Skin disorders in emergency room and its management Elaborate major skin Emergencies
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Excellent - I now have rich content from multiple authoritative textbooks. Let me compile the comprehensive response.
Major Skin Emergencies in the Emergency Room
Skin emergencies are conditions where dermatological pathology is immediately life-threatening or organ-threatening. The clinician must recognize these rapidly and act decisively - delay worsens mortality in most of them.
Overview: Classification of Skin Emergencies
| Category | Condition | Key Threat |
|---|---|---|
| Severe drug reactions | SJS / TEN / DRESS | Sepsis, multi-organ failure |
| Necrotizing infections | Necrotizing fasciitis | Septic death, limb loss |
| Septicemia with skin signs | Meningococcemia / Purpura fulminans | DIC, shock, death |
| Autoimmune blistering | Pemphigus vulgaris / Bullous pemphigoid | Fluid/protein loss, sepsis |
| Anaphylaxis/urticaria | Anaphylaxis with angioedema | Airway compromise |
| Erythroderma | Exfoliative dermatitis | Thermoregulation failure |
| Staphylococcal toxin | SSSS (Staphylococcal scalded skin syndrome) | Sepsis, fluid loss (esp. children) |
1. Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN)
What They Are
SJS and TEN exist on a continuum of severity - both are severe cutaneous adverse reactions (SCARs) and potentially fatal blistering drug eruptions. They are distinct from erythema multiforme (EM), which is largely HSV-associated.
- SJS: <10% body surface area (BSA) epidermal detachment
- SJS/TEN overlap: 10-30% BSA detachment
- TEN (Lyell syndrome): >30% BSA detachment
Incidence: 0.4-1.2 per million person-years for TEN; 1.2-6.0 per million for SJS.
Causative Drugs
"More than 100 medications have been reported to cause SJS and TEN."
- TMP-SMX (1-3 per 100,000)
- Nevirapine
- Lamotrigine (1:1,000 adults; 3:1,000 children)
- Carbamazepine (14:100,000) - especially in HLA-B*1502-positive Asians
- Allopurinol (most common cause in Europe currently)
- NSAIDs, other anticonvulsants, antibiotics (sulfonamides, penicillins)
Genetic warning: HLA-B*1502 (Han Chinese, SE Asian populations) dramatically increases SJS/TEN risk with carbamazepine. HLA typing before starting carbamazepine is recommended in all Asian patients.
Clinical Presentation
- Prodrome: fever, influenza-like symptoms 1-4 days before rash
- Skin: deep red/dusky macules on face and trunk, spreading rapidly; "2-zone" or atypical targetoid lesions; central desquamation; bullae formation, then sloughing
- Two or more mucosal surfaces are almost always involved in SJS: oral (hemorrhagic crusting), conjunctival, urethral, vaginal, anal
- Symptoms: photophobia, dysphagia, dysuria, cough (tracheobronchial involvement)
- "Pure TEN": dusky macular erythema with rapid full-thickness epidermal separation (no targetoid lesions)

Mortality Risk: SCORTEN
Score 1 point each for:
- Age >40
- Malignancy present
- BSA involved >10%
- Tachycardia (HR >120)
- BUN >28 mg/dL
- Serum bicarbonate <20 mEq/L
- Blood glucose >14 mmol/L
| SCORTEN | Mortality |
|---|---|
| 0-1 | 3.2% |
| 2 | 12.1% |
| 3 | 35.3% |
| 4 | 58.3% |
| ≥5 | >90% |
Respiratory tract involvement (bronchial TEN + ARDS) carries ~70% mortality.
Management
- Immediate cessation of causative drug - single most important intervention
- ICU or burn unit admission; multidisciplinary team
- Fluid resuscitation: approximately 2/3 of the Parkland formula (less than burn victims)
- Nutritional support and monitoring for sepsis
- Wound care: leave involved epidermis in place as biological dressing; nonstick dressings; silver-impregnated dressings; minimize tape-to-skin; IV lines at uninvolved sites
- Mucosal care: nonstick dressings to separate eroded mucosal surfaces; ophthalmology consult (risk of symblepharon/blindness); gynecology and urology consults as needed; amniotic membrane application for eyes
- Systemic immunosuppression (controversial, no consensus):
- European practice: Cyclosporine 3-6 mg/kg/day (divided)
- US practice: IVIG 1 g/kg/day for 4 days ± corticosteroids
- Etanercept: shown beneficial in moderate RCT (Asia)
- Early short-course high-dose steroids may help in some cases
Source: Andrews' Diseases of the Skin, Clinical Dermatology
2. Necrotizing Fasciitis
Definition
A rapidly progressive, life- and limb-threatening infection of the skin, subcutaneous tissue, and deep fascia characterized by widespread fascial necrosis with relative sparing of overlying skin initially.
Risk Factors
Diabetes mellitus, tobacco use, postoperative/peripartum state, IV drug use, obesity, immunosuppression.
Clinical Recognition - "Hard to Diagnose Early"
Early signs are subtle and may mimic simple cellulitis:
- Erythema, warmth, swelling, pain "out of proportion to appearance"
- Skin becomes brawny, violaceous, then dusky/gray
- Late: skin necrosis, bullae, frank gangrene, crepitus (gas-forming organisms)
- Systemic: fever, tachycardia, hypotension, altered mental status
- Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC score): CRP, WBC, Hgb, Na, creatinine, glucose
Pathogenic Types
- Type I (polymicrobial): streptococci, staphylococci, gram-negatives, anaerobes (most common)
- Type II (monomicrobial): Group A Streptococcus (flesh-eating disease) or Staphylococcus aureus
- Type III: Clostridial (gas gangrene - myonecrosis)
- Type IV: Fungal (Candida, Mucor) - immunocompromised hosts
Management - Surgical Emergency
"Rapid surgical intervention remains the mainstay of therapy...Surgical intervention less than 24 hours following onset is associated with improved clinical outcomes." - Fitzpatrick's Dermatology
- Immediate surgical consult - do not delay for further imaging if clinical diagnosis is clear
- Radical debridement of all necrotic tissue; staged daily re-debridements until clean
- Wound closure: vacuum-assisted closure (VAC) devices + skin grafting after source control
- Amputation may be required for severe limb disease (especially in diabetics)
- Broad-spectrum antibiotics (IDSA 2014 guidelines): vancomycin OR linezolid OR daptomycin PLUS one of: piperacillin-tazobactam / carbapenem / ceftriaxone + metronidazole / fluoroquinolone + metronidazole - narrow based on tissue culture
- Fluid resuscitation + electrolyte monitoring (significant wound drainage)
- IVIG: limited evidence; may consider in Group A Strep NF (neutralizes exotoxins)
- Hyperbaric oxygen: insufficient data; ongoing research
3. Meningococcemia and Purpura Fulminans
Meningococcemia - A Classic Emergency
Caused by Neisseria meningitidis. The rash is the critical clinical clue.
Cutaneous findings (from Fitzpatrick's Dermatology, Vol. 1):
- Initial: small, irregular petechiae with a "smudged" appearance
- Distribution: extremities most common; also palms, soles, mucous membranes, conjunctiva
- Petechiae in 60% of patients on presentation; higher in children 1-18 years (74%)
- Critical sign: rapid increase in number and size of petechiae correlates with fulminant disease
Purpura Fulminans
Occurs when meningococcemia progresses to severe DIC:
- Retiform purpura (branching, stellate necrosis)
- Skin necrosis extending to subcutaneous tissue, muscle, and bone
- Low protein C levels
- Gangrene of digits and distal extremities

Management
- Immediate IV benzylpenicillin (or ceftriaxone 2g IV if penicillin allergy) - do not delay for LP if patient is unstable
- Blood cultures before antibiotics if possible - but do not delay treatment
- ICU admission, sepsis resuscitation (fluids, vasopressors, oxygen)
- DIC management: FFP, cryoprecipitate, platelets as guided by coagulation profile
- Protein C concentrate may be considered in purpura fulminans
- Surgical care for gangrenous tissue (may require amputation)
- Close contacts: chemoprophylaxis (rifampicin, ciprofloxacin, or ceftriaxone)
4. DRESS Syndrome (Drug Reaction with Eosinophilia and Systemic Symptoms)
Also known as Drug-Induced Hypersensitivity Syndrome (DiHS).
Features
- Onset: 2-8 weeks after starting offending drug (longer latency than SJS)
- Rash: morbilliform eruption (face, upper trunk, extremities), often with facial edema
- Systemic involvement: fever, lymphadenopathy, hepatitis (most common), nephritis, pneumonitis, myocarditis, thyroiditis
- Hematologic: eosinophilia (hallmark), atypical lymphocytes
- Viral reactivation: HHV-6, EHV-7, CMV, EBV commonly reactivate and may drive severity
Common culprit drugs: allopurinol, carbamazepine, lamotrigine, phenytoin, dapsone, vancomycin, minocycline, sulfonamides
Management
- Stop the offending drug immediately
- Systemic corticosteroids: prednisone 1-2 mg/kg/day (mainstay; taper slowly over weeks to months to prevent relapse)
- Monitor liver function, renal function, CBC regularly
- Monitor for HHV-6 reactivation; antivirals (valganciclovir) if severe or HHV-6-driven
- Avoid re-exposure to causative drug; cross-reactivity within anticonvulsant class
5. Staphylococcal Scalded Skin Syndrome (SSSS)
Features
- Primarily affects neonates and children <5 years (adults if immunocompromised/renal failure)
- Caused by exfoliative toxins A and B from Staphylococcus aureus (usually phage type 71)
- Toxins cleave desmoglein-1 in the superficial epidermis
- Prodrome: fever, irritability, skin tenderness
- Rash: starts perioral/periorbital, then generalized erythema, then flaccid bullae and desquamation
- Nikolsky sign positive (lateral pressure on erythematous skin causes epidermal slipping)
- No mucosal involvement (distinguishes from SJS/TEN - mucosae contain desmoglein-3 which is not affected by the toxin)
Management
- Hospitalization; neonates to NICU
- Anti-staphylococcal antibiotics: IV nafcillin or oxacillin; clindamycin (inhibits toxin production); vancomycin if MRSA suspected
- Fluid and electrolyte replacement
- Wound care: gentle handling; nonstick dressings; emollients
- Prognosis: excellent in children with treatment (mortality <5%); worse in adults (~60%)
6. Anaphylaxis with Urticaria/Angioedema
Skin Signs
- Urticaria: pruritic, raised, evanescent wheals; can be anywhere on body
- Angioedema: deeper, non-pitting swelling; face, lips, tongue, throat (life-threatening when laryngeal)
- Together with systemic features (bronchospasm, hypotension, tachycardia) = anaphylaxis
Management (ABC-first approach)
- Epinephrine 0.3-0.5 mg IM (anterolateral thigh) - first-line, do not delay
- Airway: supplemental O2; early intubation or surgical airway if laryngeal edema
- IV fluids: 1-2 L normal saline for hypotension
- Antihistamines: diphenhydramine (H1) + ranitidine/famotidine (H2) - adjuncts only, NOT first-line
- Systemic corticosteroids: methylprednisolone IV - reduces biphasic reactions
- Observe for minimum 4-6 hours (24 hours if severe); prescribe epinephrine auto-injector on discharge
- Allergist referral for identification and avoidance of trigger
7. Erythroderma (Exfoliative Dermatitis)
Definition
Generalized redness and scaling involving >90% of body surface area.
Causes ("5 Ps + D")
- Psoriasis (most common underlying disease)
- Pityriasis rubra pilaris
- Primary dermatoses (atopic dermatitis, contact dermatitis, seborrheic)
- Drugs (sulfonamides, gold, isoniazid, captopril, many others)
- Paraneoplastic (Sézary syndrome - cutaneous T-cell lymphoma)
- De novo / idiopathic (in ~30%)
Systemic Complications
- Hypothermia or hyperthermia (disrupted thermoregulation)
- High-output cardiac failure (massive cutaneous vasodilation - up to 30% increase in skin blood flow)
- Protein/fluid loss through skin
- Hypoalbuminemia, edema
- Secondary bacterial infection/sepsis
- Renal failure
Management
- Hospitalize - often ICU
- Treat precipitating cause (stop drug, treat underlying psoriasis/dermatitis)
- Temperature control: warm room, blankets (patients cannot thermoregulate)
- Fluid and electrolyte replacement
- Nutritional support (high caloric needs from hypermetabolic state)
- Emollients and wet compresses for skin comfort
- Skin biopsy for diagnosis (especially to exclude Sézary syndrome)
- Treat secondary infections with appropriate antibiotics
- Disease-specific systemic therapy once diagnosis is confirmed
Quick ER Reference Summary
| Emergency | Key Clue | Immediate Action |
|---|---|---|
| SJS/TEN | Mucosal erosions + skin sloughing after drug | Stop drug; burn unit; IVIG or cyclosporine |
| Necrotizing Fasciitis | Pain out of proportion; skin necrosis; crepitus | Surgical debridement + broad-spectrum ABx |
| Meningococcemia | Non-blanching petechiae/purpura + fever | IV ceftriaxone STAT; ICU |
| Purpura Fulminans | Retiform purpura + DIC | Sepsis management; FFP; protein C |
| DRESS | Morbilliform rash + eosinophilia + organ dysfunction | Stop drug; systemic steroids |
| SSSS | Children with skin tenderness + positive Nikolsky; no mucosal involvement | IV anti-staphylococcal ABx |
| Anaphylaxis | Urticaria + angioedema + systemic features | IM epinephrine FIRST |
| Erythroderma | >90% BSA erythema + scaling + systemic compromise | Hospitalize; thermoregulation; treat cause |
Sources consulted:
- Andrews' Diseases of the Skin, Clinical Dermatology - SJS/TEN (pp. 139-142)
- Fitzpatrick's Dermatology, 2-Volume Set - Necrotizing fasciitis management; meningococcemia and purpura fulminans (pp. 2812-2813)
- Goldman-Cecil Medicine - Urticaria, angioedema, anaphylaxis
- Sabiston Textbook of Surgery - Necrotizing fasciitis surgical management
- IDSA 2014 Guidelines (cited within Fitzpatrick's) - antimicrobial therapy for necrotizing infections
Emergency room skin disorders based on tintinalli and rosens
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from both Tintinalli's and Rosen's. Let me compile the full response.
Emergency Room Skin Disorders
Based on Tintinalli's Emergency Medicine & Rosen's Emergency Medicine
Approach to the Dermatologic Patient in the ED
Both Tintinalli and Rosen emphasize a structured approach: identify whether the presentation is life-threatening first, then characterize the morphology, distribution, and associated systemic findings. The most dangerous skin disorders in the ED fall into three groups:
- Severe generalized drug/immune reactions (SJS, TEN, DRESS, pemphigus)
- Infectious emergencies with skin signs (meningococcemia, necrotizing fasciitis, cellulitis)
- Vascular/purpuric disorders (purpura fulminans)
PART 1 - SEVERE GENERALIZED SKIN DISORDERS
(Tintinalli Chapter 249; Rosen's Chapter 118/23)
1. Erythema Multiforme (EM)
Tintinalli's perspective:
"Until the early 1990s, erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrolysis were classified as a continuum of a spectrum of disease; it is now appreciated that erythema multiforme is distinct from the more serious or even life-threatening Stevens-Johnson syndrome and toxic epidermal necrolysis."
Causes:
- Adults: drugs (barbiturates, penicillins, sulfonamides, NSAIDs, phenothiazines)
- Children: predominantly infections - HSV-1/HSV-2 account for 70-90% of all EM cases; Mycoplasma pneumoniae also common
Clinical Features:
- Abrupt onset rash, sometimes preceded by burning; pruritus usually absent
- Classic "target" (iris) lesion: 2-3 zones - dark center, lighter surrounding zone, red outer ring
- Symmetric distribution on hands, feet, extensor surfaces
- EM minor: limited distribution
- EM major: oral mucosal involvement; ophthalmologic lesions in ~70% of cases

Management (Tintinalli TABLE 249-2):
| Severity | Treatment | Disposition |
|---|---|---|
| EM Minor | Prednisone 60-80 mg/day PO x 3-5 days; oral antihistamine; acyclovir if HSV-related | Outpatient; PCP/derm follow-up |
| EM Major (SJS) | Remove trigger; resuscitate; fluid/electrolytes; methylprednisolone 125 mg IV q6h or equivalent; diphenhydramine + viscous lidocaine rinses for oral lesions; Burow's solution (5% aluminum acetate) with cool compresses for blisters; ophthalmology consult; antibiotics only if established infection | Admit - acute care/burn unit; intensivist + dermatologist consults |
2. Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN)
Classification (Tintinalli):
"Some authorities include Stevens-Johnson syndrome as a severe form of erythema multiforme major, whereas others consider it a less severe form of toxic epidermal necrolysis. Perhaps the most appropriate classification approach for the emergency physician is to recognize that the severity and extent of epidermal detachment reflects the spectrum of disease."
- SJS: <10% BSA epidermal detachment
- SJS/TEN overlap: 10-30% BSA
- TEN: >30% BSA detachment
Precipitating drugs: Sulfonamides (TMP-SMX most common), anticonvulsants (phenytoin, carbamazepine, lamotrigine), allopurinol, antibiotics, NSAIDs, nevirapine.
ED Clinical Presentation:
- Flu-like prodrome (fever, malaise, myalgias) 1-4 days before skin lesions
- Maculopapular rash progressing rapidly to confluent erythema, bullae, and skin sloughing
- Mucous membranes: painful erosions of oral, ocular, urogenital mucosae in virtually all SJS cases
- Positive Nikolsky sign (lateral pressure causes epidermal separation)
- May have ARDS, hepatitis, renal failure
Tintinalli TABLE 249-2 - Management of TEN:
| Step | Action |
|---|---|
| Remove trigger | Stop all suspected causative drugs immediately |
| Resuscitation | Airway (respiratory involvement possible), circulatory support |
| Fluids | Fluid + electrolyte management (~2/3 of burn Parkland formula) |
| Wound care | Burow's solution compresses; nonstick dressings; leave sloughed epidermis in place as biologic dressing |
| Infection | Antibiotics only for confirmed infection - NOT prophylactic |
| Specialist care | Ophthalmology, gynecology, urology as indicated; dermatologist mandatory |
| Disposition | ICU or burn unit; intensivist + dermatologist consults |
Prognostic score - SCORTEN (1 point each for: age >40, HR >120, BSA involved >10%, BUN >28 mg/dL, serum glucose >14 mmol/L, bicarbonate <20 mEq/L, malignancy): mortality 3.2% at 0-1 points, >90% at ≥5 points.
3. Pemphigus Vulgaris
Autoimmune blistering disorder producing flaccid bullae that rupture easily, causing extensive skin and mucosal erosions. Risk of superinfection and sepsis.
Tintinalli TABLE 249-2 - Management:
| Action |
|---|
| Remove any drug trigger |
| Resuscitate (respiratory +/- circulatory) |
| Fluid and electrolyte management |
| Antibiotics only for confirmed infection (not prophylactic) |
| Immunosuppressive therapy |
| Plasmapheresis |
| Immunoglobulin therapy (IVIG) |
| Disposition: Admit - acute care/burn unit; intensivist + dermatologist |
4. Exfoliative Dermatitis (Erythroderma)
Generalized erythema and scaling covering >90% BSA. Causes: psoriasis, atopic dermatitis, drug reaction, Sézary syndrome (T-cell lymphoma), idiopathic.
Tintinalli TABLE 249-2:
| Severity | Treatment | Disposition |
|---|---|---|
| Minor | Remove trigger; symptomatic care (oral pain agents, antihistamines PRN) | Outpatient; PCP/derm follow-up |
| Major | Resuscitate; fluid/electrolytes; warm environment (thermoregulation impaired); emollients; treat infection; systemic therapy per dermatologist | Admit; correct hypothermia/hypovolemia; dermatology consult before systemic corticosteroids |
5. DRESS Syndrome (Drug Rash with Eosinophilia and Systemic Symptoms)
(Tintinalli Chapter 249)
"DRESS syndrome is a severe adverse drug reaction that usually develops within 8 weeks of initiation of drug therapy. Aromatic anticonvulsants (such as phenytoin and phenobarbital), allopurinol, and sulfa medications are the most common culprits."
Clinical features:
- Onset 2-8 weeks after drug initiation
- Fever + rash + internal organ involvement (liver, kidneys, hematologic most common)
- Rash polymorphic: can mimic exfoliative dermatitis or SJS
- Eosinophilia in ~30%; hepatic and renal dysfunction
- Genetic predisposition present; must warn family members

Management (Tintinalli):
- Immediate cessation of suspected culprit drug
- Systemic steroids in severe cases (hepatitis, pneumonitis, or extensive exfoliative dermatitis)
- Supportive care: antipyretics, antipruritic medications
- Hospital admission; monitor LFTs, renal function, CBC
PART 2 - PURPURIC / VASCULAR EMERGENCIES
(Tintinalli Chapter 249; Rosen's Chapter 118)
6. Meningococcemia
(Rosen's: Chapter 118 - "Bacterial Meningitis and Meningococcemia")
(Tintinalli: Chapter 249 - "Purpuric Disorders")
"A rash is frequently noted on presentation and is an invaluable clue to the correct diagnosis early in the disease course." - Tintinalli
Pathogen: Neisseria meningitidis (gram-negative diplococcus)
Population: <20 years; highest risk in children/infants <5 years; military recruits, college dorms
Clinical spectrum (Rosen's):
| Form | Features |
|---|---|
| Bacteremia | Febrile illness ± rash; no meningeal signs |
| Meningococcal meningitis | Fever, headache, neck stiffness; rash in >50%; seizures in 20% |
| Meningococcal septicemia | Lethargy, poor perfusion, cyanosis; hemorrhagic skin lesions in 28-77% |
| Fever + non-blanching rash | Up to 30% - can progress to fulminant disease if untreated |
| Purpura fulminans | Rapidly spreading ecchymoses + gangrene; most advanced form |
Skin findings (Tintinalli):
- Petechiae, urticaria, hemorrhagic vesicles, macules, maculopapules
- Classic: petechiae on extremities and trunk, palms, soles, head, mucous membranes
- Petechiae evolve into palpable purpura with gray necrotic centers - pathognomonic
- Mechanism: organism invades and destroys endothelium causing infectious vasculitis

Investigations (Rosen's):
- Blood cultures (positive in 50-80%); obtain before antibiotics if no delay
- Lumbar puncture in stable patients without DIC
- Gram stain of petechial scrapings: gram-negative diplococci in up to 2/3 of cases
- PCR of buffy coat/CSF - most sensitive and specific; unaffected by prior antibiotics
- CBC (bandemia typical), coagulation profile, metabolic panel, CXR, lactate, echo if myocarditis suspected
Treatment (Rosen's):
| Situation | Antibiotic |
|---|---|
| Standard proven meningococcemia | Penicillin G 4 million units IV q4h (adults); 250,000-300,000 units/kg/day IV q4h (children) |
| First-line empirical (ID uncertain) | Ceftriaxone or cefotaxime IV |
| Penicillin-allergic | Chloramphenicol |
- Dexamethasone 0.4-0.6 mg/kg/day q6h x 4 days for bacterial meningitis - give before first antibiotic dose if possible
- Corticosteroids in meningococcemia without meningitis: controversial; consider only if persistent shock despite fluids + vasopressors (possible adrenal insufficiency)
- Fulminant meningococcemia: airway management + IV fluid resuscitation + vasopressors; FFP for DIC bleeding; hemodialysis if anuric; correct electrolyte/acid-base abnormalities
- Plasmapheresis, blood exchange, ECMO: described but limited data
Chemoprophylaxis for close contacts (Rosen's):
- Rifampin 10 mg/kg (max 600 mg) PO q12h x 4 doses (neonates: 5 mg/kg; warn about urine/secretion discoloration)
- Alternative: Ceftriaxone IM 125 mg (children <15 years) or 250 mg (>12 years) - preferred in pregnancy
- Alternative: Ciprofloxacin 500 mg PO single dose (adults)
7. Purpura Fulminans
(Tintinalli Chapter 249)
"Purpura fulminans is a rare vascular disorder characterized by fever, shock, multiorgan failure, and the rapid development of hemorrhagic skin necrosis."
Causes: Hereditary or acquired Protein C/S deficiency; activated protein C resistance; any cause of DIC (including meningococcemia)
Dermatologic triad (Tintinalli):
- Widespread ecchymoses
- Hemorrhagic bullae
- Epidermal necrosis
Also: cyanosis with necrosis of nose, ears, genitalia; distal extremity gangrene
Management:
- Treat underlying sepsis aggressively
- DIC management: FFP, cryoprecipitate, platelets
- Protein C concentrate where available
- ICU; surgical care for gangrenous tissue
PART 3 - INFECTIOUS SKIN EMERGENCIES
(Tintinalli Chapters 192-194)
8. Cellulitis and Erysipelas
Tintinalli Disposition and Follow-up:
- Admit if: systemic toxicity, diabetes mellitus, alcoholism, immunosuppression
- Discharge if: healthy, no systemic toxicity - outpatient with 2-3 day follow-up; mark the perimeter of infection with indelible marker to monitor progression
Tintinalli TABLE 192-4 - Empiric Antibiotic Treatment:
| Severity | Antibiotic |
|---|---|
| Mild (no systemic infection, drainable abscess, immunocompetent) | No antibiotics required after complete drainage |
| Moderate (purulent cellulitis, no systemic infection) | TMP-SMX DS 1-2 tabs PO BID x 7-10 days OR Doxycycline 100 mg PO BID x 7-10 days OR Clindamycin 300-450 mg PO QID x 7-10 days |
| Severe (systemic infection/sepsis, immunocompromised) - IV antibiotics | For MRSA: Vancomycin 15 mg/kg IV q12h OR Linezolid 600 mg IV q12h OR Daptomycin 4 mg/kg IV q24h OR Telavancin 10 mg/kg IV q24h |
For non-purulent cellulitis and erysipelas (primarily streptococcal): beta-lactams are appropriate (cefazolin IV, or oral cephalexin/dicloxacillin for mild-moderate).
9. Necrotizing Fasciitis
(Tintinalli Chapter 149 / Chapter 7 in postoperative complications section)
"Hallmark of fasciitis are the presence of marked systemic toxicity and pain out of proportion to local findings." - Tintinalli
Risk factors: Diabetes mellitus, hypertension, obesity, alcoholism, immunosuppression, peripheral vascular disease - but also occurs in young, healthy individuals.
Early differentiation from cellulitis is difficult - Tintinalli notes CT findings that help:
- Asymmetric fascial thickening
- Gas tracking along fascial planes (pathognomonic)
- Focal fluid collections
- MRI: sensitive but not entirely specific
Late signs: Deep pain with surface hypesthesia; crepitation; bullae; rapidly progressing skin necrosis
Management (Tintinalli):
- Antibiotics - Triple therapy: Penicillin or cephalosporin + aminoglycoside + clindamycin (clindamycin inhibits toxin production)
- Immediate surgical debridement - do not delay
- ICU admission; fluid resuscitation; monitor electrolytes
PART 4 - URTICARIA, ANGIOEDEMA, AND ANAPHYLAXIS
(Tintinalli Chapter 14)
10. Urticaria
"Urticaria, or hives, is a cutaneous reaction marked by acute onset of pruritic, erythematic wheals of varying size that generally are described as 'fleeting.'" - Tintinalli
ED Management (Tintinalli):
- Identify and remove offending agent
- H1 antihistamines ± corticosteroids (note: adding corticosteroids to non-sedating antihistamines may not improve relapse or itch reduction)
- Epinephrine for severe or refractory cases
- H2 antihistamine (ranitidine/famotidine) in severe/chronic/unresponsive cases
- Cold compresses for symptomatic relief
- Refer to allergist for severe, recurrent, or refractory cases
11. Angioedema
(Tintinalli Chapter 14 - TABLE 14-6)
"Angioedema of the tongue, lips, and face has the potential for airway obstruction." - Tintinalli
ACE inhibitor-induced angioedema occurs in 0.1-0.7% of patients on ACE inhibitors. Mechanism involves bradykinin and substance P - does NOT respond well to antihistamines/steroids/epinephrine.
Tintinalli TABLE 14-6 - Pharmacologic Treatment of Angioedema:
| Agent | Dose | Notes |
|---|---|---|
| C1 esterase inhibitor [human] (Berinert) | 20 U/kg IV (HAE); 1000 U IV (ACE-inhibitor angioedema) | Effective in HAE and ACE-I angioedema; adverse: headache, GI symptoms |
| C1 esterase inhibitor [recombinant] (Ruconest) | 50 U/kg IV (max 4200 U) | Effective in HAE; no data for ACE-I angioedema |
| Icatibant (Firazyr) | 30 mg SC | Bradykinin B2 receptor antagonist; effective in HAE + ACE-I angioedema; single dose highly effective; 90% local reactions |
| Epinephrine | 0.3-0.5 mg IM | For life-threatening laryngeal/allergic angioedema |
| H1 antihistamines | Standard doses | Adjunct - limited benefit in bradykinin-mediated angioedema |
| Corticosteroids | Methylprednisolone IV | Adjunct |
Priority: Secure the airway early. Angioedema can progress rapidly and unpredictably.
PART 5 - PEDIATRIC INFECTIOUS SKIN EMERGENCIES
12. Kawasaki Disease
(Tintinalli Chapter 142 - Rashes in Infants and Children)
"Kawasaki's disease is the leading cause of acquired heart disease in children."
Diagnostic criteria (Classic disease): Fever ≥5 days PLUS 4 of:
- Bilateral non-exudative conjunctivitis
- Cervical lymphadenopathy
- Erythema of lips and oral mucosa (strawberry tongue)
- Skin changes of extremities (erythema, edema, desquamation)
- Rash (variable morphology; vesicles not described; perineal predilection)
- Peak age: 18-24 months; <6 months or >9 years have poorer outcomes
- Mortality <0.5% - mainly from coronary artery aneurysm rupture
- Most devastating complication: sudden cardiac death from coronary aneurysms
Quick Reference: Disposition Summary
| Condition | Disposition | Key First Steps in ED |
|---|---|---|
| EM Minor | Outpatient | Steroids, antihistamines, acyclovir if HSV |
| SJS (EM Major) | Admit - ICU/Burn Unit | Stop drug; resuscitate; fluids; ophthalmology |
| TEN | Admit - ICU/Burn Unit | Stop drug; resuscitate; burn care principles |
| Pemphigus | Admit - ICU/Burn Unit | Fluids; IVIG; immunosuppression |
| DRESS | Admit | Stop drug; systemic steroids if severe |
| Erythroderma Major | Admit | Warm environment; fluids; dermatology before steroids |
| Meningococcemia | Admit - ICU | Ceftriaxone IV STAT; blood cultures; LP if stable |
| Purpura Fulminans | Admit - ICU | Antibiotics; FFP; vasopressors; DIC management |
| Necrotizing Fasciitis | Admit - OR | Surgical debridement + triple antibiotics |
| Cellulitis (severe) | Admit | IV vancomycin ± beta-lactam; mark borders |
| Angioedema (laryngeal) | Admit - ICU | Airway FIRST; C1 inhibitor/icatibant; epinephrine |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Chapters 14, 142, 192-194, 249-250
- Rosen's Emergency Medicine: Concepts and Clinical Practice - Chapter 118 (Meningococcemia), Chapter 42 (Soft Tissue)
Emergency room skin disorders management
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Emergency Room Skin Disorders - Management
Based on Tintinalli's Emergency Medicine & Rosen's Emergency Medicine
ED APPROACH TO SKIN DISORDERS
Tintinalli's advises a structured approach: determine whether the presentation is a dermatologic emergency first, then systematically characterize lesion morphology, distribution, mucosal involvement, and systemic features.
Key history points (Tintinalli Ch. 248):
- Duration, rate of progression, % BSA involved
- Medication history (especially drugs started within 2-8 weeks) - EM, SJS, TEN, DRESS are drug-induced
- Exposures: chemicals, foods, animals, insects, plants, travel, occupational, ill contacts
- Sexual history where relevant
- Painful rash = red flag; rarely self-limiting
Examination principle:
"Use the burn rule of nines to estimate the degree of skin involvement in disorders with widespread distribution."
A painful rash is always a red flag. Mucosal involvement in a blistering eruption demands immediate hospitalization.
PART 1 - LIFE-THREATENING SKIN EMERGENCIES
1. Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN)
Classification:
- SJS: <10% BSA epidermal detachment
- SJS/TEN overlap: 10-30%
- TEN: >30% BSA - mortality up to 90% with SCORTEN ≥5
Causative agents: TMP-SMX, carbamazepine, phenytoin, lamotrigine, allopurinol, NSAIDs, penicillins, nevirapine
ED Management (Tintinalli TABLE 249-2):
| Action | Detail |
|---|---|
| Stop causative drug | Single most important step |
| Resuscitate | Airway (bronchial involvement possible), circulatory support |
| Fluid management | ~2/3 Parkland formula (less than burns); fluid + electrolytes |
| Wound care | Burow's solution (5% aluminum acetate) + cool compresses for blisters; nonstick dressings; leave epidermis in situ as biologic dressing |
| Mucosal care | Diphenhydramine + viscous lidocaine rinses for oral lesions; ophthalmology for ocular involvement |
| Antibiotics | Only for confirmed/suspected infection - NOT prophylactic |
| Systemic Rx | Methylprednisolone 125 mg IV q6h (or equivalent); IVIG or cyclosporine per specialist |
| Disposition | ICU or burn unit; intensivist + dermatologist |
SCORTEN Mortality Predictor (1 point each):
| Parameter | Threshold |
|---|---|
| Age | >40 years |
| Heart rate | >120 bpm |
| BSA involved | >10% |
| BUN | >28 mg/dL |
| Blood glucose | >14 mmol/L |
| Bicarbonate | <20 mEq/L |
| Malignancy | Present |
Score 0-1 = 3.2% mortality; Score ≥5 = >90% mortality
2. Pemphigus Vulgaris
Autoimmune blistering with flaccid bullae, mucosal erosions; risk of fluid/protein loss and sepsis.
Management (Tintinalli TABLE 249-2):
- Remove any drug trigger
- Fluid and electrolyte resuscitation
- Immunosuppressive therapy (prednisone + rituximab or azathioprine)
- IVIG (immunoglobulin therapy)
- Plasmapheresis for severe cases
- Antibiotics only for confirmed infection
- Admit: ICU/burn unit; intensivist + dermatologist
3. Exfoliative Dermatitis (Erythroderma)
Generalized erythema and scaling >90% BSA. Causes: psoriasis, drug reaction, atopic dermatitis, Sézary syndrome.
Management (Tintinalli TABLE 249-2):
| Severity | Treatment | Disposition |
|---|---|---|
| Minor | Remove trigger; oral analgesics and antihistamines PRN | Outpatient; PCP/derm follow-up |
| Major | Resuscitate; fluid/electrolyte replacement; warm room (thermoregulation impaired); emollients; treat secondary infection | Admit; correct hypothermia/hypovolemia; obtain dermatology consult before systemic corticosteroids |
4. DRESS Syndrome
Onset 2-8 weeks after drug initiation. Fever + rash + organ involvement (liver > kidney > hematologic).
Tintinalli key points:
- Eosinophilia occurs in ~30% of cases
- Rash may resemble exfoliative dermatitis OR SJS
- Genetic predisposition is present - discuss risk with patient's family members
ED Management:
- Immediately stop the causative drug
- Systemic corticosteroids for severe cases with hepatitis, pneumonitis, or extensive dermatitis
- Antipyretics and antipruritic agents (supportive)
- Admit to hospital; monitor LFTs, renal function, CBC, eosinophil count
5. Purpura Fulminans
Tintinalli (Ch. 249):
"Purpura fulminans is a rare vascular disorder characterized by fever, shock, multiorgan failure, and the rapid development of hemorrhagic skin necrosis."
Clinical triad:
- Widespread ecchymoses
- Hemorrhagic bullae
- Epidermal necrosis (nose, ears, genitalia, distal extremities)
Management:
- Treat underlying sepsis (antibiotics + vasopressors)
- DIC management: FFP, cryoprecipitate, platelets
- Protein C concentrate
- ICU; surgical care for gangrenous areas
PART 2 - INFECTIOUS SKIN EMERGENCIES
6. Necrotizing Fasciitis
Tintinalli (Ch. 152):
"Hallmark of fasciitis are the presence of marked systemic toxicity and pain out of proportion to local findings."

LRINEC Score - Laboratory Risk Indicator for Necrotizing Fasciitis (Tintinalli TABLE 152-6):
| Lab | Threshold | Points |
|---|---|---|
| CRP | >150 mg/L | +4 |
| WBC | >15,000/mm³ (or >25,000) | +1 |
| Hemoglobin | <13.5 g/dL (or <11) | +1 |
| Sodium | <135 mmol/L | +2 |
| Creatinine | >1.6 mg/dL | +2 |
| Glucose | >180 mg/dL | +1 |
Note (Tintinalli): LRINEC ≥6 has been proven to miss many cases, especially Vibrio species and neck infections. Clinical judgment remains paramount.
Imaging: CT: asymmetric fascial thickening, gas tracking along fascial planes, focal fluid collections. MRI is sensitive but not fully specific.
Management:
- Immediate surgical consultation - do not wait for imaging if clinical diagnosis clear
- IV antibiotics: triple therapy - penicillin/cephalosporin + aminoglycoside + clindamycin
- Surgical debridement within <24 hours - staged daily re-debridements
- Fluid resuscitation + electrolyte monitoring
- ICU admission
7. Cellulitis and Erysipelas
Tintinalli Disposition rule:
"Mark the patient's skin with an indelible marker along the perimeter of infection so healing can be determined at follow-up."
Admit if: Systemic toxicity, diabetes mellitus, alcoholism, or immunosuppression present.
Tintinalli TABLE 192-4 - Empiric Antibiotic Treatment:
| Severity | Indication | Treatment |
|---|---|---|
| Mild - No antibiotics | Healthy patient, complete abscess drainage, no systemic infection | None required |
| Moderate - Oral | Purulent cellulitis without systemic infection; drainable abscess + mild systemic signs | TMP-SMX DS 1-2 tabs PO BID × 7-10 days OR Doxycycline 100 mg PO BID × 7-10 days OR Clindamycin 300-450 mg PO QID × 7-10 days |
| Severe - IV (MRSA coverage) | Purulent cellulitis + systemic infection/sepsis; immunocompromised | Vancomycin 15 mg/kg IV q12h OR Linezolid 600 mg IV q12h OR Daptomycin 4 mg/kg IV q24h OR Telavancin 10 mg/kg IV q24h OR Clindamycin 600 mg IV q8h |
| Sepsis/unclear etiology | Add broad coverage | + Piperacillin-tazobactam 4.5 g IV q6h OR Meropenem 500-1000 mg IV q8h OR Imipenem-cilastatin 500 mg IV q6h |
| Water exposure | Fresh water (Aeromonas) or salt water (Vibrio) | + Doxycycline 100 mg IV q12h + Ceftriaxone 1 g IV q24h |
8. Skin Abscesses, Furuncles, and Carbuncles
(Tintinalli Ch. 152)
Management:
- Small furuncles: warm compresses to promote drainage; reassess in 2-3 days
- Sitz baths for buttock/perineal furuncles
- Large furuncles, carbuncles, abscesses: incision and drainage (I&D) required
- Simple needle aspiration inadequate for MRSA abscesses
- Use No. 11 or 15 scalpel blade over area of greatest fluctuation
- Use US to guide incision length and depth
- Break up loculations with a hemostat
- Pack the cavity with gauze; reassess at 48 hours
Incision and Drainage Technique (Tintinalli):
- Obtain consent; universal precautions including face shield
- Position for access; prep with povidone-iodine; drape
- Infiltrate from the side over the abscess; distend cavity with lidocaine
- Incise over area of greatest fluctuation
- Express contents; break loculations
- Pack with gauze wick; arrange 48-hour follow-up
Antibiotic indication after I&D: Only if moderate-severe systemic signs (see cellulitis table above)
PART 3 - VIRAL SKIN CONDITIONS IN THE ED
9. Herpes Zoster (Shingles)
(Tintinalli TABLE 250-2)
Clinical features: Vesicles and pustules on erythematous base in unilateral dermatomal distribution; associated pain, pruritus, dysesthesias. A unilateral band-like arrangement on the thorax is diagnostic.
Ramsay Hunt Syndrome: External auditory canal involvement + facial nerve paralysis + vestibulocochlear dysfunction.
| Condition | Drug | Dose | Duration |
|---|---|---|---|
| Herpes zoster | Acyclovir | 800 mg PO 5 times/day | 7 days |
| Herpes zoster | Valacyclovir | 1000 mg PO TID | 7 days |
- Initiate within first 72 hours of symptom onset for maximum benefit
- Reduces healing time, new lesion formation, risk of postherpetic neuralgia
- Immunocompromised patients with severe involvement: hospitalize for IV acyclovir
- Local care: aluminum acetate compresses TID + antibiotic ointment
- Treat pain aggressively (may be severe)
10. Herpes Simplex (HSV)
(Tintinalli TABLE 250-2)
Diagnosis: HSV type-specific NAATs are tests of choice (most sensitive/specific with active lesions). Viral culture is specific but less sensitive.
| Episode | Drug | Dose | Duration |
|---|---|---|---|
| Initial episode | Acyclovir | 400 mg PO TID or 200 mg PO 5x/day | 7-10 days |
| Initial episode | Valacyclovir | 1000 mg PO BID | 7-10 days |
| Recurrence | Acyclovir | 800 mg PO TID | 2 days |
| Recurrence | Valacyclovir | 500 mg PO BID | 3 days |
| Recurrence | Famciclovir | 1000 mg PO BID | 1 day |
| Suppressive therapy | Valacyclovir | 500-1000 mg PO daily | Long-term |
| Immunocompromised | Acyclovir | IV formulation | Inpatient |
PART 4 - PAPULOSQUAMOUS AND COMMON ED CONDITIONS
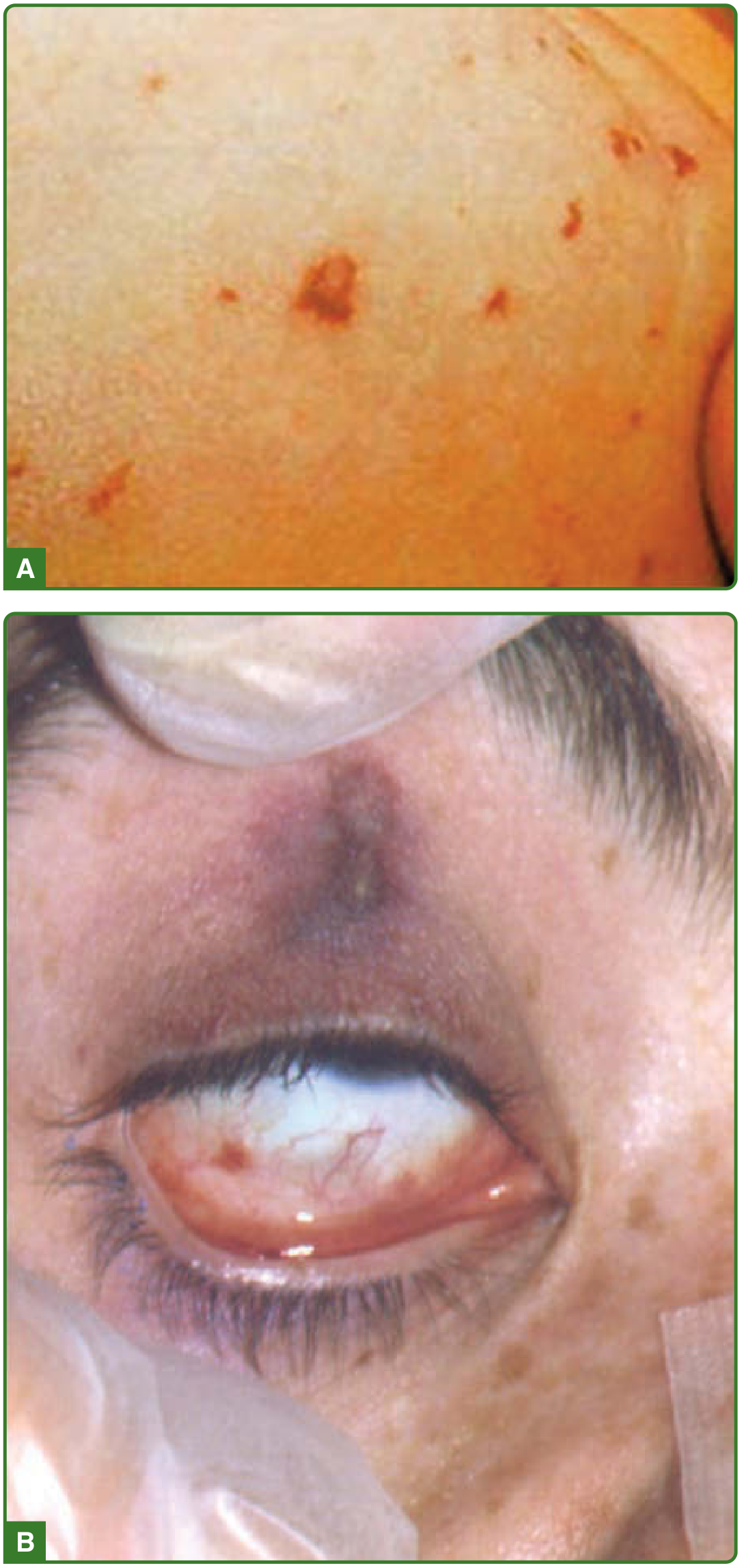
11. Scabies
(Rosen's Ch. 84; Tintinalli TABLE 35-2)
Cause: Sarcoptes scabiei mite. Transmission: direct contact, infested linens.
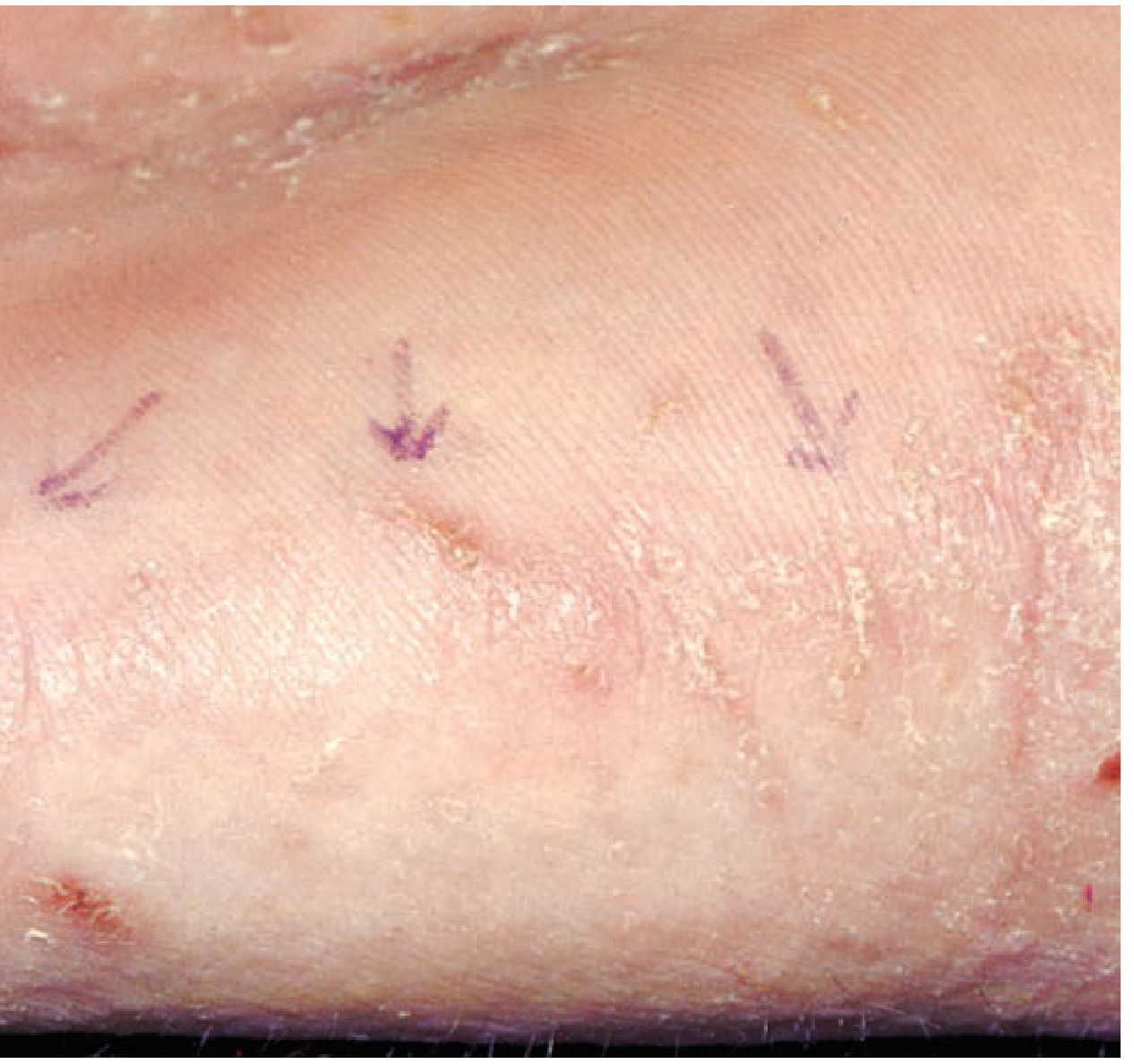
Features: Intense pruritus (hypersensitivity reaction); characteristic burrows; excoriations, papules, nodules on groin, genitalia, axilla, interdigital web spaces.
Diagnosis: Microscopic exam of scrapings - reveals mites.
| Agent | Dose/Application |
|---|---|
| Permethrin 5% cream (first-line) | One application at bedtime, entire body from neck down; wash off in 8-12 h; repeat in 7 days |
| Ivermectin (oral) | 200 mcg/kg PO once; repeat in 7 days |
| Topical ivermectin 1% | Alternative topical option |
Key instructions (both Tintinalli and Rosen's):
- Treat all household members and close contacts concurrently
- Wash linens and recently worn clothes in hot water; dry on high heat
12. Contact Dermatitis and Atopic Dermatitis
(Tintinalli TABLE 250-5, TABLE 35-2)
| Condition | Treatment |
|---|---|
| Poison ivy/oak (severe) | Oral antihistamines + clobetasol 0.05% or fluocinonide 0.05% topical; if severe: Prednisone 0.5 mg/kg/day × 2-3 weeks |
| Allergic contact dermatitis | Identify + avoid allergen; mid- to high-potency topical steroids (triamcinolone 0.1%, fluocinonide 0.05%); severe cases: oral prednisone 40-60 mg PO daily tapered over 3 weeks |
| Atopic dermatitis | High-potency: clobetasol 0.5%, halobetasol 0.5%; Mid-potency: triamcinolone 0.1%; Low-potency: hydrocortisone 2.5%; fexofenadine 180 mg morning + antihistamine at night |
| Photosensitivity | Photoprotection; identify and avoid photosensitizer |
13. Fungal Infections
(Tintinalli TABLE 250-3, TABLE 251-2, TABLE 35-2)

| Condition | Treatment | Notes |
|---|---|---|
| Tinea capitis | Griseofulvin microsize 20-25 mg/kg/day PO × 8 weeks OR Terbinafine 125-250 mg/day × 6 weeks | Add ketoconazole 2% or selenium sulfide 2.5% shampoo TID × 2 weeks; treat all close contacts simultaneously |
| Tinea corporis/cruris | Clotrimazole, miconazole topical; refractory: oral fluconazole or itraconazole | |
| Tinea barbae | Griseofulvin microsize 500 mg PO daily × 6 weeks OR Terbinafine 250 mg daily × 2-4 weeks | Avoid if hepatic disease; consider baseline LFTs |
| Pityriasis versicolor | Ketoconazole 2% shampoo as body wash daily × 7 days OR Ketoconazole/miconazole cream BID × 2-4 weeks | Discoloration may persist months after successful treatment |
14. Head/Scalp Conditions
(Tintinalli TABLE 250-3)
| Condition | Clinical Features | Treatment |
|---|---|---|
| Pediculosis capitis | Scalp pruritus (especially behind ears); lice + nits along hair shaft | Permethrin cream / pyrethrin lotion / ivermectin lotion / malathion cream; repeat in 7-10 days; machine wash linens |
| Dissecting cellulitis of scalp | Tender suppurative nodules; sinus tracts; scarring; alopecia | OTC antibacterial wash; doxycycline or minocycline 100 mg PO BID; I&D for fluctuant nodules; referral to dermatology |
| Seborrheic dermatitis | White-yellow scale on scalp, eyebrows, nasolabial folds, chest | OTC antidandruff shampoo; ketoconazole 2% shampoo/cream; desonide 0.05% or hydrocortisone 2.5% |
15. STI-Related Skin Conditions
(Rosen's Ch. 84)
| Condition | First-Line Treatment | Notes |
|---|---|---|
| Primary/Secondary syphilis | Benzathine penicillin G 2.4 million units IM single dose | Penicillin allergy: doxycycline or tetracycline × 2 weeks (except pregnancy/neurosyphilis) |
| Genital herpes (initial) | Acyclovir 400 mg PO TID × 7-10 days OR Valacyclovir 1000 mg BID × 7-10 days | Extend if not healed at 10 days |
| Chancroid | Azithromycin 1 g PO single dose OR Ceftriaxone 250 mg IM single dose | Incise and drain fluctuant buboes |
| Condyloma acuminata (HPV) | Provider-administered: cryotherapy, TCA/BCA, surgical excision; Patient-applied: imiquimod, podofilox, sinecatechins | ED may defer and refer; not a true emergency |
| Scabies (genital) | Permethrin 5% cream; treat all contacts | See scabies section above |
| Molluscum contagiosum | Refer for cryotherapy or curettage | Not emergent |
16. Urticaria and Angioedema
(Tintinalli Ch. 14)
Urticaria management:
- Identify and remove offending agent
- H1 antihistamines ± corticosteroids (note: adding steroids to non-sedating antihistamines alone may not reduce relapse risk)
- H2 antihistamine (ranitidine/famotidine) in severe/chronic/unresponsive cases
- Epinephrine 0.3-0.5 mg IM for severe or refractory cases
- Cold compresses for symptomatic relief
Angioedema - special considerations:
- ACE inhibitor angioedema occurs in 0.1-0.7% of ACE-I users
- Mechanism: bradykinin/substance P mediated - does NOT respond well to antihistamines/steroids/epinephrine
- Airway must be secured early - progression can be rapid and unpredictable
Tintinalli TABLE 14-6 - Specific Angioedema Agents:
| Agent | Dose | Indication |
|---|---|---|
| C1 esterase inhibitor [human] (Berinert) | 20 U/kg IV (HAE); 1000 U IV (ACE-I) | Hereditary angioedema (HAE) + ACE-I angioedema |
| C1 esterase inhibitor [recombinant] (Ruconest) | 50 U/kg IV (max 4200 U) | HAE |
| Icatibant (Firazyr) | 30 mg SC | HAE + ACE-I angioedema; bradykinin B2 receptor antagonist; ~10% need second dose |
PART 5 - TOPICAL THERAPY PRINCIPLES IN THE ED
(Tintinalli Ch. 248)
General topical rule:
"If it's dry, wet it; if it's wet, dry it."
Vehicle selection:
- Ointments (petroleum base, no preservatives): best for chronic dry conditions; winter months
- Creams (oil + water + preservative): most versatile; suitable for any body surface; may cause drying with chronic use
- Gels: useful for scalp, beard areas
- Patients allergic to cream preservatives: switch to ointment formulation
Corticosteroid Cream Dosing (Tintinalli TABLE 248-10):
| Body Area | Suggested Potency | Amount to Dispense |
|---|---|---|
| Face | Low | 45 g |
| Arm | Intermediate/Low | 90 g |
| Leg | Intermediate/Low | 180 g |
| Hand or foot | Intermediate/Low | 45 g |
| Forearm | Intermediate/Low | 45 g |
| Chest or back | Intermediate/Low | 180 g |
(Based on TID application × 10 days)
Non-steroidal topical agents:
- Emollients/moisturizers: reduce dryness, skin friction, and tightness; ointments best for chronic conditions
- Open wet dressings (tap water or saline): reduce discomfort; cleanse by painlessly loosening crusts
- Capsaicin 0.025% TID × 4 weeks: antipruritic via substance P depletion; not for age <10 years
- Pramoxine 1-2% or EMLA: topical anesthetics for pruritus; limited high-quality evidence
RAPID REFERENCE: Disposition by Condition
| Condition | Disposition | Priority |
|---|---|---|
| SJS/TEN | Admit - ICU/Burn Unit | CRITICAL |
| Pemphigus vulgaris | Admit - ICU/Burn Unit | CRITICAL |
| Necrotizing fasciitis | Admit - OR urgent | SURGICAL EMERGENCY |
| Meningococcemia | Admit - ICU | CRITICAL |
| Purpura fulminans | Admit - ICU | CRITICAL |
| DRESS syndrome | Admit | URGENT |
| Exfoliative dermatitis (major) | Admit | URGENT |
| Cellulitis (severe/systemic signs) | Admit | URGENT |
| Angioedema (laryngeal) | Admit - ICU | AIRWAY EMERGENCY |
| Herpes zoster (immunocompromised) | Admit for IV acyclovir | URGENT |
| Cellulitis (mild, no systemic signs) | Discharge with 2-3 day follow-up + skin marking | ROUTINE |
| EM minor | Discharge with PCP/derm follow-up | ROUTINE |
| Urticaria (mild/moderate) | Discharge + antihistamines | ROUTINE |
| Scabies | Discharge + permethrin + contact treatment | ROUTINE |
| Tinea/fungal | Discharge + antifungal | ROUTINE |
| Contact dermatitis (mild) | Discharge + topical steroids | ROUTINE |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Chapters 14, 152, 192-193, 248-253
- Rosen's Emergency Medicine: Concepts and Clinical Practice - Chapters 84, 118, 152
Secondary lesions, Labs and management of skin disorders in Emergency room
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I have all the content needed for a comprehensive, organized response. Let me now compile the full answer.
Secondary Lesions, Diagnostic Labs, and Management of Skin Disorders in the Emergency Room
Source: Tintinalli's Emergency Medicine (Ch. 246-249, 251) and Rosen's Emergency Medicine
PART 1 - SKIN LESION MORPHOLOGY
Primary vs. Secondary Lesions
Primary lesions arise directly from pathophysiological processes.
Secondary lesions have had their appearance altered due to disease evolution or external factors (scratching, trauma, treatment).
"Secondary lesions...include crusts, scales, fissures, erosions, ulcerations, excoriations, atrophy, scarring, and lichenification." - Tintinalli TABLE 248-3
TINTINALLI TABLE 248-3 - Complete Lesion Morphology
PRIMARY LESIONS:
| Descriptor | Morphology | Height |
|---|---|---|
| Macule | Flat, circumscribed discoloration ≤1 cm; color varies | Flat |
| Patch | Flat, circumscribed discoloration >1 cm | Flat |
| Papule | Solid, elevated lesion ≤1 cm | Elevated |
| Plaque | Elevated, flat-topped lesion >1 cm; may be formed by coalescence of papules | Elevated |
| Wheal | Transient, edematous, variably sized papule or plaque; evanescent (urticaria) | Elevated |
| Vesicle | Fluid-filled blister ≤1 cm; clear or hemorrhagic | Elevated |
| Bulla | Fluid-filled blister >1 cm | Elevated |
| Pustule | Vesicle filled with purulent fluid | Elevated |
| Nodule | Palpable solid lesion <1 cm | Elevated |
| Tumor | Palpable solid lesion >1 cm | Elevated |
| Cyst | Sac containing liquid or semi-solid material | Elevated |
| Abscess | Tender, erythematous, fluctuant nodule filled with pus | Elevated |
| Petechiae | Nonblanching purple spots <2 mm | Flat |
| Purpura | Nonblanching purple discoloration of skin (>3 mm) | Flat |
| Telangiectasia | Small, blanchable superficial capillaries | Flat |
SECONDARY LESIONS:
| Descriptor | Morphology | Height |
|---|---|---|
| Scale | Accumulation of dead stratum corneum cells (keratin flakes) | Elevated |
| Crust | Dried serum, blood, or pus overlying damaged epidermis | Elevated |
| Lichenification | Thickened skin with exaggerated skin markings from chronic rubbing | Elevated |
| Excoriation | Linear marks from scratching - breaks the epidermis | Flat/depressed |
| Erosion | Loss of epidermis only; moist, shallow; heals without scarring | Depressed |
| Ulcer | Full-thickness epidermal or dermal tissue loss; heals with scarring | Depressed |
| Fissure | Linear crack in the skin surface (heel, fingertip, anal) | Flat |
| Scar | Sclerotic area of skin following tissue repair | Flat or elevated |
| Keloid | Hypertrophied scar extending beyond wound margins | Elevated |
| Atrophy | Thinning of epidermis or dermis; shiny, wrinkled skin | Depressed |
| Sclerosis | Firm, indurated skin | Flat or elevated |
TINTINALLI TABLE 248-2 - Lesion Configuration Descriptors
| Configuration | Meaning |
|---|---|
| Annular | Ring-like |
| Arcuate | Curved |
| Confluent | Blending together |
| Dermatomal | Belt-like, unilateral, follows anatomic dermatome |
| Discrete | Separate, individual lesions |
| Grouped / Herpetiform | Clustered |
| Guttate | Scattered ("drop-like") |
| Iris | Concentric circles (target lesion) |
| Linear | In a line |
| Retiform | Net-like (purpura fulminans) |
| Serpiginous | Snake-like |
TINTINALLI TABLE 248-4/5 - Differential Diagnosis by Lesion Morphology
Primary Lesion Morphology → Key Differentials:
| Lesion | Key Diagnoses to Consider |
|---|---|
| Macule | Drug eruption, nevus, viral exanthem, secondary syphilis, meningococcemia (early), ecchymosis, vitiligo, tinea versicolor, early cellulitis |
| Papule | Acne, warts, molluscum contagiosum, atopic dermatitis, urticaria, folliculitis, vasculitis, psoriasis, scabies, poison ivy, erythema multiforme, varicella (early), gonococcemia |
| Plaque | Eczema, pityriasis rosea, tinea corporis/versicolor, psoriasis, seborrheic dermatitis, urticaria, secondary syphilis, erythema multiforme |
| Nodule | Basal cell/squamous cell/metastatic carcinoma, melanoma, erythema nodosum, furuncle, lipoma |
| Wheal | Urticaria, angioedema, insect bites, erythema multiforme |
| Pustule | Acne, folliculitis, gonococcemia, herpes (zoster, simplex, varicella), impetigo, psoriasis, pyoderma gangrenosum |
| Vesicle | HSV, herpes zoster, varicella, impetigo, poison ivy/oak, thermal burn, friction blister, TEN, bullous pemphigoid, pemphigus vulgaris |
| Bulla | Bullous impetigo, poison ivy/oak, thermal burn, TEN, bullous pemphigoid, pemphigus vulgaris |
Secondary Lesion Morphology → Key Differentials:
| Lesion | Key Diagnoses to Consider |
|---|---|
| Scales | Psoriasis, pityriasis rosea, toxic/infectious erythemas, secondary syphilis, tinea, tinea versicolor, xerosis, first-degree thermal burn |
| Crusts | Eczema, tinea, impetigo, contact dermatitis, insect bite |
| Erosions | Candidiasis, tinea, varicella, HSV, impetigo, pemphigus vulgaris, SJS |
| Ulcers | Diabetic/venous/arterial ulcer, syphilis (chancre), chanroid, pyoderma gangrenosum, pressure ulcer |
| Excoriations | Scabies, atopic dermatitis, any pruritic dermatosis |
| Fissures | Athlete's foot, cheilitis, anal fissure, xerosis |
| Lichenification | Atopic/contact dermatitis (chronic), lichen simplex chronicus |
Distribution Pattern → Differential Diagnosis (Tintinalli TABLE 246-1)
| Distribution | Differential Diagnosis |
|---|---|
| Flexor surfaces | Atopic dermatitis, candidiasis, eczema, ichthyosis |
| Sun-exposed areas (face, upper thorax, distal extremities) | Sunburn, photosensitive drug eruption, SLE, viral exanthem, porphyria |
| Distal extremities | Viral exanthem, atopic/contact dermatitis, eczema, Rocky Mountain spotted fever, gonococcemia |
| Front and back of chest | Pityriasis rosea, secondary syphilis, drug eruption, psoriasis, atopic/contact dermatitis |
| Clothing-covered areas | Contact dermatitis, psoriasis, folliculitis |
| Face + upper thorax (acneiform) | Acne, drug-induced acne, irritant dermatitides |
PART 2 - DIAGNOSTIC TESTS FOR SKIN DISORDERS IN THE ED
(Tintinalli Ch. 248 - Diagnostic Approach)
1. Potassium Hydroxide (KOH) Preparation
Uses: Dermatophyte infections (tinea), molluscum contagiosum, pityriasis versicolor
Specimen sources: Loose skin scales, nail parings, subungual debris, short residual hairs, small pearly globules (from molluscum body)
KOH Prep Steps (Tintinalli TABLE 248-6):
- Place skin scrapings on a glass slide
- Add a coverslip
- Apply KOH 10-40% solution to the edge of the coverslip - it will be drawn under by capillary action
- Apply heat to the underside of the slide (match or lighter) until bubbles appear under coverslip
- Visualize under 10× magnification; use low condenser and light settings; focus up and down rapidly
Findings:
- True hyphae (dermatophyte infection): long, branching green rods of constant width that cross cell borders
- Molluscum bodies: oval discs with homogeneous cytoplasm
- Spores in hair: small, round spores packed closely within the hair shaft (endothrix = Trichophyton; ectothrix = Microsporum)
2. Tzanck Smear
Uses: Diagnose herpetic infections - HSV-1, HSV-2, varicella-zoster virus
"The presence of the multinucleated giant cell does not distinguish between herpes simplex, herpes zoster, and varicella syndromes." - Tintinalli
Specimen: Scrape the base of a recently unroofed vesicle or pustule; remove purulent fluid from base with scalpel; place on microscope slide
Steps:
- Air-dry the specimen
- Stain with Giemsa or Wright stain
- View under low power - scan for epithelial cells
- Positive finding: multinucleated giant cells (syncytium of epidermal cells with multiple overlapping nuclei)
Limitation: Does not differentiate HSV-1, HSV-2, or VZV; NAATs (PCR) are more sensitive and specific for definitive typing
3. Wood's Lamp Examination
Mechanism: UV light source at 365 nm wavelength
Fluorescent findings (Tintinalli):
| Condition / Organism | Fluorescence Color |
|---|---|
| Erythrasma (Corynebacterium minutissimum) | Red or pink (coral-red) |
| Tinea capitis (Microsporum species) | Green or yellow |
| Tinea versicolor (Malassezia species) | Green or yellow |
| Pseudomonas skin infection | Yellow or green |
| Porphyria cutanea tarda | Urine fluoresces orange or red |
| Nits (lice eggs) | Fluoresce |
Note: >90% of tinea capitis is due to Trichophyton species which do NOT fluoresce - Wood's lamp has limited utility for tinea capitis in most regions.
Other uses: Detect extent of melasma (darker under Wood's lamp), assess depigmentation in vitiligo
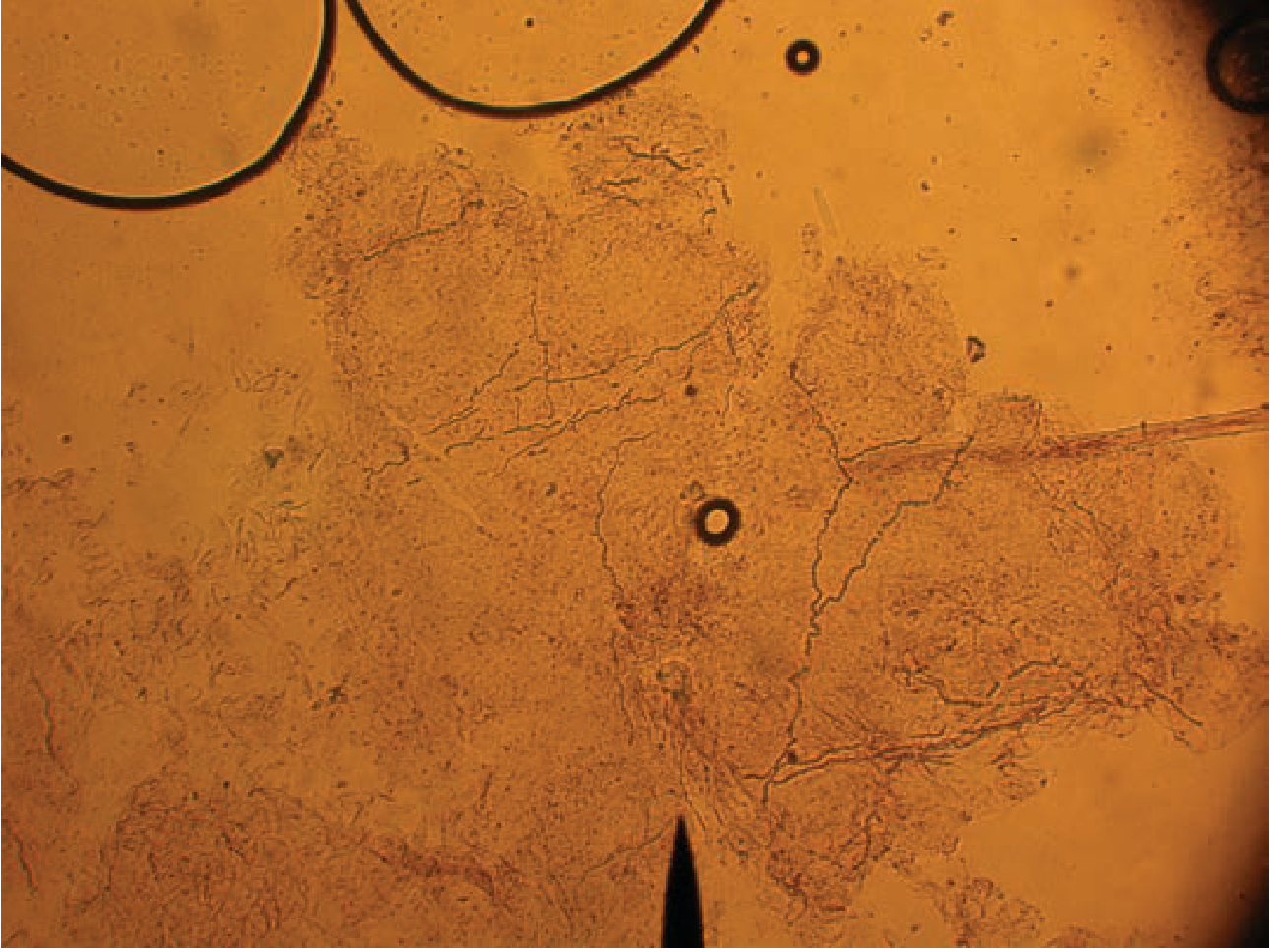
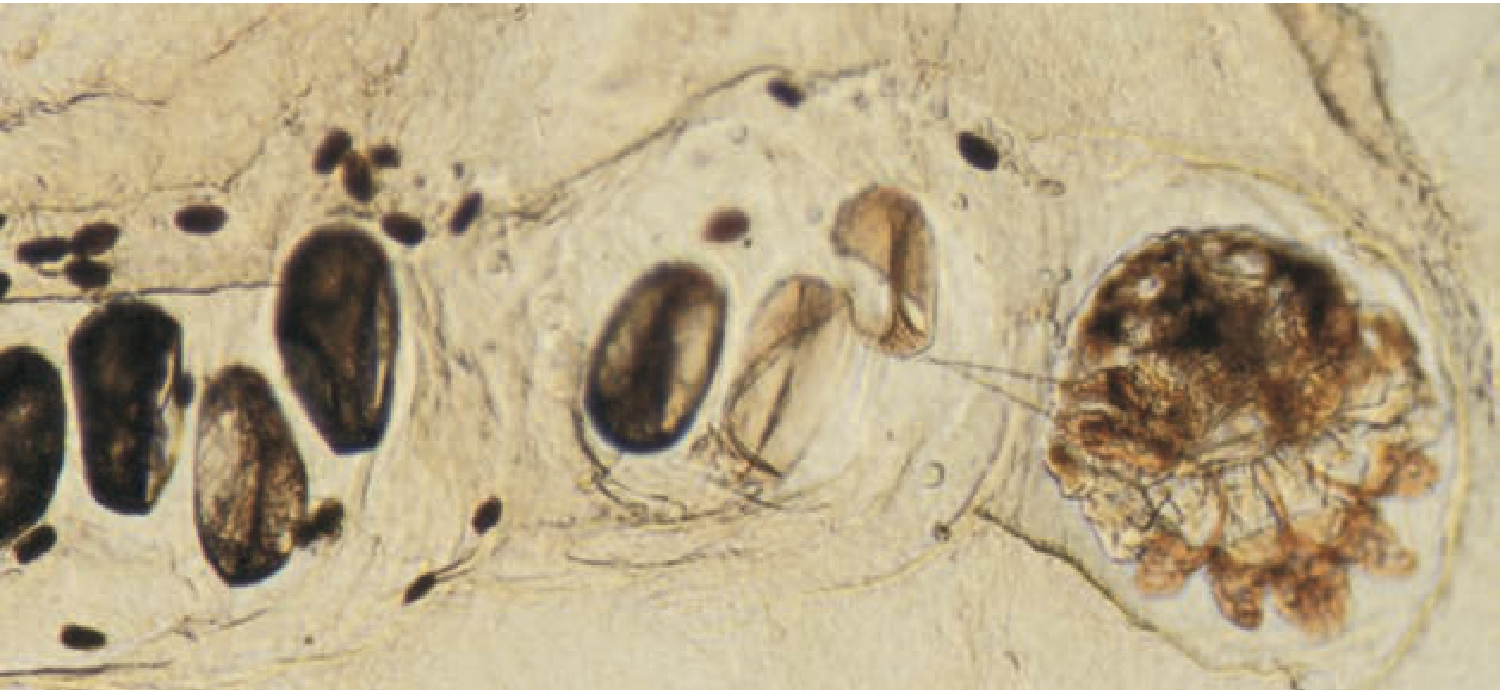
4. Scabies Preparation
Best sites for specimen: Burrows (10 mm elongated papule with vesicle/pustule) on fingers, wrists, elbows
Steps:
- Identify burrow - a small black dot within represents the mite
- Apply a single drop of mineral oil to scalpel blade (keeps scrapings adherent)
- Hold skin taut; scrape across the lesion with scalpel tip
- Place material on slide with additional mineral oil drop; add coverslip
- View under low power
Positive findings:
- Mite (8-legged creature)
- Eggs (smooth ovals)
- Feces (clusters of red-brown pellets)
5. Lice Preparation
Lice are usually found on scalp, eyelashes, and pubic areas - may be visible to the naked eye.
Nits (eggs) adhere to the hair shaft; confirm by microscopy.
6. Ancillary Labs for Systemic Assessment
(Tintinalli Ch. 248 - ED Diagnosis)
"Ancillary studies may also be required to assess for systemic involvement." - Tintinalli
| Lab Finding | What It Suggests |
|---|---|
| Fever + leukocytosis | Underlying infectious disorder or autoimmune reaction |
| Elevated transaminases (patient on anticonvulsant) | DRESS syndrome - hepatic involvement |
| DIC (↑PT/PTT, ↓fibrinogen, ↓platelets, ↑D-dimer) | Bacteremia, meningococcemia, purpura fulminans, toxic shock syndrome |
| Thrombocytopenia | Bacteremia, sepsis, toxic shock, TTP |
| Acute kidney injury (↑creatinine) | Meningococcemia (DIC), DRESS, TEN |
| Eosinophilia (>500/µL) | DRESS syndrome (present in ~30%) |
| Hyperglycemia | Necrotizing fasciitis, severe sepsis (also SCORTEN factor for TEN mortality) |
| Hyponatremia (<135) | Necrotizing fasciitis (LRINEC score) |
| CRP >150 mg/L | Necrotizing fasciitis (highest LRINEC weight = +4 points) |
| Blood cultures | Meningococcemia, necrotizing fasciitis with sepsis, cellulitis with systemic signs |
| ASO titer | Group A streptococcal infection |
Imaging:
- CT scan: assess depth of tissue involvement; gas tracking along fascial planes in necrotizing fasciitis; detect foreign bodies
- X-ray: subcutaneous gas in necrotizing fasciitis/gas gangrene
- Ultrasound: differentiate abscess from cellulitis; guide I&D; assess depth of soft tissue infection; detect foreign bodies
7. Skin Biopsy (ED Context)
Indications in the ED:
- Confirm diagnosis of TEN/SJS (frozen section if available - rapid diagnosis)
- Rule out malignancy (referral basis)
- Bullous disorders (pemphigus vs. pemphigoid - direct immunofluorescence needed)
- Vasculitis confirmation
Tintinalli on SJS/TEN biopsy: Histology shows lymphocytic infiltrate at dermoepidermal junction with keratinocyte necrosis - often full-thickness; cellular necrosis out of proportion to infiltrate.
PART 3 - ED MANAGEMENT FRAMEWORK
STEP 1: Identify Emergencies First
Tintinalli trigger signs for immediate action:
| Sign | Consider |
|---|---|
| Widespread skin sloughing / positive Nikolsky sign | SJS/TEN → stop drug, admit ICU/burn unit |
| Petechiae + fever + ill-appearing | Meningococcemia → IV ceftriaxone STAT |
| Pain out of proportion to skin findings + systemic toxicity | Necrotizing fasciitis → surgical consult STAT |
| Skin + eosinophilia + organ dysfunction | DRESS → stop drug, admit |
| >90% BSA erythema + systemic compromise | Erythroderma → admit, thermoregulation |
| Angioedema approaching larynx | Secure airway; C1 inhibitor/icatibant/epinephrine |
STEP 2: Systemic Corticosteroids
(Tintinalli Ch. 248 - ED Treatment)
"Some severe widespread dermatologic syndromes, such as erythema multiforme, toxic epidermal necrolysis, and vasculitis, are best treated with systemic steroids only after consultation with a dermatologist."
Use systemic steroids without dermatology consult for:
- Urticaria and angioedema
- Contact/allergic dermatitis (Toxicodendron/poison ivy)
- Other allergic reactions
Systemic steroid protocols:
| Condition | Regimen |
|---|---|
| Severe contact dermatitis / poison ivy | Prednisone 0.5 mg/kg/day × 2-3 weeks taper |
| SJS (EM major) | Methylprednisolone 125 mg IV q6h (or equivalent) |
| DRESS (severe) | Prednisone 1-2 mg/kg/day; taper slowly over weeks-months |
| Exfoliative dermatitis | Only after dermatology consult |
| Urticaria/angioedema | Methylprednisolone 125 mg IV (or equivalent oral) |
STEP 3: Antihistamines - Dosing Table
(Tintinalli TABLE 248-8)
| Drug | Adult Dose | Pediatric Dose | Class |
|---|---|---|---|
| Diphenhydramine (Benadryl) | 25-50 mg PO/IV/IM QID | 5 mg/kg/day in 4 divided doses (max 300 mg/day) | H1 (sedating) |
| Hydroxyzine | 25-100 mg PO TID-QID | 2 mg/kg/day PO in 4 divided doses | H1 (sedating) |
| Cetirizine (Zyrtec) | 5-10 mg PO once daily | ≥6 years: 5-10 mg PO once daily | H1 (non-sedating) |
| Fexofenadine (Allegra) | 60 mg PO BID | ≥6 years: 30 mg PO BID | H1 (non-sedating) |
| Loratadine (Claritin) | 10 mg PO once daily | ≥6 years: 10 mg PO once daily | H1 (non-sedating) |
| Famotidine (Pepcid) | 20 mg PO BID | 0.5 mg/kg/day in 2 divided doses (max 40 mg/day) | H2 (adjunct in severe reactions) |
| Ranitidine (Zantac) | 150 mg PO BID | 5-10 mg/kg/day in 2 divided doses (max 300 mg/day) | H2 (adjunct) |
STEP 4: Topical Corticosteroids - Potency Classification
(Tintinalli TABLE 248-7)
| US Group | Potency | Representative Agents |
|---|---|---|
| 1 - Superpotent | Very Potent | Clobetasol (Temovate) 0.05% cream/ointment; Halobetasol 0.05%; Betamethasone (Diprolene) |
| 2 - Potent | Potent | Fluocinonide (Lidex) 0.05% ointment; Halcinonide 0.1% cream; Mometasone (Elocon) 0.1% ointment |
| 3 - Upper mid-strength | Betamethasone (Diprolene) 0.05% lotion; Fluticasone (Cutivate) 0.005% ointment; Triamcinolone 0.1% ointment | |
| 4 - Mid-strength | Mometasone (Elocon) 0.1% cream/lotion | |
| 5 - Lower mid-strength | Moderate | Betamethasone 0.1% cream; Fluocinolone (Synalar) 0.025% cream; Fluticasone (Cutivate) 0.05% cream |
| 6 - Mild | Alclometasone 0.05%; Desonide (Desonate) 0.05% cream; Triamcinolone 0.025% cream | |
| 7 - Least Potent | Mild | Hydrocortisone 1% or 2.5% cream/lotion/ointment |
Body area selection rule:
- Face, intertriginous areas, children: Low potency (Group 6-7) only
- Extremities, trunk: Intermediate (Group 3-5)
- Thick plaques (psoriasis, palms, soles): High potency (Group 1-2)
- Never use superpotent steroids on face, groin, or under occlusion chronically
STEP 5: Topical Antibiotics
(Tintinalli Ch. 248)
| Agent | Use |
|---|---|
| Mupirocin (Bactroban) 2% | Impetigo - as effective as oral antibiotics for superficial skin infection |
| Polymyxin B | Wound dressing adjunct; reduce bacterial colonization |
| Bacitracin | Wound dressing; prevent adherence of dressings to wounds |
| Neomycin | Combined wound dressings (note: common sensitizer - contact allergy risk) |
| Silver sulfadiazine | Burn wounds; do NOT apply to face (causes staining); wipe off prior application before reapplying |
| Oral tetracycline rinses | Aphthous stomatitis |
"Topical antibacterial agents are rarely useful as primary therapy for superficial bacterial infections of the skin. The exception is topical mupirocin." - Tintinalli
STEP 6: Antipruritic (Non-Steroidal) Agents
(Tintinalli Ch. 248)
| Agent | Dose | Notes |
|---|---|---|
| Capsaicin 0.025% topical | Apply TID × up to 4 weeks | Desensitizes nerve fibers via substance P depletion; not for age <10 years |
| Pramoxine 1-2% | Apply as directed | Topical anesthetic; limited evidence |
| EMLA (lidocaine 2.5% + prilocaine 2.5%) | Apply as directed | Topical anesthetic for pruritus; evidence limited |
| Domeboro solution (aluminum sulfate 1:10) | Soaks/compresses | Astringent; relieves weeping, pruritic lesions |
| Oatmeal baths | As needed | Soothing antipruritic for widespread pruritus |
| Open wet dressings (tap water or saline) | TID | Cleanse crusts and exudates painlessly; reduce discomfort |
| Emollients/moisturizers | After bathing while skin still moist | Restore water and lipids; reduce pruritus and tightness |
PART 4 - MANAGEMENT SUMMARY BY SECONDARY LESION TYPE
| Secondary Lesion | Most Common Diagnoses | ED Management |
|---|---|---|
| Scales | Psoriasis, tinea, pityriasis rosea, drug eruption | KOH prep → antifungals or topical steroids |
| Crusts | Impetigo, eczema, contact dermatitis | Mupirocin for impetigo; wet compresses to loosen crusts; topical steroids for eczema |
| Erosions | HSV, pemphigus, candida, impetigo | Tzanck smear → antivirals; antifungals; wound care |
| Ulcers | Syphilis, chanroid, diabetic/pressure ulcers | STI testing; wound care; appropriate antibiotics; vascular/wound surgery referral |
| Fissures | Tinea pedis, xerosis, anal fissure | Antifungals; emollients; topical steroids; stool softeners |
| Excoriations | Scabies, atopic dermatitis | Scabies prep → permethrin; antihistamines; topical steroids |
| Lichenification | Chronic eczema, lichen simplex | High-potency topical steroids; antihistamines for itch-scratch cycle |
| Crusted + weeping vesicles | Herpes zoster, impetigo, contact dermatitis | Tzanck; NAATs; antivirals; wet compresses; mupirocin |
| Purpura (non-blanching) | Meningococcemia, vasculitis, ITP | URGENT: blood cultures, CBC, coagulation; IV antibiotics if meningococcemia suspected |
| Bullae | TEN, SJS, pemphigus, bullous impetigo | SCORTEN; stop drug; burn/ICU care; IV antibiotics for impetigo |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Tables 246-1, 248-2, 248-3, 248-4, 248-5, 248-6, 248-7, 248-8, 248-9, 248-10 (Chapters 246, 248-249)
- Rosen's Emergency Medicine: Concepts and Clinical Practice - Chapter 84 (STIs), Chapter 118 (Meningococcemia)
This is a shared conversation. Sign in to Orris to start your own chat.