What is shop and what are its types?
Searching the Web
types of shops retail establishments explained
What is shock? And what are its type? According to physiology.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have thorough content from multiple authoritative textbooks. Here is the complete answer:
Shock - Physiology
Definition
Shock is a state of systemic tissue hypoperfusion - a condition in which the cardiac output is relatively or absolutely inadequate to maintain sufficient perfusion of tissues, leading to cellular hypoxia. At its core, every form of shock results in an imbalance between oxygen delivery and oxygen demand at the tissue level.
"Circulatory shock comprises a collection of different entities that share certain common features; however, the feature common to all the entities is inadequate tissue perfusion with a relatively or absolutely inadequate cardiac output."
- Ganong's Review of Medical Physiology
The Four Major Types of Shock
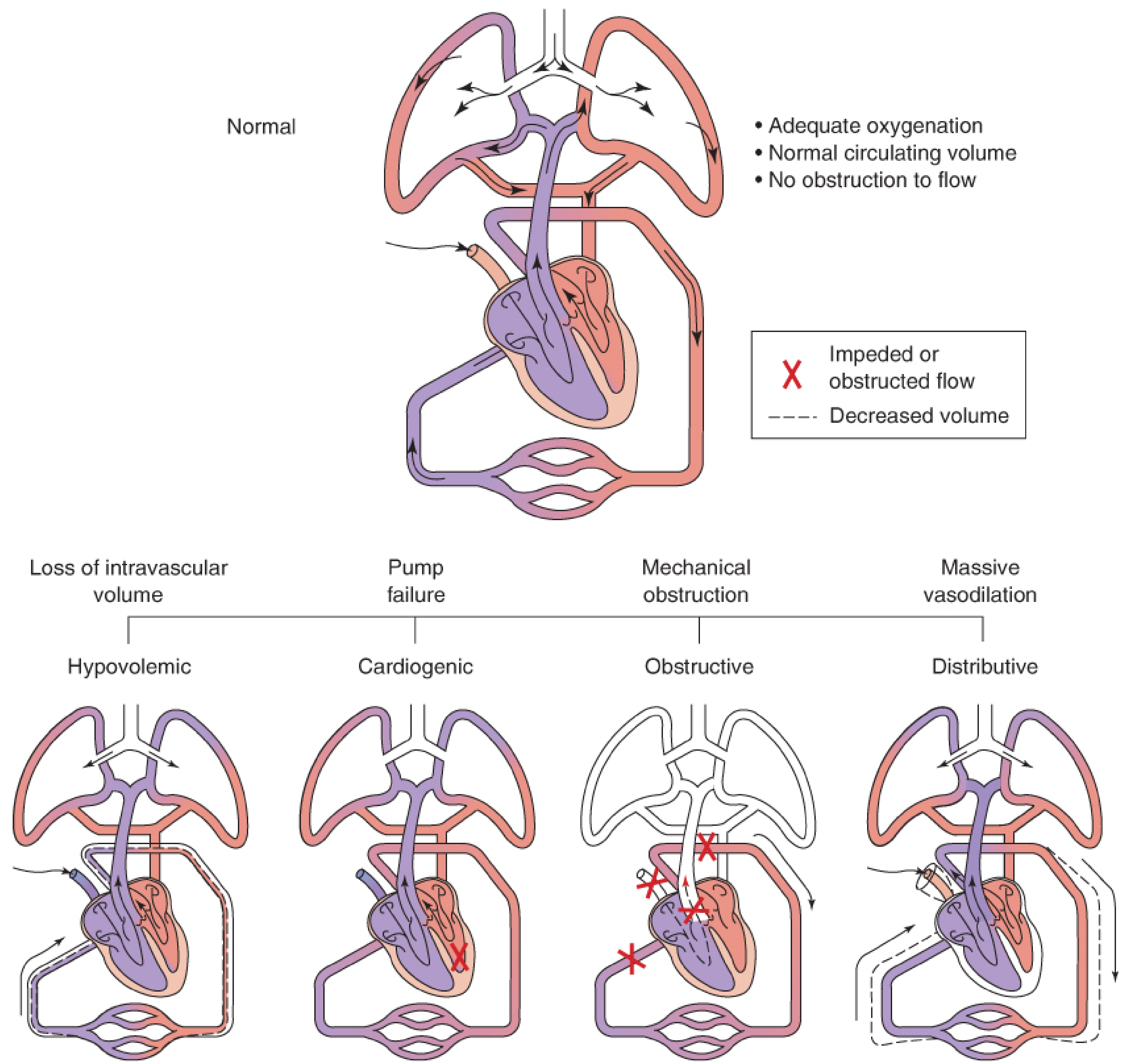
1. Hypovolemic Shock (also called "Cold Shock")
Mechanism: Loss of intravascular volume - the vascular system is inadequately filled.
Causes:
- Hemorrhage (most common)
- Severe burns (plasma loss)
- Severe dehydration, diarrhea, vomiting
Physiological features:
- Hypotension
- Rapid, thready pulse
- Cold, pale, clammy skin
- Intense thirst
- Rapid respiration
- Restlessness or torpor
Key physiology: When blood volume drops, venous return decreases and cardiac output falls. Arterial baroreceptor stimulation is reduced, triggering sympathetic activation - causing reflex tachycardia and vasoconstriction (sparing brain and heart). Severe cases develop lactic acidosis (lactate rising from 1 mmol/L up to 9 mmol/L), which depresses the myocardium and decreases vascular responsiveness to catecholamines. Prolonged hypotension can cause acute kidney injury.
(Ganong's Review of Medical Physiology)
2. Cardiogenic Shock
Mechanism: Pump failure - the heart cannot generate sufficient output despite adequate volume.
Causes:
- Myocardial infarction (most common)
- Severe ventricular arrhythmia
- Cardiac tamponade (extrinsic compression)
- End-stage cardiomyopathy
Key physiology: The cardiac output is absolutely reduced due to intrinsic myocardial dysfunction. Unlike hypovolemic shock, the problem is not volume but the pump itself. Ventricular function is compromised, leading to elevated filling pressures and decreased forward flow.
(Robbins & Kumar Basic Pathology; Ganong's Physiology)
3. Distributive Shock (Vasogenic / Low-Resistance Shock)
Mechanism: Massive vasodilation - the vascular system is pathologically enlarged even though blood volume is normal. Cardiac output may actually be high, but perfusion is maldistributed.
This category includes three major subtypes:
| Subtype | Trigger | Mechanism |
|---|---|---|
| Septic shock | Bacterial/fungal infection | Microbial PAMPs activate innate immunity, causing massive cytokine release, endothelial injury, and vasodilation |
| Anaphylactic shock | IgE-mediated hypersensitivity | Systemic vasodilation + increased vascular permeability |
| Neurogenic shock | Spinal cord injury or deep anesthesia | Loss of sympathetic vascular tone |
Septic shock physiology (detailed): Microbial constituents engage Toll-like receptors (TLRs), G-protein-coupled receptors, and C-type lectin receptors on macrophages, neutrophils, and dendritic cells. This triggers a massive outpouring of inflammatory mediators causing: arterial vasodilation, vascular leakage, venous blood pooling, and ultimately organ hypoperfusion and failure. Mortality remains 20-30% despite modern care.
(Robbins & Kumar Basic Pathology)
4. Obstructive Shock
Mechanism: Mechanical obstruction to blood flow in the great vessels, lungs, or heart - physically blocking adequate cardiac output.
Causes:
- Pulmonary embolism (blocks right ventricular outflow)
- Tension pneumothorax (compresses vena cava)
- Cardiac tamponade (pericardial fluid compresses heart)
Key physiology: Despite a structurally normal heart and adequate volume, flow is physically obstructed. The physiology is often similar to cardiogenic shock in its hemodynamic profile (low cardiac output, elevated filling pressures).
(Fischer's Mastery of Surgery; Ganong's Physiology)
Summary Table
| Type | Core Problem | Cardiac Output | SVR | Example |
|---|---|---|---|---|
| Hypovolemic | Low volume | ↓ | ↑ | Hemorrhage, burns |
| Cardiogenic | Pump failure | ↓ | ↑ | MI, tamponade |
| Distributive | Vasodilation | ↑ or normal | ↓↓ | Sepsis, anaphylaxis |
| Obstructive | Flow blocked | ↓ | ↑ | PE, tension pneumothorax |
SVR = Systemic Vascular Resistance
Stages of Shock (General)
- Compensated (reversible) - Compensatory mechanisms (sympathetic activation, vasoconstriction, tachycardia) maintain perfusion. Cellular injury is reversible.
- Progressive (decompensated) - Compensatory mechanisms fail; lactic acidosis worsens; tissue injury worsens.
- Irreversible - Widespread cell death, multi-organ failure; often fatal despite treatment.
Sources:
- Ganong's Review of Medical Physiology, 26th Ed., Chapter on Circulation
- Robbins & Kumar Basic Pathology, Chapter 3
- Fischer's Mastery of Surgery, 8th Ed., Chapter 265
How does action potential in... How does ac- action potential in the cardiac muscle occurs? I need complete... Like... A detailed view on this topic.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
I now have comprehensive, detailed content from Braunwald's Heart Disease, Costanzo Physiology, and Goodman & Gilman's. Let me compose the full answer.
Action Potential in Cardiac Muscle - A Detailed Physiological View
What is a Cardiac Action Potential?
The cardiac action potential (AP) is a time-dependent change in the voltage difference between the inside and outside of a cardiac cell. It is generated by sequential opening and closing of ion channels (Na⁺, Ca²⁺, K⁺) in the cell membrane, which allow charged ions to flow down their electrochemical gradients.
Unlike skeletal muscle action potentials (which last ~2 ms), the cardiac AP lasts 200-400 ms - a feature that is physiologically essential to prevent tetanic contraction and allow the heart to refill between beats.
"Transmembrane current through voltage-gated ion channels is the primary determinant of cardiac action potential morphology and duration."
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Resting Membrane Potential (Phase 4 - in Ventricular Muscle)
Before any action potential fires, the cardiac cell sits at a resting membrane potential of -80 to -90 mV (for ventricular and His-Purkinje cells). This negative interior voltage is maintained by:
- Inward-rectifier K⁺ channels (I_K1): K⁺ is at ~150 mM inside and ~4 mM outside. K⁺ tends to leave the cell down its chemical gradient, leaving negative charges behind and making the interior negative.
- Na⁺/K⁺-ATPase pump: Actively pumps 3 Na⁺ out and 2 K⁺ in, maintaining the gradients.
- The Na⁺ equilibrium potential (E_Na) is about +65 mV, while the K⁺ equilibrium potential (E_K) is about -94 mV.
Note: SA and AV node cells have a less negative resting potential of -50 to -65 mV because they have fewer I_K1 channels.
The Five Phases of the Cardiac Action Potential
The ventricular muscle action potential is divided into 5 phases (Phase 0-4):
Phase 0 - Rapid Depolarization (Upstroke)
Ion involved: Na⁺ (fast inward current)
When a cardiac myocyte is depolarized above threshold (~-70 mV) - usually by current arriving through gap junctions from an adjacent cell - voltage-gated fast Na⁺ channels (Nav1.5) rapidly open.
- Up to 10⁷ Na⁺ ions/sec rush into the cell per channel
- The membrane potential rapidly swings from -90 mV to about +20 to +30 mV
- This rapid rise is called the upstroke, measured as dV/dt (Vmax)
- Na⁺ channels then rapidly inactivate (close) - lasting only ~1 ms
- The rate of rise (dV/dt) is the major determinant of conduction velocity - the faster phase 0, the faster the impulse spreads
Phase 1 - Initial Rapid Repolarization
Ion involved: K⁺ (transient outward current, I_to)
Immediately after the peak of the upstroke, a brief, partial repolarization occurs:
- The inactivation gates on Na⁺ channels close - inward Na⁺ current ceases
- A transient outward K⁺ current (I_to) activates - K⁺ rushes out because both electrical (interior is positive) and chemical (high K⁺ inside) forces drive it outward
- This partial repolarization brings the membrane potential down slightly, setting the voltage level for the plateau (Phase 2)
Phase 2 - Plateau
Ions involved: Ca²⁺ (inward) balanced against K⁺ (outward)
This is the defining feature of the cardiac action potential and lasts 150-200 ms. The membrane potential hovers near 0 mV because inward and outward currents are nearly equal.
Inward current:
- L-type (long-lasting) Ca²⁺ channels (I_Ca,L) open - Ca²⁺ flows into the cell
- This Ca²⁺ entry triggers a massive Ca²⁺ release from the sarcoplasmic reticulum (SR) via ryanodine receptors - this is called Calcium-Induced Calcium Release (CICR)
- The surge in intracellular Ca²⁺ activates the contractile proteins (troponin C), causing myocyte contraction - this is electromechanical coupling
Outward current:
- Delayed rectifier K⁺ currents (I_Ks, I_Kr) slowly activate, partially counterbalancing the Ca²⁺ inward current
The plateau is the reason the cardiac AP is so long - it is protective against re-excitation during contraction (absolute refractory period).
Phase 3 - Final Rapid Repolarization
Ion involved: K⁺ (large outward current)
The plateau ends and the cell rapidly repolarizes back to -90 mV:
- L-type Ca²⁺ channels inactivate - inward Ca²⁺ current ceases
- Delayed rectifier K⁺ channels (I_Kr, I_Ks) are now fully activated - large outward K⁺ current sweeps the membrane back to negative
- Inward-rectifier K⁺ channels (I_K1) also contribute as membrane approaches negative voltages
The timing of Phase 3 sets the refractory period - the cell cannot be re-excited until it repolarizes below -60 mV.
Phase 4 - Resting Membrane Potential
In ventricular and atrial muscle cells, Phase 4 is a stable resting membrane potential at -85 to -90 mV. These cells do not spontaneously depolarize - they wait for an incoming signal.
In SA node pacemaker cells, Phase 4 is different (see below).
Summary Table of Phases
| Phase | Name | Key Ion | Channel | Effect |
|---|---|---|---|---|
| 0 | Rapid depolarization | Na⁺ in | Nav1.5 (fast) | Upstroke to +20 mV |
| 1 | Initial repolarization | K⁺ out | I_to | Brief notch |
| 2 | Plateau | Ca²⁺ in / K⁺ out | L-type Ca²⁺ / I_Ks, I_Kr | Contraction, long AP |
| 3 | Final repolarization | K⁺ out | I_Kr, I_Ks, I_K1 | Returns to rest |
| 4 | Resting potential | K⁺ | I_K1 | Stable -90 mV |
Refractory Periods
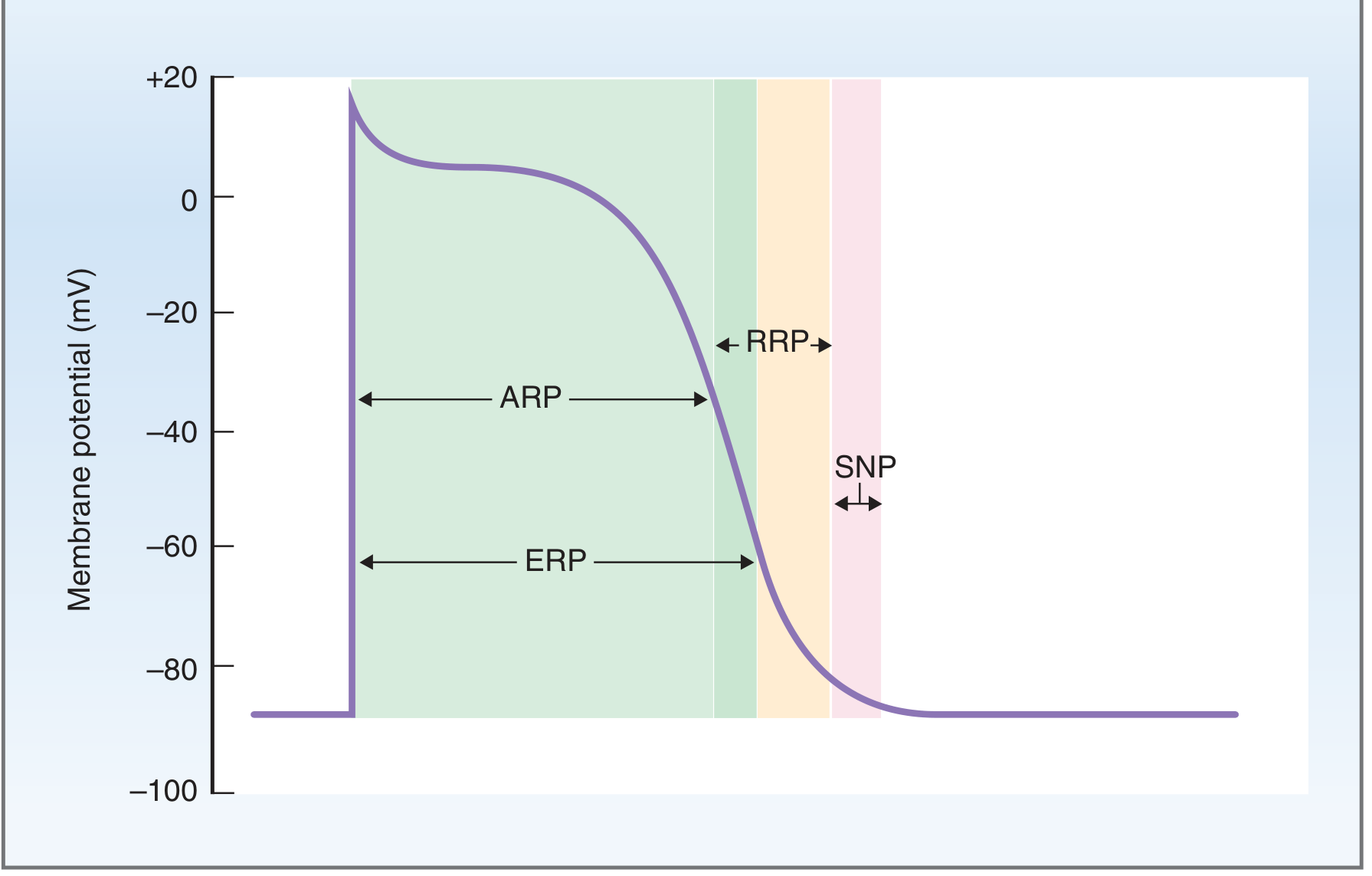
The refractory period exists because Na⁺ channels, once inactivated during Phase 0, cannot reopen until they recover during repolarization:
| Period | Timing | What Happens |
|---|---|---|
| Absolute Refractory Period (ARP) | Phase 0 through mid-Phase 3 | No stimulus, however large, can trigger another AP. Na⁺ channels are inactivated. |
| Effective Refractory Period (ERP) | ARP + early RRP | Functionally same as ARP |
| Relative Refractory Period (RRP) | Late Phase 3 | A larger-than-normal stimulus CAN fire an AP, but it is abnormal (slower upstroke) |
| Supranormal Period (SNP) | End of Phase 3 | Slightly sub-threshold stimulus can fire an AP - a window of vulnerability |
The long refractory period (matching the duration of contraction) prevents tetanus - the heart cannot be re-stimulated while it is contracting, which is essential for pumping function.
(Costanzo Physiology 7th Ed.)
The SA Node - Pacemaker Action Potential ("Slow Response")
The SA node generates spontaneous action potentials with a distinctly different shape, called the "slow response" AP:
- Resting potential: -50 to -65 mV (less negative, fewer I_K1 channels)
- No fast Phase 0: No fast Na⁺ channels; instead, the upstroke is carried by L-type Ca²⁺ channels - hence slower
- Phase 4 is NOT stable - it shows a slow spontaneous depolarization called the pacemaker potential
Pacemaker Potential Mechanism (Phase 4 in SA Node):
- After each AP, the membrane repolarizes to about -65 mV (maximum diastolic potential)
- A special current called I_f ("funny current") activates - carried by Na⁺ flowing inward through HCN channels
- I_f is called "funny" because it is turned ON by hyperpolarization (opposite of typical channels)
- This slow inward Na⁺ current gradually depolarizes the cell
- At about -40 mV, L-type Ca²⁺ channels open and produce the rapid upstroke
- The cycle repeats automatically, generating the heart rate (60-100 bpm)
"I_f is turned on by repolarization from the preceding action potential, thus ensuring that each action potential in the SA node will be followed by another action potential." - Costanzo Physiology
Conduction of the Action Potential Through the Heart
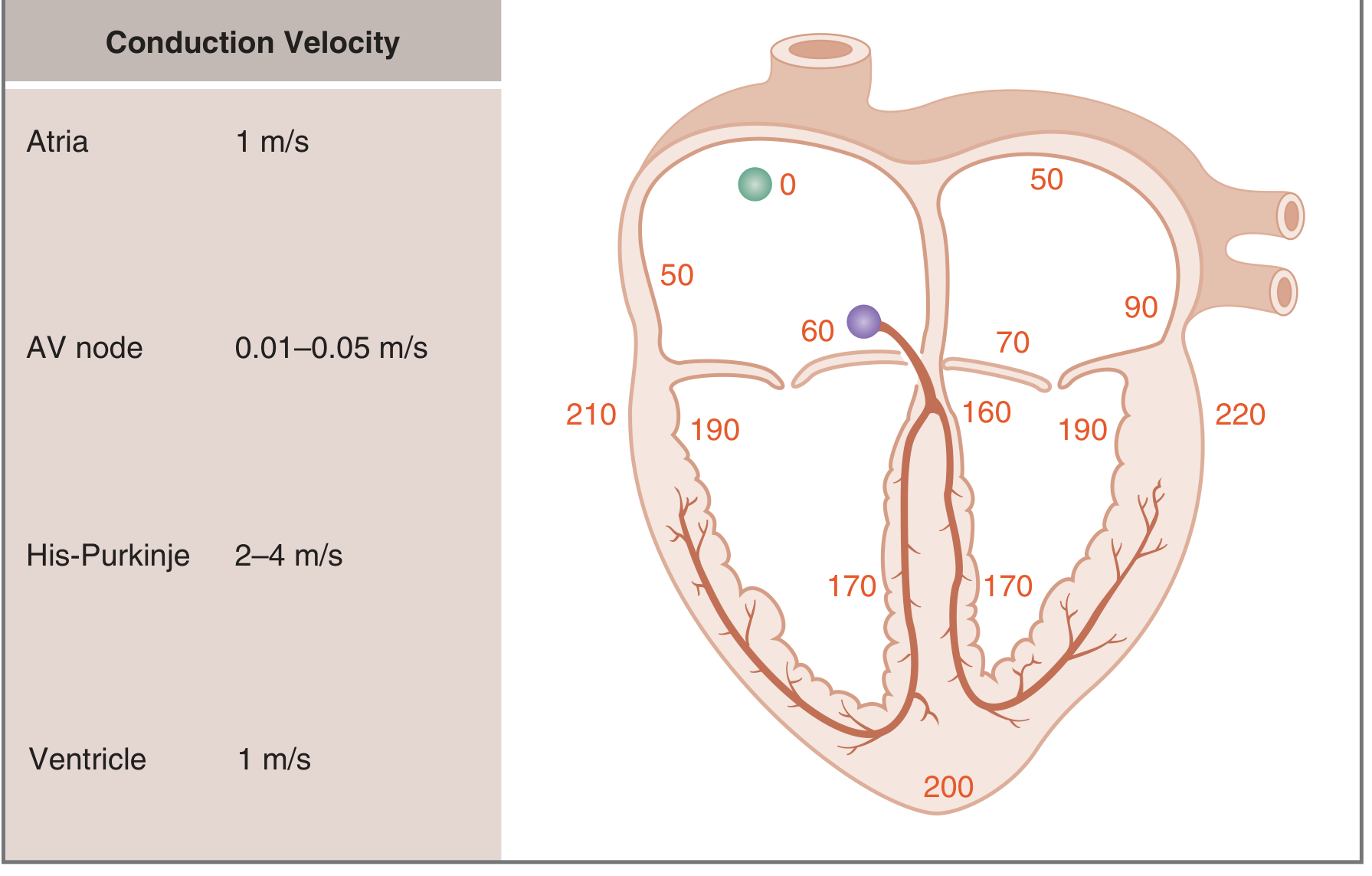
The AP spreads from cell to cell through gap junctions (low-resistance connections), which make the cardiac muscle act as a functional syncytium:
| Region | Conduction Velocity | Time from SA node |
|---|---|---|
| SA node (origin) | - | 0 ms |
| Atria | 1 m/s | ~50 ms |
| AV node | 0.01-0.05 m/s (SLOWEST) | ~60 ms |
| His bundle | - | ~130 ms |
| Purkinje fibers | 2-4 m/s (FASTEST) | ~160 ms |
| Ventricles | 1 m/s | ~220 ms |
Why is AV node slow? The deliberate delay (~100 ms) allows the atria to fully contract and empty blood into the ventricles before the ventricles are stimulated. Without this delay, the ventricles would contract before they are properly filled.
Why are Purkinje fibers fast? Rapid conduction ensures the ventricles activate quickly and in a coordinated sequence, producing efficient ejection.
The propagation of the AP depends on:
- Size of the inward Na⁺ current (larger = faster spread to adjacent cells)
- Cable properties of myocardium - especially the low internal resistance (Ri) provided by gap junctions
- dV/dT of the upstroke (correlates with inward current size)
(Costanzo Physiology 7th Ed.; Braunwald's Heart Disease)
Electromechanical Coupling Summary
Electrical stimulus → Phase 0 (Na⁺ in) → Phase 2 (Ca²⁺ in via L-type channels)
→ Ca²⁺ triggers SR Ca²⁺ release (CICR) → ↑ intracellular Ca²⁺
→ Ca²⁺ binds troponin C → cross-bridge cycling → CONTRACTION
→ Ca²⁺ pumped back into SR (SERCA) + out of cell (NCX) → RELAXATION
Sources:
- Braunwald's Heart Disease, 12th Ed. - Chapter 62: Cardiac Action Potential & Ion Channels
- Costanzo Physiology, 7th Ed. - Chapter 4: Cardiac Physiology
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Chapter 34
This is a shared conversation. Sign in to Orris to start your own chat.