Dystomelia
Reading File
Finding Sources
Searching the Web
dystomelia medical definition limb malformation
Finding Sources
Searching the Web
dystomelia congenital limb defect definition classification
Searching PubMed
dystomelia limb malformation congenital
Finding Sources
Reading Web Page
dysmelia definition classification types causes treatment
Searching the Web
dysmelia definition phocomelia amelia thalidomide limb deficiency types
Reading File
Reading File
Reading File
Diaestmatomyleia
Reading File
Finding Sources
Finding Sources
Searching PubMed
diastematomyelia spinal cord split
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook content and MRI images. Here is the full clinical summary:
Diastematomyelia
(Your spelling "Diaestmatomyleia" = diastematomyelia — also called split cord malformation)
Definition
Diastematomyelia is a congenital malformation in which the spinal cord is longitudinally split into two hemicords, each containing one anterior and one posterior grey matter horn. It belongs to the group of split notochord syndromes — disorders of notochord midline integration — and is classified under occult spinal dysraphism. The alternative term is split cord malformation (SCM).
- Localization in Clinical Neurology, 8e — listed explicitly as the "spinal notochord syndrome"
- Grainger & Allison's Diagnostic Radiology
Classification (Pang's Types)
| Type I | Type II | |
|---|---|---|
| Dural sacs | Two separate dural sacs | Single dural sac |
| Septum | Rigid osteocartilaginous (bony) spur | Fibrous band between hemicords |
| Plain X-ray | May show scoliosis, hemivertebrae, bifid/fused vertebrae at spur level | Usually normal |
| Tethering | Hemicords fuse tightly just below the spur | Less tethering |
There is a craniocaudal gradient of division: partial clefting cranially → two complete dural sacs separated by a bony spur inferiorly in Type I.
"In type I diastematomyelia, there are two complete dural sacs. There is a craniocaudal gradient of division, ranging from partial clefting cranially to two complete dural sacs separated by an osteocartilaginous spur inferiorly." — Grainger & Allison's Diagnostic Radiology
Pathogenesis
Aberrant neuro-endodermal adhesions during early embryogenesis are the most accepted mechanism. A persistent adhesion between ectoderm and endoderm splits the notochord/neural plate, leading to formation of two hemicords with interposing mesenchymal tissue that ossifies into a bony spur (Type I) or remains fibrous (Type II).
Associated Anomalies
- Tethered spinal cord — most important association; progressive cord dysfunction occurs from repeated flexion/extension stretching the tethered cord
- Hydromyelia — dilation of the central canal, may affect either or both hemicords
- Low conus medullaris / thick/fatty filum terminale
- Scoliosis
- Spina bifida / lipomyelomeningodysplasia
- Dermal sinus
- Intramedullary lipoma
- Klippel-Feil syndrome
Clinical Features
Presentation varies by age and whether cord dysfunction is progressive:
| Age group | Features |
|---|---|
| Infants | Decreased spontaneous leg movements; skin stigmata (midline hair tuft, dimple, lipoma, dermal sinus) |
| Children | Delayed walking, abnormal gait, poor bladder control |
| Adolescents/Adults | Back and leg pain, sensory loss, difficulty walking, urinary incontinence, sexual dysfunction |
Cutaneous markers overlying the spine (hair tuft, lipoma, dimple, hyperpigmented patch) are important clinical flags prompting imaging.
Associated orthopedic findings: scoliosis, leg length discrepancy.
Associated urologic findings: poor bladder control, recurrent UTIs, loss of previously attained continence.
"Common associated spinal anomalies include diastematomyelia (split cord), spinal lipomas, dermal sinuses, and fibrolipomas of the filum terminale. Progressive cord dysfunction can occur when repeated flexion and extension of the spine results in stretching of the tethered cord." — Goldman-Cecil Medicine
Imaging
MRI is the investigation of choice.
MRI Findings:
- Sagittal T1: may show severe scoliosis; division of spinal cord into right and left hemicords
- Axial T1/T2: two separate hemicords visible side-by-side within the spinal canal
- Type I: bony spur with marrow signal on MRI, completely extradural, usually midline
- Type II: fibrous band of T2 hypointensity passing intradurally between hemicords; may be subtle
Plain radiograph: scoliosis, hemivertebrae, bifid or fused vertebrae at spur level (Type I).
MRI of diastematomyelia (Bradley & Daroff's Neurology in Clinical Practice):
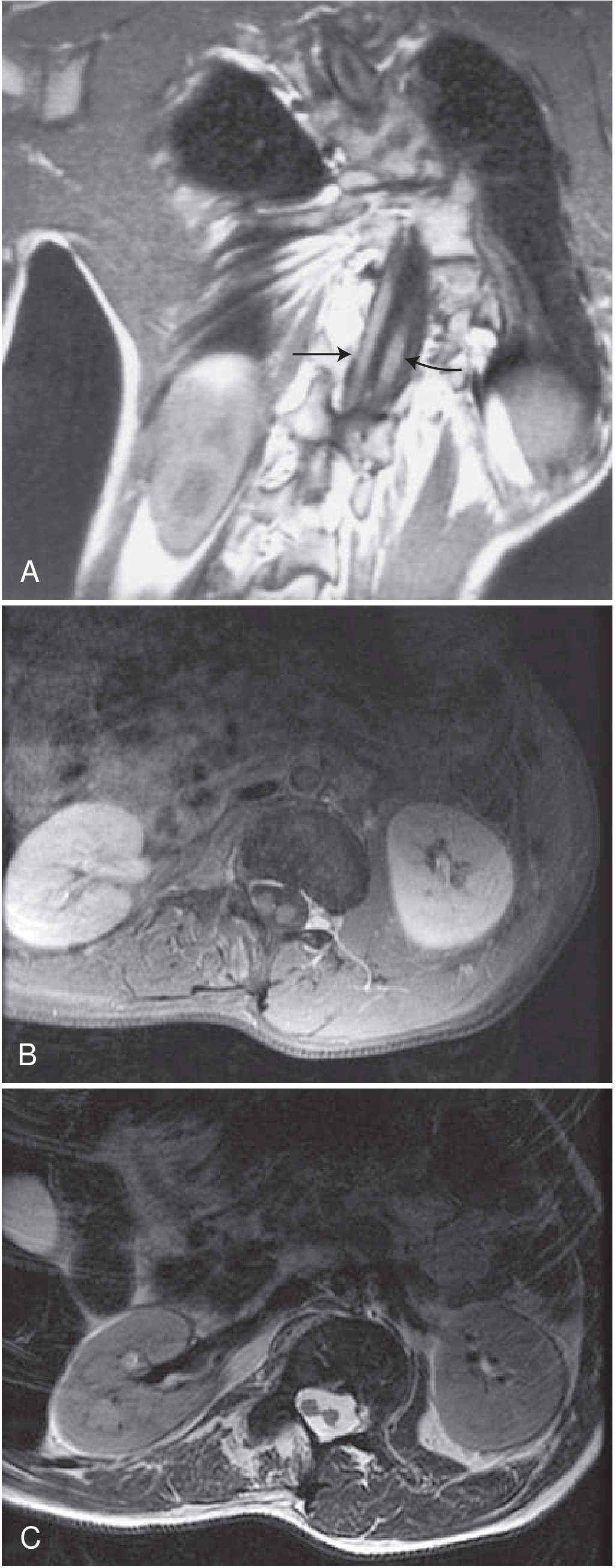
A. Sagittal T1 — severe scoliosis with spinal cord dividing into right (arrow) and left (curved arrow) hemicords.
B & C. Axial T1 and T2 — two distinct separate hemicords in cross-section.
Type II diastematomyelia — cervical cord with associated craniocervical meningocele (Grainger & Allison):
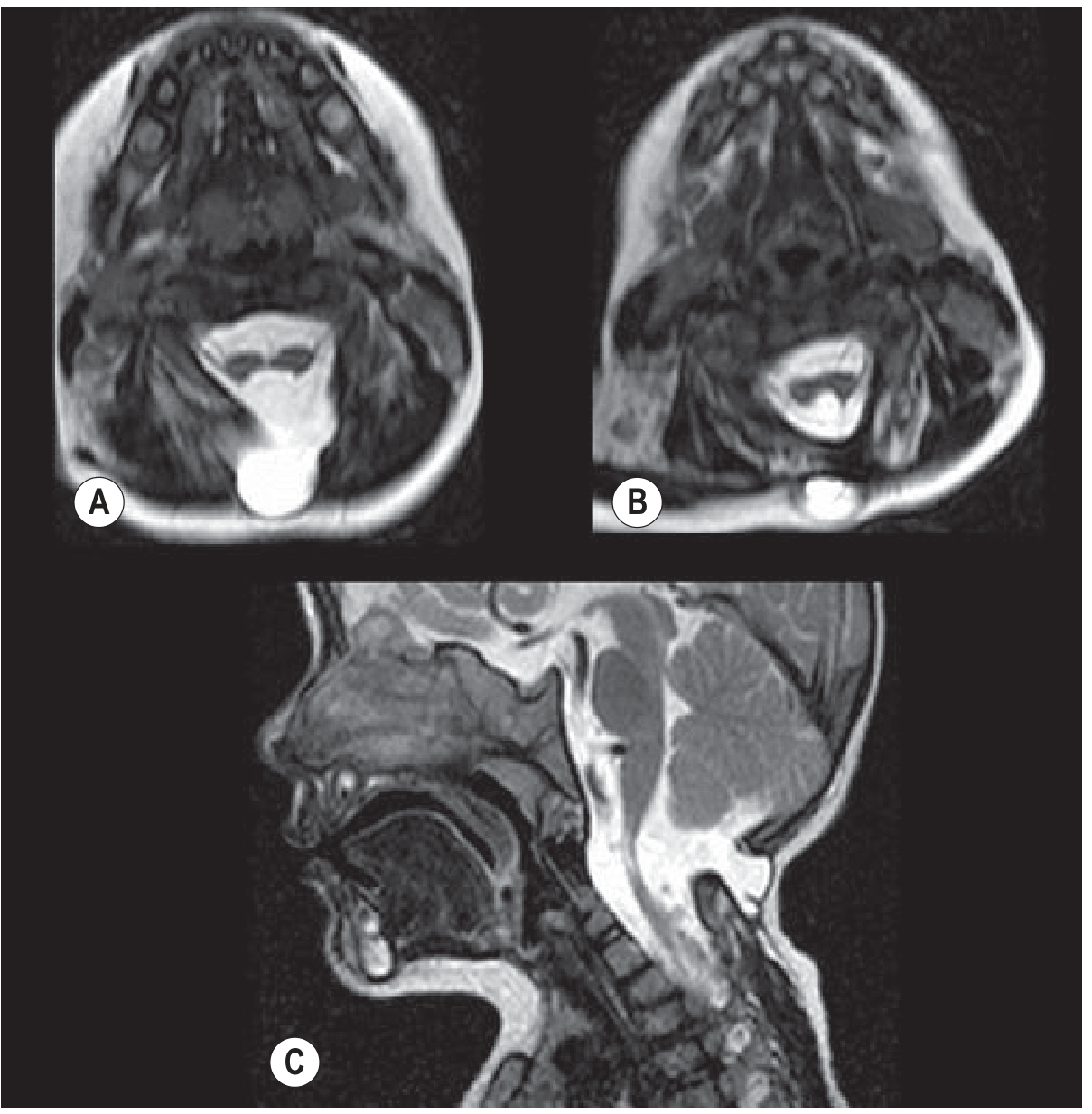
A & B. Axial T2 — cord splits into two hemicords; normal CSF between them creates the apparent "signal abnormality". C. Sagittal — apparent cord thinning is the clue; hemicords reunite inferiorly.
Management
Treatment is surgical in symptomatic patients:
- Surgical untethering — release of the tethered cord; excision of the bony or fibrous septum
- Indications: progressive neurological deficit, significant tethered cord syndrome, symptomatic cases
- Asymptomatic individuals: surgical value is uncertain (cord often retethers post-operatively)
- Bladder dysfunction: managed with intermittent catheterization, UTI treatment, genitourinary reflux surveillance
Prenatal management (when detected antenatally):
- Detailed anatomic fetal survey + fetal echocardiogram
- Genetic counselling; karyotype ± microarray
- MRI to identify associated anomalies
- Serial ultrasound for head growth monitoring
- Goldman-Cecil Medicine; Creasy & Resnik's Maternal-Fetal Medicine
Recent Literature
A 2023 prenatal diagnosis case review (PMID 37491555) confirmed diastematomyelia can be reliably diagnosed by prenatal ultrasound and MRI, with the axial plane being most informative for demonstrating the split cord. A 2021 pediatric spinal cord disease review (PMID 34470868) emphasizes early surgical intervention to prevent irreversible neurological decline.
This is a shared conversation. Sign in to Orris to start your own chat.