Differential diagnosis for skin eruption with itching
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I have comprehensive material from Fitzpatrick's Dermatology and Harrison's Principles. Now I can compose a thorough, well-organized differential diagnosis.
Differential Diagnosis: Skin Eruption with Itching (Pruritic Rash)
A pruritic skin eruption has a broad differential that is best organized by morphology, distribution, and associated features. Below is a systematic framework drawn from Fitzpatrick's Dermatology and Harrison's Principles of Internal Medicine.
1. Eczematous / Dermatitic Disorders
These are the most common causes and characteristically present with pruritus as the dominant symptom.
| Condition | Key Features |
|---|---|
| Atopic Dermatitis (AD) | Flexural distribution (antecubital, popliteal fossae); personal/family history of asthma/allergic rhinitis; starts in infancy; lichenification from chronic scratching; elevated IgE; Dennie-Morgan folds |
| Allergic Contact Dermatitis (ACD) | Antigen-specific (Type IV hypersensitivity); well-demarcated; localized to site of contact (e.g., nickel, poison ivy, rubber); diagnosed by patch testing |
| Irritant Contact Dermatitis (ICD) | Non-immunologic; caused by inherent properties of the offending agent (acids, bases, detergents); well-demarcated; typically occupational |
| Lichen Simplex Chronicus | End stage of chronic itch-scratch cycle; circumscribed lichenified plaque; posterior neck, dorsum of feet, ankles |
| Seborrheic Dermatitis | Yellowish, greasy scale; scalp, nasolabial folds, eyebrows, retroauricular; associated with Malassezia overgrowth |
| Nummular Dermatitis | Coin-shaped, oozing, crusted plaques; extremities; common in dry skin states |
- Fitzpatrick's Dermatology, block4; Harrison's, p. 426-428
2. Urticarial Eruptions
These present as transient, blanching wheals with intense itch, lasting <24 hours per lesion.
- Urticaria (acute/chronic) - IgE-mediated or non-immunologic; mast cell degranulation; wheals with surrounding flare
- Neutrophilic urticaria - Urticarial plaques with neutrophilic infiltrate on biopsy
- Papular urticaria - Insect bite hypersensitivity; children; grouped papulovesicles
- Urticarial vasculitis - Urticarial plaques lasting >24 hours; burning > itching; may show purpura; requires biopsy
- Dermal hypersensitivity reaction
- Polymorphous eruption of pregnancy (PEP/PUPPP) - Third trimester; urticarial papules in striae
- Urticarial bullous pemphigoid - Urticarial prodrome before blistering in elderly patients
- Acute hemorrhagic edema of childhood
- Fitzpatrick's Dermatology, block1 (Urticaria/Urticaria differential)
3. Maculopapular / Exanthematous Eruptions
- Drug eruptions (morbilliform) - Most common drug reaction; symmetric blanching macules/papules; trunk-first; starts 7-14 days after drug initiation
- Viral exanthems - Measles, rubella, roseola, EBV, parvovirus B19 (slapped cheek); diffuse, symmetric
- Pityriasis rosea - Herald patch followed by "Christmas tree" distribution; collarette scale; mild itch
- Secondary syphilis - Involves palms and soles; painless; maculopapular to papulosquamous
4. Papulosquamous Disorders
| Condition | Distinguishing Features |
|---|---|
| Psoriasis | Well-demarcated erythematous plaques with silvery scale; extensor surfaces, scalp, nails; Auspitz sign; can be pruritic |
| Lichen Planus | Purple, polygonal, pruritic, flat-topped papules (the "4 Ps"); Wickham striae; flexor wrists, ankles, oral mucosa |
| Dermatophytosis (Tinea) | Annular, scaly, advancing border; KOH positive; tinea corporis, cruris, pedis |
| Pityriasis versicolor | Hypo- or hyperpigmented scaly macules; trunk; Malassezia furfur; mild itch |
5. Vesiculobullous Disorders (Pruritic)
- Scabies - Intense nocturnal itch; burrows in web spaces, wrists, genitalia; mites; household contacts affected
- Chickenpox (Varicella) - Intensely pruritic; "dewdrop on a rose petal" vesicles; successive crops; fever
- Bullous pemphigoid - Elderly; tense bullae on urticarial base; subepidermal; IgG anti-hemidesmosome (BP180/BP230)
- Dermatitis herpetiformis - Intensely pruritic; grouped vesicles on extensor surfaces; associated with celiac disease; IgA deposits at dermal papillae
- Dyshidrotic eczema (pompholyx) - Deep-seated vesicles on palms and soles; episodic; associated with stress and atopy
6. Infestations & Infections
- Scabies - Classic nocturnal itch, burrows, household clustering
- Pediculosis (lice) - Head, body, pubic; pruritus from bites
- Insect bites/papular urticaria - Grouped; excoriated; seasonal
- Tinea infections - Fungal; annular; KOH preparation diagnostic
7. Systemic Causes of Pruritus with or without Rash
Systemic conditions can produce pruritus, sometimes with secondary excoriation lesions but without a primary eruption:
| Systemic Cause | Clue |
|---|---|
| Cholestasis (primary biliary cholangitis, obstruction) | Elevated ALP/GGT; jaundice; bile acid deposition |
| Chronic kidney disease | Uremia; "half-and-half" nails; elevated creatinine |
| Hematologic malignancy (lymphoma, polycythemia vera) | B symptoms; aquagenic pruritus in PCV; lymphadenopathy |
| Thyroid disorders | Hypothyroidism (dry skin, myxedema) or hyperthyroidism (warm, moist skin) |
| Iron deficiency anemia | Pruritus without primary lesion; pallor |
| HIV/AIDS | Pruritic papular eruption; eosinophilic folliculitis |
| Diabetes mellitus | Generalized or localized (candidiasis, intertrigo) |
| Pregnancy | PEP, cholestasis of pregnancy, prurigo of pregnancy |
8. Targetoid / Immunobullous (Erythema Multiforme Spectrum)
- Erythema multiforme - Target lesions; at least 2 zones; triggered by HSV or mycoplasma; acral
- Fixed drug eruption - Recurrent at same site; post-drug exposure; leaves post-inflammatory hyperpigmentation
- Stevens-Johnson Syndrome / TEN - Mucosal involvement; epidermal detachment; drug-induced emergency
Clinical Approach to Narrow the Differential
- Morphology - Macule, papule, vesicle, wheal, plaque, scale, lichenification, burrow
- Distribution - Flexural (AD), extensor (psoriasis), acral (EM, scabies), dermatomal (zoster), universal
- Duration & course - Acute (<6 weeks) vs. chronic; episodic vs. persistent
- Associated symptoms - Fever (infection), joint pain (psoriatic arthritis), mucosal involvement (LP, SJS)
- History - New medications, contacts, travel, atopic history, occupational exposures
- Investigations - KOH prep, skin biopsy with DIF, patch testing, IgE levels, CBC, LFTs, renal function
- Fitzpatrick's Dermatology (toolbox): "History, distribution, examine mucous membranes, biopsy for routine histology and DIF, viral studies, other lab workup depending on morphology."
Ige
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Excellent - a clear diagram. Now I have everything needed for a comprehensive answer on IgE.
Immunoglobulin E (IgE)
Structure & Basic Properties
IgE is the least abundant immunoglobulin isotype in human serum, with a normal concentration of approximately 100-400 ng/mL. The vast majority of IgE is tissue-bound (attached to mast cells and basophils), with a serum half-life of only ~2 days. It is a monomer with an extra constant domain (CH4) compared to IgG, which contributes to its high-affinity receptor binding.
- Scott-Brown's Otorhinolaryngology, block2
Production - Isotype Switching
IgE is not produced directly; it arises from isotype class switching of IgM-secreting B cells:
- An antigen (allergen) is presented via MHC II to a Th0 cell
- In the presence of IL-4, Th0 differentiates into a Th2 cell
- Th2 cells secrete IL-4 and IL-13, which drive B cells to switch from IgM to IgE production
- Plasma cells secrete IgE, which binds to FcεRI on mast cells (MC)
This process occurs mainly in the bone marrow and draining regional lymph nodes, though local IgE production at mucosal sites has also been reported (e.g., in local allergic rhinitis).
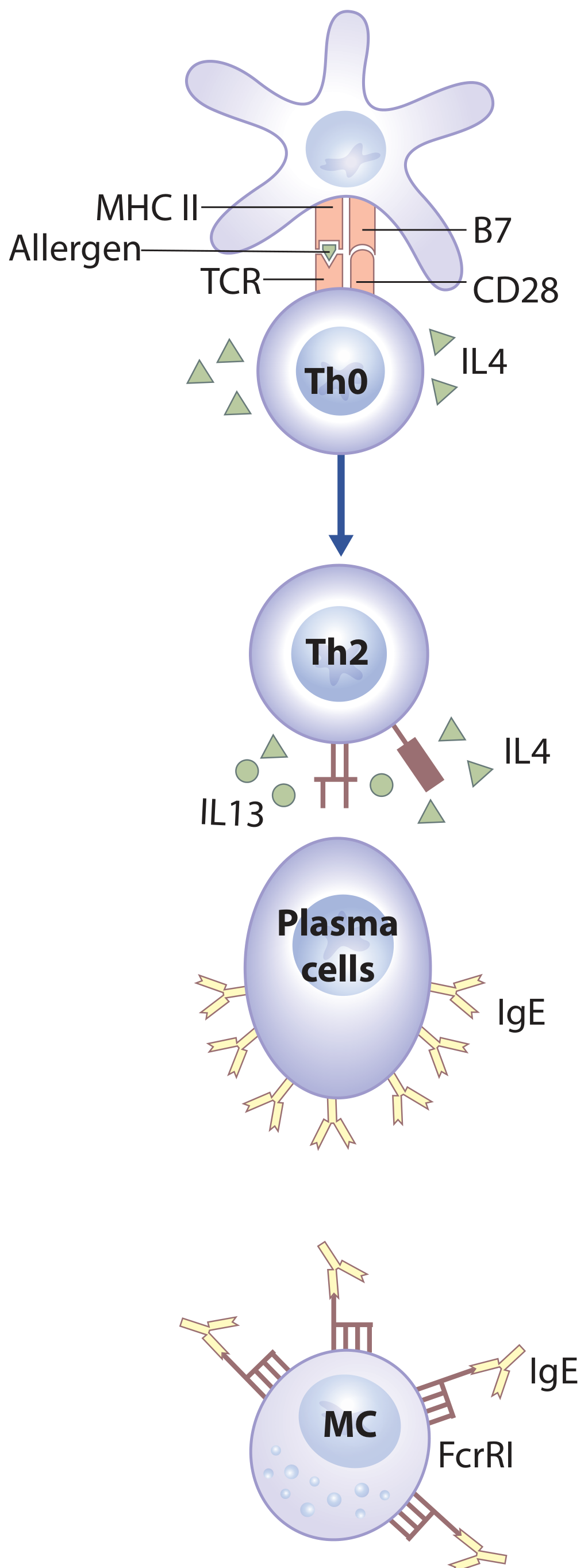
Figure: Th2 development and IgE production. Allergen presented via MHC II drives Th0→Th2 differentiation (IL-4 required). Th2 cells produce IL-4/IL-13, driving plasma cells to secrete IgE, which loads onto mast cells (MC) via FcεRI. - Scott-Brown's Otorhinolaryngology
Receptors
| Receptor | Affinity | Cells Expressing It | Role |
|---|---|---|---|
| FcεRI (high affinity) | Very high (Kd ~10⁻¹⁰ M) | Mast cells, basophils, eosinophils | Mediates Type I hypersensitivity; binds IgE Fc region; cross-linking triggers degranulation |
| FcεRII / CD23 (low affinity) | Lower | B cells, monocytes, macrophages | Regulates IgE synthesis; antigen presentation |
Low-level FcεRI expression is also detected on dendritic cells and macrophages, though their significance is less certain.
- Scott-Brown's Otorhinolaryngology, block2
Mechanism of Type I (Immediate) Hypersensitivity
IgE is the central antibody of Type I (immediate) hypersensitivity, which follows two phases:
Sensitization phase:
- First antigen exposure → IgE produced → IgE binds via Fc to FcεRI on mast cells/basophils (no symptoms yet)
Effector phase:
- Second antigen exposure → antigen cross-links two adjacent IgE molecules on mast cells → signal transduction → degranulation
Mediators released:
| Mediator | Type | Effects |
|---|---|---|
| Histamine | Preformed (primary) | Vasodilation, increased vascular permeability, bronchospasm, pruritus |
| Tryptase | Preformed | Marker of mast cell activation; elevated in anaphylaxis |
| Prostaglandins | Newly formed (secondary) | Edema, bronchoconstriction |
| Leukotrienes C4/D4 | Newly formed | Vasodilation, vascular permeability (slow-reacting substances) |
| Leukotriene B4 | Newly formed | Chemoattractant; recruits leukocytes |
| PAF | Newly formed | Platelet aggregation, bronchoconstriction |
| Cytokines (TNF-α, IL-4) | Secondary | Sustain and amplify inflammation |
- Jawetz Medical Microbiology, block2; Cellular and Molecular Immunology, block4
Note: In anaphylaxis, histamine and PAF are elevated in ~70-100% of cases, while tryptase is elevated in only ~60%.
Clinical Conditions Associated with Elevated IgE
Atopic / Allergic diseases:
- Atopic dermatitis (eczema) - often markedly elevated
- Allergic asthma
- Allergic rhinitis (hay fever)
- Urticaria
Infectious:
- Parasitic infections (helminths - very high IgE, e.g., ascariasis, toxocariasis)
- Allergic bronchopulmonary aspergillosis (ABPA) - a normal IgE level excludes this diagnosis
Immunodeficiency syndromes:
- Hyper-IgE syndrome (Job syndrome) - IgE often >2000 IU/mL; eczema + recurrent staphylococcal abscesses + skeletal abnormalities; STAT3 mutation
- Wiskott-Aldrich syndrome - elevated IgE with thrombocytopenia and immunodeficiency
- Netherton syndrome, Omenn syndrome
Neoplastic:
- IgE myeloma (rare monoclonal IgE)
- Tietz Textbook of Laboratory Medicine, block42; Dermatology 2-Vol Set, block13
Measurement of IgE
| Test | What It Measures | Clinical Use |
|---|---|---|
| Total serum IgE | Sum of all IgE regardless of specificity | Screening for atopic state; diagnosis of ABPA, Hyper-IgE syndrome; parasite screening |
| Specific IgE (sIgE) | IgE against a particular allergen | Identifies the causative allergen (e.g., ImmunoCAP) |
| Skin prick test | In vivo mast cell degranulation | Rapid, sensitive allergen identification |
Important caveats:
- Large overlap exists between IgE levels in allergic and non-allergic individuals
- Total IgE alone has limited diagnostic utility for common allergic diseases
- A normal IgE does not exclude allergic disease
- IgE levels may wane with age in Hyper-IgE syndrome
Methods used: ELISA, fluorescence enzyme immunoassay (FEIA/ImmunoCAP), chemiluminescence immunoassay (CIA), near-infrared particle immunoassay (NIPIA).
- Tietz Textbook of Laboratory Medicine, block42
IgE-Targeted Therapy
Omalizumab is a humanized monoclonal anti-IgE antibody (anti-IgE therapy). It blocks IgE from binding to FcεRI on mast cells and basophils, preventing degranulation. Approved uses include:
- Severe allergic asthma
- Chronic spontaneous urticaria
- Nasal polyps with comorbid asthma
- Allergic bronchopulmonary aspergillosis (ABPA)
- Scott-Brown's Otorhinolaryngology, block10; Katzung's Pharmacology, block11
Summary Table
| Property | Detail |
|---|---|
| Serum concentration | ~100-400 ng/mL (lowest of all Ig isotypes) |
| Half-life (serum) | ~2 days |
| Half-life (tissue-bound) | Weeks |
| Heavy chain | ε (epsilon) |
| Produced by | Plasma cells (after Th2-driven isotype switching) |
| Key cytokines driving production | IL-4, IL-13 (from Th2 cells) |
| High-affinity receptor | FcεRI (mast cells, basophils, eosinophils) |
| Low-affinity receptor | FcεRII / CD23 (B cells, monocytes) |
| Primary role | Type I hypersensitivity; anti-parasite immunity |
| Anti-IgE drug | Omalizumab |
This is a shared conversation. Sign in to Orris to start your own chat.