a woman who previously had regular cycles, or 6 months in a woman with irregular cycles.
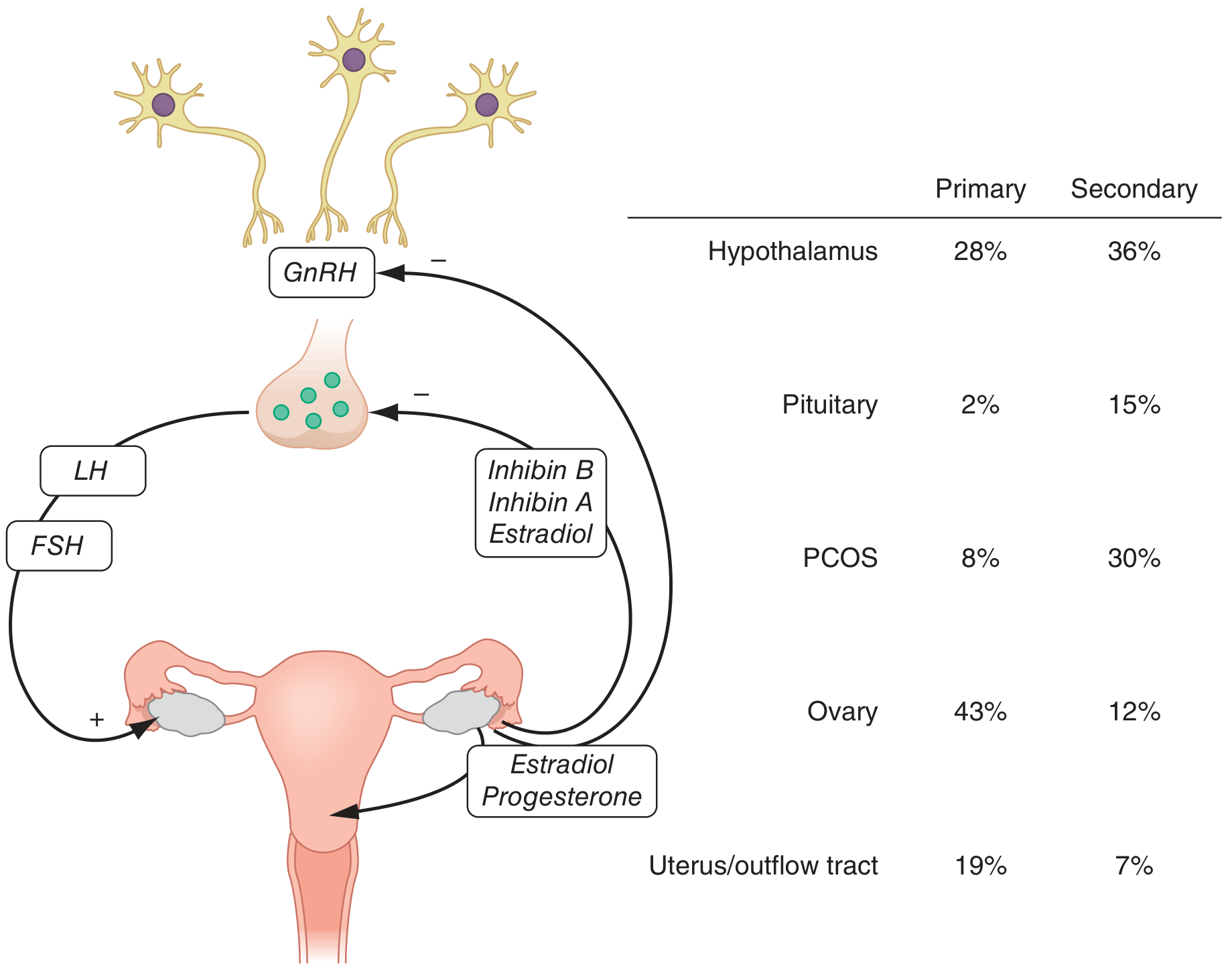
Physiology
Normal menstruation depends on an intact hypothalamic-pituitary-ovarian-uterine axis. The hypothalamus secretes GnRH in a pulsatile fashion, which stimulates pituitary secretion of FSH and LH. These stimulate ovarian folliculogenesis and steroidogenesis. Estradiol and progesterone drive endometrial growth and shedding, and provide negative feedback to the hypothalamus and pituitary. Disruption at any level produces amenorrhea.
Classification and Etiology
Amenorrhea is best approached by categorizing it anatomically.
1. Outflow Tract / Uterine Causes
| Condition | Type | Notes |
|---|---|---|
| Imperforate hymen | Primary | Cyclic pain + hematocolpos |
| Transverse vaginal septum | Primary | Similar to hymen |
| Congenital vaginal atresia | Primary | |
| Mullerian agenesis (MRKH syndrome) | Primary | Normal 46,XX; uterus/vagina absent; ovaries normal; caused by WNT4 mutations |
| Androgen Insensitivity Syndrome (AIS) | Primary | 46,XY; female external genitalia; absent/sparse pubic/axillary hair; testes present; accounts for ~10% of primary amenorrhea |
| Asherman syndrome | Secondary | Post-traumatic intrauterine synechiae; curettage accounts for >90%; TB endemic cause |
| Cervical stenosis | Secondary | Post-procedure |
2. Ovarian Causes (Hypergonadotropic Hypogonadism)
| Condition | Type | Notes |
|---|---|---|
| Turner syndrome (45,X) | Primary | Most common; streak ovaries; stigmata: short stature, webbed neck, shield chest, cubitus valgus, short 4th metacarpal |
| Other gonadal dysgenesis (46,XX, 46,XY) | Primary | Elevated FSH/LH |
| Mosaic karyotypes | Primary/Secondary | Occasional estrogen, rare ovulation possible |
| Primary ovarian insufficiency (POI) | Secondary | FSH >25-40 mIU/mL x2 samples; idiopathic, autoimmune, chemo, radiation |
| PCOS | Primary or Secondary | Hyperandrogenism, oligo-anovulation |
| Ovarian tumor | Secondary | Rare |
| Resistant ovary syndrome | Primary/Secondary |
3. Pituitary Causes (Hypogonadotropic Hypogonadism)
| Condition | Type | Notes |
|---|---|---|
| Hyperprolactinemia | Secondary | Prolactinoma most common; also drugs |
| Sheehan syndrome | Secondary | Postpartum pituitary necrosis |
| Lymphocytic hypophysitis | Secondary | |
| Acquired hypopituitarism | Secondary | Trauma, tumor, irradiation |
| Cushing disease | Secondary |
4. Hypothalamic Causes (Hypogonadotropic Hypogonadism)
| Condition | Type | Notes |
|---|---|---|
| Functional hypothalamic amenorrhea (FHA) | Secondary | Caloric restriction, excess exercise, psychological stress; increased CRH suppresses GnRH |
| Kallmann syndrome | Primary | IHH + anosmia; ~50% genetic cause; 3x more common in males |
| Isolated hypogonadotropic hypogonadism | Primary | No anosmia; ~50% of patients have some breast development |
| Tumor/infiltrative disease | Either | Craniopharyngioma, sarcoid, histiocytosis |
5. Other Endocrine / Systemic Causes
| Cause | Mechanism |
|---|---|
| Hypothyroidism | Elevated TSH → elevated TRH → elevated prolactin → anovulation |
| Hyperthyroidism | Altered sex hormone binding globulin, disrupted feedback |
| Adrenal: Cushing, CAH, virilizing tumor | Androgen excess → disrupted HPO axis |
| Late-onset CAH (21-hydroxylase deficiency) | Excess androgens |
| Eating disorders (anorexia nervosa) | Combined nutritional, stress, weight-loss mechanism |
6. Iatrogenic Causes
| Drug | Mechanism |
|---|---|
| Antipsychotics (haloperidol, risperidone, clozapine) | Dopamine blockade → hyperprolactinemia |
| Tricyclic antidepressants / MAOIs | Increased prolactin |
| Antihypertensives (methyldopa, reserpine, Ca-channel blockers) | Dopamine depletion → prolactin elevation |
| Chemotherapy (busulfan, chlorambucil) | Ovarian toxicity |
| OCP / progestational agents | Hormonal suppression |
| Marijuana, digitalis | Estrogenic activity |
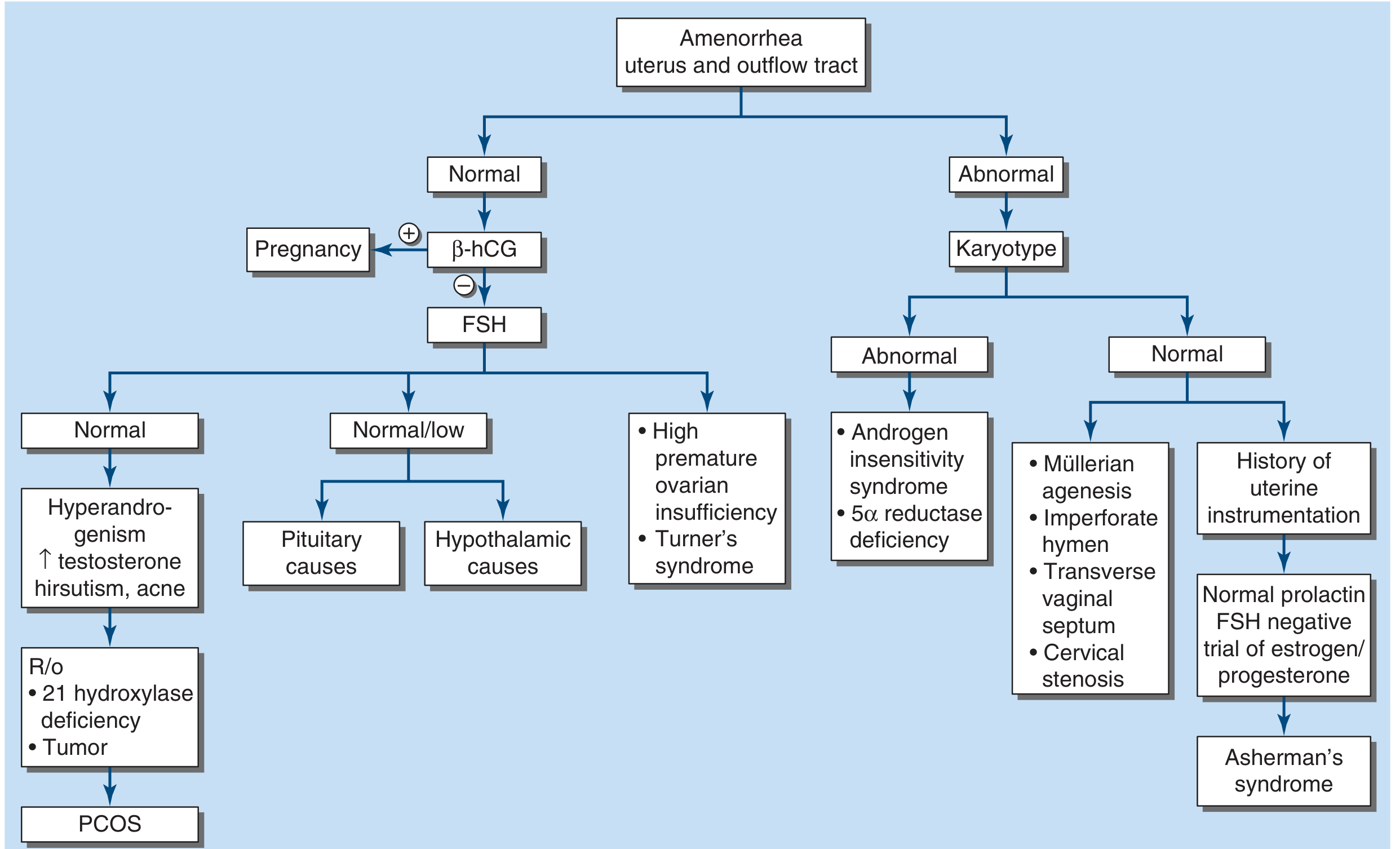
Evaluation
Step 1 - Establish the Type and Do a Pregnancy Test
A urine/serum beta-hCG must be performed first in all reproductive-age women - pregnancy is the most common cause of secondary amenorrhea.
Step 2 - Physical Examination
- Presence or absence of secondary sexual characteristics (breast development, pubic/axillary hair) - key to categorizing primary amenorrhea
- Pelvic anatomy - normal vs. abnormal (outflow tract defects, imperforate hymen)
- Signs of hyperandrogenism (acne, hirsutism, clitoromegaly)
- Signs of Turner syndrome, or other syndromic features
- Galactorrhea (suggests hyperprolactinemia)
Step 3 - Initial Laboratory Work-Up (in patient with normal anatomy and normal secondary sexual characteristics)
- Serum TSH - exclude thyroid disorders
- Serum prolactin - obtain fasting, no recent breast stimulation, in follicular phase if cycles exist
- Serum FSH (with estradiol) - key test to distinguish ovarian from central cause
- Consider vaginal ultrasound for antral follicle count (PCOS vs. POI)
- If prolactin elevated or hypothalamic amenorrhea suspected: MRI of sella/hypothalamus
Step 4 - Interpret FSH
| FSH Level | Interpretation | Likely Causes |
|---|---|---|
| High (>25-40 mIU/mL on 2 samples) | Hypergonadotropic hypogonadism | POI, Turner, gonadal dysgenesis |
| Normal/Low | Hypogonadotropic or eugonadotropic | FHA, pituitary tumor/disease, PCOS, hypothalamic lesion |
| Normal + hyperandrogenism | Eugonadotropic | PCOS, CAH, androgen-secreting tumor |
Step 5 - Additional Tests Based on Findings
- If POI confirmed: FMR1 premutation, karyotype, 21-hydroxylase antibody
- If PCOS suspected: Total testosterone, SHBG, 17-hydroxyprogesterone (to exclude CAH)
- If PCOS confirmed: Fasting glucose, lipid profile
- AMH: Low in POI, high in PCOS; undetectable years before final menses in POI
- Karyotype: Perform in primary amenorrhea with gonadal failure (~30% have abnormal karyotype); consider in all POI regardless of age
- DEXA scan: For suspected long-term hypoestrogenism (bone density)
Treatment
Outflow Tract Obstruction
- Imperforate hymen or vaginal septum: surgical correction - must be done promptly to prevent endometriosis from retrograde flow
- Mullerian agenesis: Vaginal dilation (first-line); surgical creation of neovagina if needed; ovaries are normal so surrogacy/uterine transplant can enable pregnancy
- AIS: Gonadectomy (after pubertal development to allow breast development and growth spurt) + estrogen replacement + possible vaginal dilation
- Asherman syndrome: Hysteroscopic lysis of adhesions + post-op estrogen to stimulate re-epithelialization
Ovarian Insufficiency / Hypergonadotropic Hypogonadism
- Hormone replacement therapy (HRT): Estrogen + progesterone to restore estrogen levels, protect bone (prevent osteoporosis), and provide cycle control
- Fertility: Oocyte donation is the most effective option; spontaneous pregnancy can rarely occur in POI
- Y-chromosome containing gonadal material: Gonadectomy to prevent gonadoblastoma
Functional Hypothalamic Amenorrhea
- Address the underlying cause: nutritional rehabilitation (weight gain), reduce exercise intensity, stress management, cognitive behavioral therapy (CBT)
- Estrogen replacement / OCP for bone protection while addressing root cause
- Pulsatile GnRH or gonadotropins if fertility is desired and lifestyle modifications insufficient
Hyperprolactinemia
- Dopamine agonists (cabergoline, bromocriptine) - first-line for prolactinoma and hyperprolactinemia-induced amenorrhea
- Surgery for resistant macroprolactinomas
PCOS
- Combined OCPs for cycle regulation and hyperandrogenism control
- Metformin for insulin resistance/metabolic features
- Ovulation induction (letrozole, clomiphene, or gonadotropins) for fertility
Hypothyroidism / Hyperthyroidism
- Thyroid hormone replacement or anti-thyroid therapy - menses typically resume with euthyroid state
Key Clinical Points
- Absent menses may indicate a systemic medical condition with implications beyond fertility - always establish a cause.
- When gonadal failure accompanies primary amenorrhea, karyotypic abnormality is present in ~30% of cases.
- The most important diagnostic elements are: physical exam for secondary sexual characteristics and anatomy, beta-hCG, prolactin, TSH, and FSH.
- The progestogen challenge test has poor sensitivity and specificity and is no longer routinely recommended to assess estrogen status.
- Long-term hypoestrogenism from any cause increases fracture risk - bone mineral density assessment (DEXA) should be considered.
- Functional hypothalamic amenorrhea is a diagnosis of exclusion after ruling out organic causes.
Sources: Harrison's Principles of Internal Medicine 22E, p. 3176-3178; Berek & Novak's Gynecology, pp. 1855-1890; Tietz Textbook of Laboratory Medicine 7th Ed., pp. 2353-2490; Goldman-Cecil Medicine, p. 1677
Abnormal Uterine Bleeding in short Refer DC Datta
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I have enough material for a concise, well-structured answer. Note: DC Datta's textbook is not available in the library, but I'll present content aligned with the standard teaching in DC Datta's style (definitions, patterns, PALM-COEIN classification, evaluation, management) and flag this clearly.
Abnormal Uterine Bleeding (AUB)
Note: DC Datta's Textbook of Gynecology is not in this library's collection. The following is based on Goldman-Cecil Medicine, Berek & Novak's Gynecology, and Rosen's Emergency Medicine - the content closely aligns with DC Datta's standard teaching on this topic.
Definition
AUB is any bleeding from the uterine corpus that is abnormal in regularity, frequency, duration, or volume and that occurs in the absence of pregnancy.
Normal menstrual parameters (for reference):
| Parameter | Normal Range |
|---|---|
| Frequency | 24-38 days |
| Duration | 4-8 days |
| Volume | 5-80 mL per cycle |
Terminology (FIGO 2011)
Old terms like DUB (Dysfunctional Uterine Bleeding), menorrhagia, metrorrhagia have been replaced by descriptive terms:
| Term | Meaning |
|---|---|
| Heavy Menstrual Bleeding (HMB) | Excessive volume interfering with quality of life |
| Intermenstrual Bleeding (IMB) | Bleeding between regular cycles |
| Irregular Menstrual Bleeding | Unpredictable timing |
| Prolonged Menstrual Bleeding | Duration >8 days |
PALM-COEIN Classification (FIGO)
The standard classification divides causes into structural (PALM) and non-structural (COEIN):
PALM - Structural Causes
| Cause | Key Features | |
|---|---|---|
| P | Polyp (AUB-P) | Endometrial/endocervical; IMB, postcoital bleeding |
| A | Adenomyosis (AUB-A) | Endometrial glands in myometrium; HMB + dysmenorrhea; bulky tender uterus |
| L | Leiomyoma (AUB-L) | Submucosal (AUB-LSM) causes most bleeding; other types (AUB-LO) less so |
| M | Malignancy & Hyperplasia (AUB-M) | Endometrial carcinoma/atypical hyperplasia; must exclude in all postmenopausal AUB |
COEIN - Non-Structural Causes
| Cause | Key Features | |
|---|---|---|
| C | Coagulopathy (AUB-C) | vWD, ITP, anticoagulant use; heavy flow since menarche |
| O | Ovulatory Dysfunction (AUB-O) | Most common - anovulation from PCOS, thyroid, hyperprolactinemia, perimenopause, adolescence |
| E | Endometrial (AUB-E) | Primary endometrial disorder; abnormal local hemostasis |
| I | Iatrogenic (AUB-I) | Hormonal contraceptives, anticoagulants, antipsychotics |
| N | Not yet classified (AUB-N) | Rare/poorly defined entities |
Epidemiology
- AUB affects 10-30% of women of reproductive age
- ~20% is postmenarchal (adolescent) - due to HPO axis immaturity → anovulation
- ~50% is perimenopausal - incipient ovarian failure
- ~75% of cases have no organic cause - i.e., anovulatory/dysfunctional bleeding
Pathophysiology of Anovulatory Bleeding
In anovulation, unopposed estrogen continuously stimulates the endometrium without the stabilizing effect of progesterone:
- Endometrium proliferates and thickens irregularly
- Unsynchronized shedding → irregular, unpredictable, often heavy bleeding
- Estrogen withdrawal bleeding (when estrogen drops)
- Estrogen breakthrough bleeding (from continuously high estrogen)
Evaluation / Diagnosis
History
- Pattern, duration, quantity of bleeding; clots; flooding
- LMP, sexual history, contraceptive use
- Symptoms of thyroid disease, PCOS, coagulopathy
- Drug history (anticoagulants, OCP, antipsychotics)
Examination
- General: pallor, signs of anaemia, thyroid enlargement, hirsutism
- Pelvic: uterine size, tenderness, adnexal masses; speculum for cervical/vaginal cause
- Exclude pregnancy first (beta-hCG)
Investigations
| Test | Purpose |
|---|---|
| Beta-hCG | Exclude pregnancy (first step always) |
| CBC + platelets | Anaemia; thrombocytopenia |
| Coagulation profile (PT, aPTT, vWF) | Exclude coagulopathy |
| TSH | Thyroid dysfunction |
| Fasting glucose | PCOS-related insulin resistance |
| Prolactin, FSH, LH | Anovulatory causes |
| Testosterone, DHEA-S | Hyperandrogenism |
| Transvaginal ultrasound (TVUS) | Polyps, fibroids, endometrial thickness |
| Endometrial biopsy / D&C | Women >35 years, risk factors for endometrial cancer, or failed medical treatment |
| Hysteroscopy | Gold standard to visualize endometrial cavity; directed biopsy |
| SIS (Saline Infusion Sonography) | Better detection of intracavitary lesions |
Endometrial sampling is mandatory in women >35 years or those with prolonged anovulatory bleeding, due to risk of endometrial carcinoma.
Management
Acute / Emergency (Haemodynamically Unstable)
- IV fluids, blood transfusion if needed
- IV conjugated estrogen 25 mg every 4-6 hours (until bleeding stops)
- Intrauterine Foley tamponade (26Fr, 30 mL saline) as temporizing measure
- Surgical: urgent D&C, uterine artery embolization (UAE), endometrial ablation, or hysterectomy
Medical (Outpatient / Subacute)
Hormonal:
| Drug | Dose / Route | Notes |
|---|---|---|
| Combined OCP | 1 tablet every 6 hours x 5-7 days (acute); then cyclic | First-line for anovulatory AUB; bleeding stops within 24 hours |
| Progestins (MPA, norethindrone) | MPA 5-10 mg x 10 days; norethindrone 5 mg TDS x 7 days | For women with estrogen contraindications |
| Levonorgestrel IUD (Mirena) | Intrauterine | Excellent for HMB long-term; reduces flow by >90% |
| GnRH agonists | Monthly injection | Fibroid-related AUB; pre-operative use |
| Relugolix / Elagolix | Oral GnRH antagonists | For fibroid/adenomyosis-related bleeding |
Non-Hormonal:
| Drug | Dose | Mechanism |
|---|---|---|
| Tranexamic acid | 1.3 g PO TDS x 5 days OR 10 mg/kg IV | Antifibrinolytic; reduces HMB by ~50% |
| NSAIDs (mefenamic acid, ibuprofen) | Start before menses | Reduces prostaglandins; modest effect on flow |
| Desmopressin | For vWD-related AUB |
Surgical
| Procedure | Indication |
|---|---|
| D&C (dilatation & curettage) | Diagnostic + acute control; not long-term solution alone |
| Hysteroscopic polypectomy/myomectomy | Structural causes (polyps, submucosal fibroids) |
| Endometrial ablation | Persistent AUB with completed family; not 100% effective |
| UAE | Symptomatic fibroids; preserve uterus |
| Myomectomy | Fibroids; fertility desired |
| Hysterectomy | Refractory/recurrent AUB; family complete; malignancy |
Special Age Groups
| Age Group | Commonest Cause | Approach |
|---|---|---|
| Adolescent | Anovulation (HPO axis immaturity) | Exclude coagulopathy; OCP/progestins |
| Reproductive age | PCOS, polyp, fibroid, pregnancy complication | PALM-COEIN workup |
| Perimenopausal | Anovulation (incipient ovarian failure) | Exclude endometrial pathology; hormonal |
| Postmenopausal | Endometrial atrophy (most common); carcinoma | Endometrial biopsy mandatory |
Sources: Goldman-Cecil Medicine International Edition; Rosen's Emergency Medicine 9e; Berek & Novak's Gynecology. DC Datta's Textbook of Gynecology was not available in the library - content presented follows the same standard framework.
Generate a quick reference PDF for PALM-COEIN classification
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace
Running Command
mkdir -p /home/daytona/workspace/palm-coein && python3 -c "from reportlab.lib.pa…
Writing File
~/palm-coein/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm, cm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import FrameBreak
OUTPUT = "/home/daytona/workspace/palm-coein/PALM_COEIN_Quick_Reference.pdf"
# ── Colour palette ────────────────────────────────────────────────────────────
DARK_BLUE = colors.HexColor("#1a3c5e")
PALM_COLOR = colors.HexColor("#c0392b") # red for PALM
COEIN_COLOR = colors.HexColor("#1a6b3e") # green for COEIN
LIGHT_RED = colors.HexColor("#fdecea")
LIGHT_GREEN = colors.HexColor("#e8f5e9")
LIGHT_BLUE = colors.HexColor("#e8f0fe")
GOLD = colors.HexColor("#d4a017")
GREY_BG = colors.HexColor("#f4f6f9")
MID_GREY = colors.HexColor("#7f8c8d")
WHITE = colors.white
BLACK = colors.HexColor("#1c1c1c")
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=15*mm, leftMargin=15*mm,
topMargin=15*mm, bottomMargin=15*mm,
title="PALM-COEIN Classification – Quick Reference",
author="Orris Medical Reference"
)
W, H = A4
COL = W - 30*mm # usable width
styles = getSampleStyleSheet()
def style(name, **kw):
return ParagraphStyle(name, **kw)
# ── Custom styles ─────────────────────────────────────────────────────────────
TITLE_S = style("Title_S", fontSize=22, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_CENTER,
leading=28, spaceAfter=2)
SUB_S = style("Sub_S", fontSize=11, textColor=colors.HexColor("#cfe2ff"),
fontName="Helvetica", alignment=TA_CENTER, leading=14)
FOOT_S = style("Foot_S", fontSize=7.5, textColor=MID_GREY,
fontName="Helvetica-Oblique", alignment=TA_CENTER)
SEC_HDR = style("SecHdr", fontSize=13, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_CENTER,
leading=16)
CELL_HDR= style("CellHdr", fontSize=9.5, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=12)
CELL_TXT= style("CellTxt", fontSize=8.5, textColor=BLACK,
fontName="Helvetica", leading=11, alignment=TA_LEFT)
CELL_KEY= style("CellKey", fontSize=9, textColor=BLACK,
fontName="Helvetica-Bold", leading=12, alignment=TA_LEFT)
BODY_S = style("Body_S", fontSize=8.5, textColor=BLACK,
fontName="Helvetica", leading=12, alignment=TA_JUSTIFY)
BOLD_S = style("Bold_S", fontSize=8.5, textColor=BLACK,
fontName="Helvetica-Bold", leading=12)
NOTE_S = style("Note_S", fontSize=8, textColor=MID_GREY,
fontName="Helvetica-Oblique", leading=11)
PILL_S = style("Pill_S", fontSize=9, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=11)
story = []
# ══════════════════════════════════════════════════════════════════════════════
# HEADER BANNER
# ══════════════════════════════════════════════════════════════════════════════
header_data = [[
Paragraph("<b>PALM-COEIN</b>", TITLE_S),
]]
header_table = Table(header_data, colWidths=[COL])
header_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), DARK_BLUE),
("TOPPADDING", (0,0), (-1,-1), 12),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
("ROUNDEDCORNERS",(0,0), (-1,-1), [6,6,0,0]),
]))
story.append(header_table)
sub_data = [[
Paragraph("Classification of Abnormal Uterine Bleeding (AUB) — FIGO 2011", SUB_S),
]]
sub_table = Table(sub_data, colWidths=[COL])
sub_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), colors.HexColor("#2c5282")),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 10),
("ROUNDEDCORNERS",(0,0), (-1,-1), [0,0,6,6]),
]))
story.append(sub_table)
story.append(Spacer(1, 8))
# ── Definition box ─────────────────────────────────────────────────────────
def_data = [[
Paragraph(
"<b>AUB</b> = Any uterine bleeding that is abnormal in <b>regularity, frequency, "
"duration, or volume</b> in the absence of pregnancy.",
BODY_S)
]]
def_table = Table(def_data, colWidths=[COL])
def_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LIGHT_BLUE),
("BOX", (0,0), (-1,-1), 0.8, DARK_BLUE),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING", (0,0), (-1,-1), 7),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
("ROUNDEDCORNERS",(0,0), (-1,-1), [4,4,4,4]),
]))
story.append(def_table)
story.append(Spacer(1, 10))
# ══════════════════════════════════════════════════════════════════════════════
# PALM — STRUCTURAL CAUSES
# ══════════════════════════════════════════════════════════════════════════════
palm_hdr = Table([[Paragraph("PALM — Structural Causes", SEC_HDR)]], colWidths=[COL])
palm_hdr.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), PALM_COLOR),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("ROUNDEDCORNERS",(0,0), (-1,-1), [6,6,0,0]),
]))
story.append(palm_hdr)
palm_col_w = [12*mm, 28*mm, 35*mm, 50*mm, COL - 12*mm - 28*mm - 35*mm - 50*mm]
palm_rows = [
# header
[
Paragraph("Code", CELL_HDR),
Paragraph("Category", CELL_HDR),
Paragraph("Pathology", CELL_HDR),
Paragraph("Clinical Features", CELL_HDR),
Paragraph("Investigation", CELL_HDR),
],
# P
[
Paragraph("<b>P</b>", style("PL", fontSize=16, textColor=PALM_COLOR,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=18)),
Paragraph("<b>Polyp</b>\n(AUB-P)", CELL_KEY),
Paragraph("Endometrial or endocervical epithelial overgrowth", CELL_TXT),
Paragraph("• Intermenstrual bleeding (IMB)\n• Postcoital bleeding\n• Variable flow", CELL_TXT),
Paragraph("TVUS / SIS\nHysteroscopy", CELL_TXT),
],
# A
[
Paragraph("<b>A</b>", style("AL", fontSize=16, textColor=PALM_COLOR,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=18)),
Paragraph("<b>Adenomyosis</b>\n(AUB-A)", CELL_KEY),
Paragraph("Endometrial glands + stroma within myometrium", CELL_TXT),
Paragraph("• Heavy menstrual bleeding (HMB)\n• Dysmenorrhea\n• Bulky, tender uterus", CELL_TXT),
Paragraph("TVUS / MRI", CELL_TXT),
],
# L
[
Paragraph("<b>L</b>", style("LL", fontSize=16, textColor=PALM_COLOR,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=18)),
Paragraph("<b>Leiomyoma</b>\n(AUB-L)\n\nSubmucosal → AUB-LSM\nOther → AUB-LO", CELL_KEY),
Paragraph("Benign smooth muscle tumour; submucosal type most likely to cause AUB", CELL_TXT),
Paragraph("• HMB, prolonged bleeding\n• Pelvic pressure/bulk\n• Irregular uterus on exam", CELL_TXT),
Paragraph("TVUS / SIS\nMRI for mapping", CELL_TXT),
],
# M
[
Paragraph("<b>M</b>", style("ML", fontSize=16, textColor=PALM_COLOR,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=18)),
Paragraph("<b>Malignancy &\nHyperplasia</b>\n(AUB-M)", CELL_KEY),
Paragraph("Endometrial carcinoma; atypical hyperplasia; cervical/other malignancy", CELL_TXT),
Paragraph("• Postmenopausal bleeding\n• Irregular, painless bleeding\n• Risk: obesity, nulliparity, unopposed estrogen", CELL_TXT),
Paragraph("Endometrial biopsy\nD&C\nHysteroscopy\nMRI staging", CELL_TXT),
],
]
palm_table = Table(palm_rows, colWidths=palm_col_w, repeatRows=1)
palm_table.setStyle(TableStyle([
# header row
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#8b1a10")),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
# alternating rows
("BACKGROUND", (0,1), (-1,1), LIGHT_RED),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), LIGHT_RED),
("BACKGROUND", (0,4), (-1,4), WHITE),
# grid
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#e0b0b0")),
("BOX", (0,0), (-1,-1), 0.8, PALM_COLOR),
# padding
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("ALIGN", (0,0), (0,-1), "CENTER"),
("ROUNDEDCORNERS",(0,0), (-1,-1), [0,0,6,6]),
]))
story.append(palm_table)
story.append(Spacer(1, 10))
# ══════════════════════════════════════════════════════════════════════════════
# COEIN — NON-STRUCTURAL CAUSES
# ══════════════════════════════════════════════════════════════════════════════
coein_hdr = Table([[Paragraph("COEIN — Non-Structural Causes", SEC_HDR)]], colWidths=[COL])
coein_hdr.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), COEIN_COLOR),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("ROUNDEDCORNERS",(0,0), (-1,-1), [6,6,0,0]),
]))
story.append(coein_hdr)
coein_col_w = [12*mm, 30*mm, 38*mm, 48*mm, COL - 12*mm - 30*mm - 38*mm - 48*mm]
coein_rows = [
[
Paragraph("Code", CELL_HDR),
Paragraph("Category", CELL_HDR),
Paragraph("Mechanism", CELL_HDR),
Paragraph("Clinical Features", CELL_HDR),
Paragraph("Key Tests", CELL_HDR),
],
# C
[
Paragraph("<b>C</b>", style("CL", fontSize=16, textColor=COEIN_COLOR,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=18)),
Paragraph("<b>Coagulopathy</b>\n(AUB-C)", CELL_KEY),
Paragraph("vWD, ITP, anticoagulant therapy, liver disease", CELL_TXT),
Paragraph("• HMB since menarche\n• Easy bruising, prolonged bleeding\n• Family history of bleeding", CELL_TXT),
Paragraph("PT, aPTT\nvWF antigen\nPlatelet count", CELL_TXT),
],
# O
[
Paragraph("<b>O</b>", style("OL", fontSize=16, textColor=COEIN_COLOR,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=18)),
Paragraph("<b>Ovulatory\nDysfunction</b>\n(AUB-O)", CELL_KEY),
Paragraph("Anovulation → unopposed estrogen\nCauses: PCOS, thyroid, hyperprolactinemia, perimenopause, adolescence", CELL_TXT),
Paragraph("• Irregular, unpredictable bleeding\n• May be heavy or light\n• Intermenstrual bleeding", CELL_TXT),
Paragraph("TSH, Prolactin\nFSH, LH\nTestosterone\nTVUS", CELL_TXT),
],
# E
[
Paragraph("<b>E</b>", style("EL", fontSize=16, textColor=COEIN_COLOR,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=18)),
Paragraph("<b>Endometrial</b>\n(AUB-E)", CELL_KEY),
Paragraph("Primary endometrial disorder; abnormal local haemostasis (↓ vasoconstrictors, ↑ fibrinolysis)", CELL_TXT),
Paragraph("• Regular cycles but HMB\n• No structural cause found\n• Normal ovulation", CELL_TXT),
Paragraph("Endometrial biopsy\nHysteroscopy\n(diagnosis of exclusion)", CELL_TXT),
],
# I
[
Paragraph("<b>I</b>", style("IL", fontSize=16, textColor=COEIN_COLOR,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=18)),
Paragraph("<b>Iatrogenic</b>\n(AUB-I)", CELL_KEY),
Paragraph("Hormonal contraceptives, IUDs, anticoagulants, antipsychotics (→ hyperprolactinemia)", CELL_TXT),
Paragraph("• Breakthrough bleeding on OCP\n• Irregular bleeding on progestin-only\n• Drug history positive", CELL_TXT),
Paragraph("Drug history\nProlactin if on antipsychotics", CELL_TXT),
],
# N
[
Paragraph("<b>N</b>", style("NL", fontSize=16, textColor=COEIN_COLOR,
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=18)),
Paragraph("<b>Not Yet\nClassified</b>\n(AUB-N)", CELL_KEY),
Paragraph("Rare / poorly defined entities not fitting other categories", CELL_TXT),
Paragraph("• Arteriovenous malformations\n• Myometrial hypertrophy\n• Endometritis (rare)", CELL_TXT),
Paragraph("Case-dependent\nspecialist workup", CELL_TXT),
],
]
coein_table = Table(coein_rows, colWidths=coein_col_w, repeatRows=1)
coein_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#145232")),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
("BACKGROUND", (0,1), (-1,1), LIGHT_GREEN),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), LIGHT_GREEN),
("BACKGROUND", (0,4), (-1,4), WHITE),
("BACKGROUND", (0,5), (-1,5), LIGHT_GREEN),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#a8d5b5")),
("BOX", (0,0), (-1,-1), 0.8, COEIN_COLOR),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("ALIGN", (0,0), (0,-1), "CENTER"),
("ROUNDEDCORNERS",(0,0), (-1,-1), [0,0,6,6]),
]))
story.append(coein_table)
story.append(Spacer(1, 10))
# ══════════════════════════════════════════════════════════════════════════════
# NORMAL MENSTRUAL PARAMETERS + MANAGEMENT OVERVIEW (side by side)
# ══════════════════════════════════════════════════════════════════════════════
half = (COL - 6*mm) / 2
# --- Normal Parameters ---
norm_title = Table([[Paragraph("Normal Menstrual Parameters", style("NT",
fontSize=9.5, textColor=WHITE, fontName="Helvetica-Bold",
alignment=TA_CENTER, leading=12))]],
colWidths=[half])
norm_title.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), DARK_BLUE),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("ROUNDEDCORNERS",(0,0), (-1,-1), [4,4,0,0]),
]))
norm_rows = [
[Paragraph("<b>Parameter</b>", CELL_HDR), Paragraph("<b>Normal Range</b>", CELL_HDR)],
[Paragraph("Frequency", CELL_TXT), Paragraph("Every 24–38 days", CELL_TXT)],
[Paragraph("Duration", CELL_TXT), Paragraph("4–8 days", CELL_TXT)],
[Paragraph("Volume", CELL_TXT), Paragraph("5–80 mL per cycle", CELL_TXT)],
[Paragraph("Regularity",CELL_TXT), Paragraph("Variation ≤7-9 days cycle-to-cycle", CELL_TXT)],
]
norm_table = Table(norm_rows, colWidths=[half*0.5, half*0.5])
norm_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#34495e")),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("BACKGROUND", (0,1), (-1,1), GREY_BG),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), GREY_BG),
("BACKGROUND", (0,4), (-1,4), WHITE),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#bdc3c7")),
("BOX", (0,0), (-1,-1), 0.8, DARK_BLUE),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("ROUNDEDCORNERS",(0,0), (-1,-1), [0,0,4,4]),
]))
# --- Management Summary ---
mgmt_title = Table([[Paragraph("Management Overview", style("MT",
fontSize=9.5, textColor=WHITE, fontName="Helvetica-Bold",
alignment=TA_CENTER, leading=12))]],
colWidths=[half])
mgmt_title.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), colors.HexColor("#6b2d8b")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("ROUNDEDCORNERS",(0,0), (-1,-1), [4,4,0,0]),
]))
mgmt_rows = [
[Paragraph("<b>Situation</b>", CELL_HDR), Paragraph("<b>First-line Treatment</b>", CELL_HDR)],
[Paragraph("Acute / haemodynamic instability", CELL_TXT),
Paragraph("IV conj. estrogen 25 mg q4-6h; D&C; UAE", CELL_TXT)],
[Paragraph("Anovulatory (stable)", CELL_TXT),
Paragraph("Combined OCP 1 tab q6h × 5–7 days, then cyclic", CELL_TXT)],
[Paragraph("HMB (non-structural)", CELL_TXT),
Paragraph("Tranexamic acid 1.3 g TDS × 5 days; LNG-IUD", CELL_TXT)],
[Paragraph("Structural cause (fibroid/polyp)", CELL_TXT),
Paragraph("Hysteroscopic resection; myomectomy; UAE", CELL_TXT)],
[Paragraph("Postmenopausal AUB", CELL_TXT),
Paragraph("Endometrial biopsy FIRST; treat cause", CELL_TXT)],
[Paragraph("Refractory / family complete", CELL_TXT),
Paragraph("Endometrial ablation; hysterectomy", CELL_TXT)],
]
mgmt_table = Table(mgmt_rows, colWidths=[half*0.52, half*0.48])
mgmt_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#4a1a6b")),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("BACKGROUND", (0,1), (-1,1), colors.HexColor("#f3e8ff")),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), colors.HexColor("#f3e8ff")),
("BACKGROUND", (0,4), (-1,4), WHITE),
("BACKGROUND", (0,5), (-1,5), colors.HexColor("#f3e8ff")),
("BACKGROUND", (0,6), (-1,6), WHITE),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#d8b4fe")),
("BOX", (0,0), (-1,-1), 0.8, colors.HexColor("#6b2d8b")),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("ROUNDEDCORNERS",(0,0), (-1,-1), [0,0,4,4]),
]))
# combine left/right
norm_block = [norm_title, norm_table]
mgmt_block = [mgmt_title, mgmt_table]
from reportlab.platypus import BalancedColumns
side_data = [[norm_title, Spacer(6,1), mgmt_title],
[norm_table, Spacer(6,1), mgmt_table]]
side_table = Table(
[[norm_title, Spacer(6,1), mgmt_title],
[norm_table, Spacer(6,1), mgmt_table]],
colWidths=[half, 6, half]
)
side_table.setStyle(TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("LEFTPADDING", (0,0), (-1,-1), 0),
("RIGHTPADDING", (0,0), (-1,-1), 0),
("TOPPADDING", (0,0), (-1,-1), 0),
("BOTTOMPADDING",(0,0), (-1,-1), 0),
]))
story.append(side_table)
story.append(Spacer(1, 8))
# ══════════════════════════════════════════════════════════════════════════════
# INVESTIGATION ALGORITHM BOX
# ══════════════════════════════════════════════════════════════════════════════
inv_title = Table([[Paragraph("Step-wise Investigation Algorithm", style("IT",
fontSize=9.5, textColor=WHITE, fontName="Helvetica-Bold",
alignment=TA_CENTER, leading=12))]],
colWidths=[COL])
inv_title.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), colors.HexColor("#b7600c")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("ROUNDEDCORNERS",(0,0), (-1,-1), [4,4,0,0]),
]))
story.append(inv_title)
steps = [
["1", "Beta-hCG", "Exclude pregnancy — always the FIRST step"],
["2", "CBC + Platelets", "Assess anaemia; detect thrombocytopenia"],
["3", "TSH", "Thyroid dysfunction → anovulation"],
["4", "Prolactin", "Hyperprolactinemia → anovulation"],
["5", "Coagulation (PT, aPTT, vWF)", "Exclude coagulopathy (esp. adolescents)"],
["6", "FSH, LH, Testosterone", "Evaluate HPO axis; hyperandrogenism (PCOS)"],
["7", "TVUS / SIS", "Structural causes — polyps, fibroids, endometrial thickness"],
["8", "Endometrial biopsy", "Women >35 y, prolonged anovulation, risk factors for Ca"],
["9", "Hysteroscopy", "Gold standard for intracavitary pathology; directed biopsy"],
]
step_rows = [[Paragraph("<b>#</b>", CELL_HDR), Paragraph("<b>Test</b>", CELL_HDR), Paragraph("<b>Purpose</b>", CELL_HDR)]]
for s in steps:
step_rows.append([
Paragraph(f"<b>{s[0]}</b>", style("SN", fontSize=11, textColor=colors.HexColor("#b7600c"),
fontName="Helvetica-Bold", alignment=TA_CENTER, leading=14)),
Paragraph(s[1], CELL_KEY),
Paragraph(s[2], CELL_TXT),
])
step_table = Table(step_rows, colWidths=[10*mm, 55*mm, COL - 65*mm])
step_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#7c3a05")),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
*[("BACKGROUND", (0,i), (-1,i), GREY_BG if i%2==1 else WHITE) for i in range(1, 10)],
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#e0c9b0")),
("BOX", (0,0), (-1,-1), 0.8, colors.HexColor("#b7600c")),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("ALIGN", (0,0), (0,-1), "CENTER"),
("ROUNDEDCORNERS",(0,0), (-1,-1), [0,0,4,4]),
]))
story.append(step_table)
story.append(Spacer(1, 6))
# ── Footer ─────────────────────────────────────────────────────────────────
HRFlowable(width=COL, thickness=0.5, color=MID_GREY)
story.append(HRFlowable(width=COL, thickness=0.5, color=MID_GREY))
story.append(Spacer(1, 3))
story.append(Paragraph(
"FIGO 2011 Classification • Sources: Goldman-Cecil Medicine · Berek & Novak's Gynecology · Rosen's Emergency Medicine • For educational use only",
FOOT_S))
# ══════════════════════════════════════════════════════════════════════════════
# BUILD
# ══════════════════════════════════════════════════════════════════════════════
doc.build(story)
print(f"PDF saved: {OUTPUT}")
Running Command
cd /home/daytona/workspace/palm-coein && python3 generate_pdf.py 2>&1
Running Command
ls -lh /home/daytona/workspace/palm-coein/PALM_COEIN_Quick_Reference.pdf
Your PALM-COEIN Quick Reference PDF is ready:
PALM COEIN Quick Reference
PDF Document · PDF
What's inside (single A4 page):
| Section | Contents |
|---|---|
| Header | Title + AUB definition box |
| PALM (red) | P-A-L-M table with pathology, clinical features, investigations |
| COEIN (green) | C-O-E-I-N table with mechanism, features, key tests |
| Side-by-side | Normal menstrual parameters + Management overview |
| Algorithm | 9-step investigation sequence |
| Footer | FIGO 2011 source credit |
This is a shared conversation. Sign in to Orris to start your own chat.