Infective Endocarditis
Reading File
Finding Sources
Searching PubMed
"infective endocarditis"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to provide a comprehensive, well-structured response on Infective Endocarditis. Let me compile the full answer.
Infective Endocarditis (IE)
Definition
Infective endocarditis (IE) is a microbial infection of the heart valves or the mural endocardium that leads to the formation of vegetations composed of thrombotic debris and organisms, often associated with destruction of the underlying cardiac tissues. The aorta, aneurysms, prosthetic devices, and other blood vessels can also be infected. While fungi and other organisms can be responsible, the vast majority of cases are bacterial.
- Robbins & Kumar Basic Pathology, p. 368
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 528
Classification: Acute vs. Subacute
| Feature | Acute IE | Subacute IE |
|---|---|---|
| Virulence | Highly virulent (e.g., S. aureus) | Lower virulence (e.g., viridans streptococci) |
| Valve | Often previously normal | Deformed/damaged valve |
| Onset | Rapid (days) | Insidious (weeks to months) |
| Destruction | Severe, destructive | Less destructive, healing at base |
| Treatment | Usually requires surgery | Often cured with antibiotics alone |
| Prognosis | Worse | Better |
A clear delineation between the two forms does not always exist - many cases fall somewhere along the spectrum.
Epidemiology
-
Global incidence: ~13.8 per 100,000 (range 5.7-35.8 per 100,000)
-
Deaths due to IE have increased 131% since 1990, with ~66,322 deaths estimated
-
In-hospital mortality up to 22%; 5-year mortality up to 40%
-
The opioid epidemic has driven a surge in S. aureus IE from IV drug use (IVDU), particularly in rural US settings
-
In developing countries with endemic rheumatic fever: younger adults with subacute VGS IE
-
In developed countries/healthcare settings: older adults, S. aureus, acute IE
-
Fuster and Hurst's The Heart, 15th Edition
-
Braunwald's Heart Disease, Chapter on IE
Predisposing Conditions / Risk Factors
Cardiac:
- Prosthetic heart valves (10-20% of all IE)
- Previous IE
- Congenital heart disease (bicuspid aortic valve, unrepaired cyanotic CHD)
- Mitral valve prolapse (the leading pre-existent risk factor now that RHD has declined)
- Degenerative calcific valvular stenosis
- Rheumatic heart disease (still major in developing countries)
- Hypertrophic obstructive cardiomyopathy
- Ventricular assist devices, implantable cardiac devices
Non-cardiac:
- Intravenous drug use (IVDU)
- Indwelling vascular catheters / pacemaker leads
- Diabetes, immunodeficiency, malignancy, neutropenia, alcohol use
- Poor oral health / invasive dental procedures
Microbiology
| Organism | Context | Type |
|---|---|---|
| Streptococcus viridans (VGS) | Damaged valves, oral procedures, community-acquired | Subacute (50-60% of native valve IE) |
| Staphylococcus aureus | Skin, healthcare settings, IVDU, healthy valves | Acute - most common overall in high-income countries |
| Staphylococcus epidermidis | Prosthetic valves (early, <1 year) | Subacute/chronic |
| Enterococci | GI/GU procedures, older adults | Subacute |
| HACEK group* | Oral flora | Subacute |
| Gram-negative bacilli | Immunocompromised, IVDU | Rare |
| Fungi | Immunocompromised, prosthetic valves | Rare |
| Culture-negative (~10%) | Prior antibiotics, fastidious organisms | Variable |
*HACEK = Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella
Valve preferences:
- Left-sided: mitral (41.1%), aortic (37.6%) - community/healthcare IE
- Right-sided (tricuspid): characteristic of IVDU
Pathogenesis
- Bacteremia seeds the bloodstream (dental/surgical procedure, IVDU, trivial skin breaks, gut/oral flora)
- Endothelial disruption at sites of turbulent flow creates sterile platelet-fibrin deposits (non-bacterial thrombotic endocarditis, NBTE)
- Circulating organisms adhere to these sterile thrombi - especially when surface receptors (e.g., fibronectin-binding proteins on S. aureus) facilitate binding
- Organisms proliferate within the vegetation, protected from immune defenses (avascular structure - no direct blood supply, limited immune access)
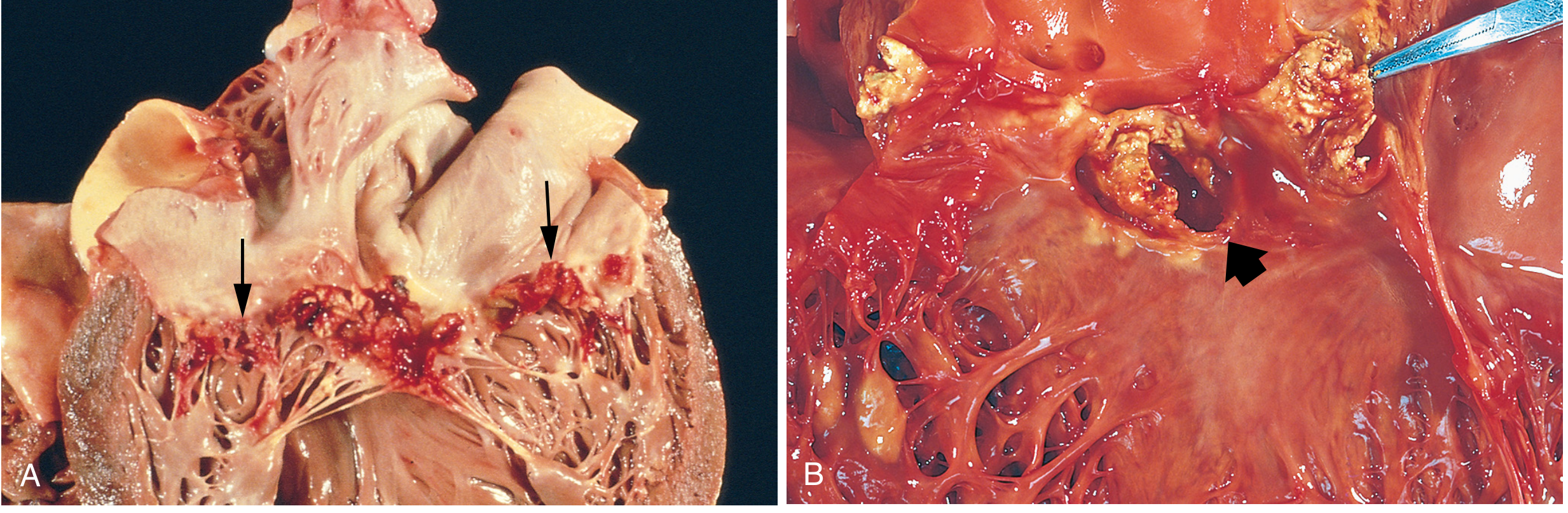
- The vegetation grows - friable, bulky, destructive - composed of fibrin, inflammatory cells, and organisms
Pathology / Morphology
Gross:
- Vegetations are the hallmark - friable, bulky masses on valve cusps (usually on the line of closure, atrial surface for AV valves, ventricular surface for semilunar valves)
- Can be single or multiple, can extend onto chordae tendineae
- Can erode into myocardium → ring abscess (perivalvular abscess)
- Aortic and mitral valves most common; tricuspid in IVDU
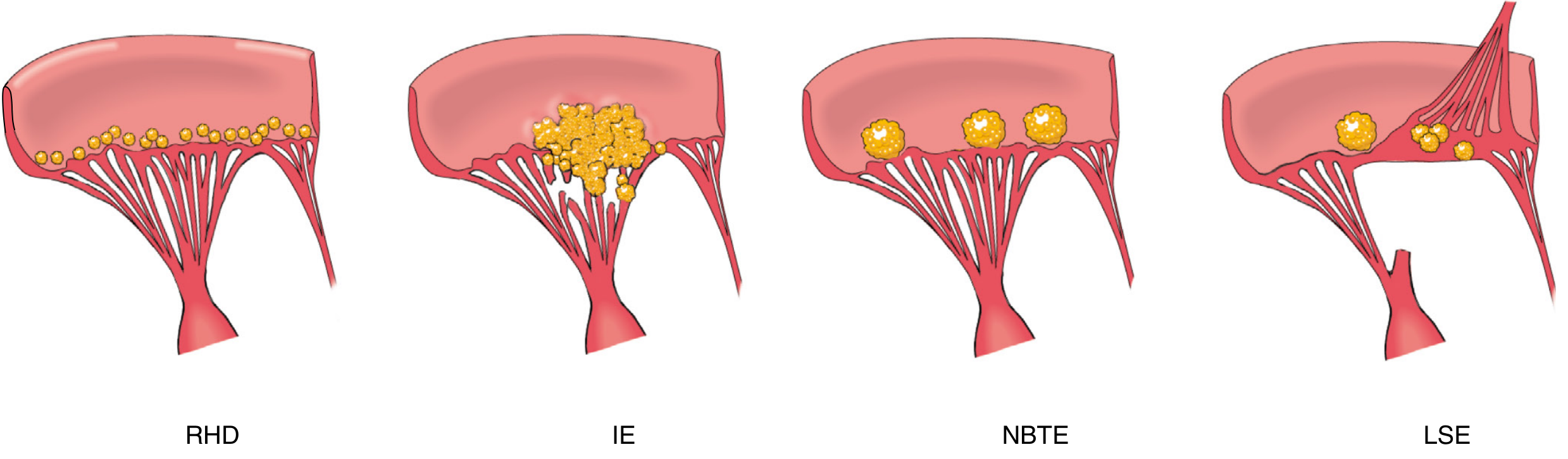
Comparison of vegetative endocarditis forms:
Microscopic:
- Subacute IE: granulation tissue at the vegetation base (healing), fibrosis, calcification over time
- Acute IE: minimal healing, predominant acute inflammatory infiltrate, extensive destruction
Clinical Features
Symptoms:
- Fever (most consistent sign - present in >90%; may be low-grade or absent in elderly)
- Chills, night sweats, malaise, anorexia, weight loss ("flu-like")
- Myalgia, arthralgia
- Back pain
Signs:
- New or changing cardiac murmur (majority of left-sided IE)
- Peripheral stigmata (immune complex and embolic phenomena):
- Osler nodes - tender nodules on fingertips/toes (immune complex mediated)
- Janeway lesions - non-tender hemorrhagic/erythematous macules on palms/soles (septic emboli - more common in acute IE)
- Roth spots - oval retinal hemorrhages with white centers
- Splinter hemorrhages - linear hemorrhages under nails
- Conjunctival petechiae
- Splenomegaly
- Clubbing (in subacute IE)
Complications:
| Complication | Frequency | Mechanism |
|---|---|---|
| Heart failure | 32.3% | Severe valve regurgitation (most common cause of death) |
| Embolic stroke | 16.9% | Vegetation fragment embolism |
| Other embolization | 22.6% | Septic emboli to spleen, kidney, brain, coronary arteries |
| Intracardiac abscess | 14.4% | Perivalvular extension - may cause heart block |
| Mycotic aneurysm | Infected emboli in vessel walls | |
| Glomerulonephritis | Immune complex deposition | |
| Septic pulmonary emboli | Common in IVDU | Right-sided vegetations |
Diagnosis: Modified Duke Criteria
MAJOR Criteria:
-
Blood culture positive for IE:
- Typical organisms (S. viridans, S. bovis, HACEK, S. aureus, community-acquired enterococci) from ≥2 separate blood cultures, OR
- Persistently positive blood cultures (≥2 cultures drawn >12h apart; or ≥3 of 4 if drawn ≥1h apart)
- Single positive culture for Coxiella burnetii or anti-phase 1 IgG antibody titer >1:800
-
Evidence of endocardial infection:
- Echocardiography positive for IE (vegetation, abscess, new prosthetic valve dehiscence), OR
- New valvular regurgitation (worsening or changing of existing murmur not sufficient)
MINOR Criteria:
- Predisposing heart condition or IV drug use
- Fever ≥38°C (100.4°F)
- Vascular phenomena: arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial/conjunctival hemorrhage, Janeway lesions
- Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
- Microbiologic evidence - positive blood culture but not meeting major criteria
Classification:
| Category | Criteria |
|---|---|
| Definite IE | 2 major, OR 1 major + 3 minor, OR 5 minor (clinical); or pathologic criteria |
| Possible IE | 1 major + 1 minor, OR 3 minor |
| Rejected | Firm alternative diagnosis, OR resolution with ≤4 days of antibiotics, OR no pathologic evidence after ≤4 days antibiotics |
2023 Duke/ISCVID Update: Added FDG-PET/CT as an imaging major criterion (abnormal metabolic activity within 3 months of prosthetic valve implantation), expanded molecular diagnostics (PCR, sequencing), and refined minor criteria to include more specific immune and vascular phenomena. - Textbook of Clinical Echocardiography
Echocardiography
TTE (Transthoracic Echo):
- First-line study; sensitivity 50-90% for native valve vegetations (95% specificity); ~50% for prosthetic valves
- Sensitivity for abscess: 30-50% native, only 15-35% prosthetic
- Should be performed as soon as possible in suspected IE
TEE (Transesophageal Echo):
- Superior resolution; sensitivity ~90% for vegetation, ~87% for abscess
- Indications for TEE (after TTE):
- TTE technically inadequate or non-diagnostic despite high clinical suspicion
- Prosthetic valve involvement
- S. aureus bacteremia
- Suspected perivalvular extension/abscess
- Suspicion of prosthetic valve IE
Repeat echo is recommended for high-risk patients (virulent organism, new murmur, persistent fever/bacteremia, clinical deterioration).
Other imaging (2023 criteria): ¹⁸F-FDG PET/CT, CT angiography, cardiac MRI - especially valuable in prosthetic valve IE where TTE/TEE sensitivity is limited.
Treatment
Antibiotic Regimens
| Organism | Regimen | Duration |
|---|---|---|
| VGS/S. gallolyticus (MIC <0.12) | Penicillin G (12-18 MU IV/day) or ceftriaxone 2g IV/day ± gentamicin (first 2 wk) | 4 weeks (6 wk for PVE or major emboli) |
| VGS (MIC 0.12-0.5) | Penicillin G + gentamicin, or ceftriaxone + gentamicin | 4 weeks |
| Enterococcus (PCN-susceptible) | Ampicillin 2g IV q4h + gentamicin 3mg/kg/day or ampicillin + ceftriaxone 2g IV q12h | 4-6 weeks |
| Enterococcus (PCN-resistant) | Vancomycin + gentamicin | 6 weeks |
| VRE | Linezolid 600mg IV/PO q12h or daptomycin ≥10-12 mg/kg/day | ≥6 weeks |
| S. aureus NVE (MSSA) | Oxacillin or nafcillin 2g IV q4h (cefazolin if mild PCN allergy) | 6 weeks (≥2 wk for uncomplicated right-sided IVDU IE) |
| S. aureus NVE (MRSA) | Vancomycin 15 mg/kg IV q12h or daptomycin ≥8 mg/kg/day | 6 weeks |
| S. aureus PVE (MSSA) | Oxacillin + rifampin 300mg PO q8h + gentamicin (first 2 wk) | ≥6 weeks |
| S. aureus PVE (MRSA) | Vancomycin + rifampin + gentamicin (first 2 wk) | ≥6 weeks |
| HACEK | Ceftriaxone 2g IV/day (alt: ampicillin or ciprofloxacin) | 4 wk NVE; 6 wk PVE |
| Culture-negative IE | Infectious diseases consultation required | Variable |
Empiric therapy (before culture results): Vancomycin 15 mg/kg IV q12h covers MRSA; switch to oxacillin/nafcillin if MSSA confirmed (penicillins are superior to vancomycin for MSSA).
Monitoring: Aminoglycoside levels, vancomycin trough 15-20 mcg/mL, weekly audiometry if aminoglycosides >7 days, CK monitoring on daptomycin.
- The Washington Manual of Medical Therapeutics
Surgical Indications (Native Valve IE)
Surgery is required in up to ~48% of IE cases. Indications include:
- Heart failure (most common) - severe valvular regurgitation or obstruction causing acute decompensation
- Perivalvular extension - abscess, fistula, new heart block
- Uncontrolled infection - persistent bacteremia/fever >5-7 days despite appropriate antibiotics; organisms resistant to antibiotics (fungi, Brucella)
- Prevention of embolism - large vegetation (>10 mm), especially with prior embolic event; rapidly increasing vegetation size
- S. aureus infection (high-risk feature)
- Prosthetic valve IE with any of the above, plus valve dehiscence
Prosthetic valve IE - surgery also indicated for: valve dehiscence, intracardiac fistula, relapsing PVE, severe prosthetic dysfunction causing heart failure.
Prophylaxis (AHA 2021 Update)
High-risk cardiac conditions warranting prophylaxis for invasive dental procedures:
- Prosthetic cardiac valve or material (including TAVR)
- Previous IE
- Unrepaired cyanotic CHD or repaired CHD with prosthetic material (first 6 months post-procedure)
- Cardiac valvulopathy in transplant recipients
- Ventricular assist devices and implantable hearts (added in 2021)
Regimens (dental/oral/respiratory procedures):
- Standard: Amoxicillin 2g PO, 1 hour before procedure
- Unable to take PO: Ampicillin 2g IM/IV or cefazolin/ceftriaxone 1g IM/IV within 30 min before
- Penicillin-allergic: Cephalexin 2g PO, or clarithromycin/azithromycin 500mg PO (clindamycin removed in 2021 update due to C. difficile risk); doxycycline added as an alternative
- GI/GU procedures: Routine prophylaxis not recommended
Note: The 2021 AHA update also emphasized shared decision-making, allergy screening (90% of "penicillin-allergic" patients test negative on skin testing and can receive amoxicillin), and maintenance of good oral health.
Summary: IE Management Team Approach
Every patient with IE should be managed in a hospital with expertise in IE, including:
- Infectious diseases
- Cardiovascular medicine
- Cardiovascular surgery
This "endocarditis team" approach has been shown to improve outcomes and is endorsed by both AHA and ESC guidelines.
Key Sources:
- Braunwald's Heart Disease, 11th Edition - Epidemiology, pathogenesis, team management
- Fuster and Hurst's The Heart, 15th Edition - Duke criteria, echo, PVE, surgery
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Pathology and morphology
- Robbins & Kumar Basic Pathology - Classification and pathogenesis
- The Washington Manual of Medical Therapeutics - Antibiotic regimens, prophylaxis
- Textbook of Clinical Echocardiography - 2023 Duke/ISCVID criteria

1001560354.jpg
True or false
Here are the answers:
a) The stomach has the greatest number of bacteria in the GI tract. → FALSE
The stomach has the fewest bacteria due to its acidic environment (pH ~2). The large intestine (colon) has the greatest number — up to 10¹¹–10¹² organisms per mL.
b) E. coli is the most abundant organism in the colon. → FALSE
E. coli is present in the colon but is a minor constituent. The most abundant organisms are obligate anaerobes, particularly Bacteroides, Bifidobacterium, and Faecalibacterium species, which outnumber E. coli by roughly 100–1000 fold.
c) Use of broad-spectrum antibiotics can lead to overgrowth of Clostridioides difficile. → TRUE
Broad-spectrum antibiotics (especially clindamycin, fluoroquinolones, cephalosporins, and ampicillin) disrupt the normal colonic flora, eliminating competitive organisms and allowing C. difficile to proliferate and produce toxins, causing pseudomembranous colitis.
d) Gut microbiome is acquired primarily at birth. → FALSE
The gut microbiome begins to be acquired at birth (especially during vaginal delivery and breastfeeding), but it is more accurate to say it is established through early life — the statement oversimplifies. More precisely, the microbiome is shaped by the mode of delivery, breastfeeding, diet, and environment over the first 2–3 years of life. The word "primarily at birth" makes this false as a standalone claim — colonization is a continuous process.
e) Staphylococcus epidermidis is a major component of the skin microbiome. → TRUE
S. epidermidis is a coagulase-negative staphylococcus and one of the most abundant and consistently found organisms on human skin. It colonizes sebaceous and moist areas and plays a role in skin defense by competing with pathogens like S. aureus.
Summary Table:
| Statement | Answer | |
|---|---|---|
| a | Stomach has greatest bacteria in GI tract | FALSE |
| b | E. coli is most abundant in colon | FALSE |
| c | Broad-spectrum antibiotics → C. difficile overgrowth | TRUE |
| d | Gut microbiome acquired primarily at birth | FALSE |
| e | S. epidermidis is major skin microbiome component | TRUE |
Can syphilis be infectious during secondary stage?
Reading File
Finding Sources
Reading File
Reading File
Yes — absolutely. Secondary syphilis is highly infectious.
Here is the full picture:
Infectiousness Across Syphilis Stages
| Stage | Infectious? | Why |
|---|---|---|
| Primary | Yes | Chancre teems with Treponema pallidum |
| Secondary | Yes - most infectious stage | Widespread mucocutaneous lesions, high spirochete burden |
| Early latent (<1 year) | Possibly (can relapse to secondary) | May revert to secondary stage |
| Late latent (>1 year) | No | Spirochetes far fewer, no active lesions |
| Tertiary | No | Spirochetes very difficult to demonstrate |
Why Secondary Syphilis Is So Infectious
Secondary syphilis develops 4-8 weeks after the primary chancre heals, representing systemic hematogenous dissemination of T. pallidum. According to Robbins & Kumar:
"The manifestations of secondary syphilis include mucocutaneous lesions, which are highly infectious, and generalized lymphadenopathy."
The specific infectious lesions in secondary syphilis are:
- Condyloma lata - broad, flat, moist papules in warm/moist areas (perineum, perianal region, axillae) - extremely rich in treponemes
- Mucous patches - painless, silvery-gray erosions on oral/genital mucosa - highly infectious
- The widespread maculopapular rash (including palms and soles) - not typically infectious because keratinized skin contains insufficient treponemes
"With the exception of mucous patches and condyloma lata, cutaneous manifestations of secondary syphilis do not contain a substantial number of treponemes and, therefore, are not typically infectious." - Fitzpatrick's Dermatology
Transmission Route in Secondary Syphilis
- Almost exclusively sexual contact with infectious lesions (condyloma lata, mucous patches)
- Lesions can be on genital, anal, or oral mucosa
- Direct skin-to-skin contact with an infectious lesion is sufficient for transmission
- Congenital transmission is also most likely during primary and secondary stages when spirochete burden is highest
Important Clinical Points
- Early latent syphilis (within the first year) can relapse back into secondary syphilis, making the patient infectious again - this is why early latent syphilis is treated with the same urgency
- Serologic tests are most sensitive in secondary syphilis - RPR/VDRL sensitivity is 100% in this stage (vs. 78-86% in primary)
- Patients in primary or secondary syphilis who are diagnosed should have all sexual contacts from the past 90 days traced and treated
Bottom line: Secondary syphilis is not just infectious - it is the peak infectious stage of the disease, primarily through condyloma lata and mucous patches.
- Robbins & Kumar Basic Pathology, p. 669
- Fitzpatrick's Dermatology, Chapter 170
Risk of transmission of HSV to the baby is low if it is recurrent genital herpes in a pregnant mother Tru or false?
Finding Sources
Reading File
Reading File
✅ TRUE
The risk of neonatal HSV transmission is significantly lower with recurrent genital herpes compared to primary infection.
The Numbers
| Type of Maternal Infection at Delivery | Risk of Neonatal Transmission |
|---|---|
| Primary (first episode) HSV near delivery | 25% - 60% |
| Nonprimary first episode (first clinical episode but antibodies present) | Intermediate |
| Recurrent genital HSV (symptomatic) | 1% - 5% |
| Recurrent HSV (asymptomatic/subclinical shedding) | Very low (~0 in some series) |
Why Recurrent Infection Carries Lower Risk
There are three key reasons:
-
Pre-formed maternal antibodies (IgG) - In recurrent infection, the mother has type-specific anti-HSV antibodies that cross the placenta and provide the neonate with passive protection
-
Lower viral shedding - Recurrent episodes involve far less virus at the genital tract compared to primary infection, reducing the inoculum the baby is exposed to during passage through the birth canal
-
Shorter duration of shedding - Recurrent episodes shed virus for fewer days than primary infection
"The risk of transmission to a neonate born to a mother who acquires primary genital HSV infection near the time of delivery is estimated to be 25% to 60%. The risk is considerably lower (1% to 2%) among women with recurrent, clinically evident infection."
- Creasy & Resnik's Maternal-Fetal Medicine
"The risk of infection for an infant delivered vaginally when the mother has active recurrent genital herpes infection is 2%-5%, whereas it is 26%-56% if the maternal infection at delivery is a first episode."
- Andrews' Diseases of the Skin
Important Nuances
- 70% of neonatal HSV cases occur in mothers with no known history of genital herpes - meaning subclinical/asymptomatic shedding is the biggest source of neonatal HSV, not symptomatic recurrences
- Recurrent HSV during pregnancy does not increase the risk of abortion or low-birth-weight infants
- Scalp electrodes during delivery can increase neonatal HSV risk up to 7-fold - should be avoided if HSV shedding is possible
- Vacuum-assisted delivery increases relative risk 2-27 times
- Despite the lower risk, recurrent herpes with active lesions at delivery is still an indication for caesarean section
Management of Recurrent HSV in Pregnancy
-
Suppressive acyclovir/valacyclovir from 36 weeks reduces recurrence at delivery and likelihood of caesarean section
-
Routine prenatal cultures are not recommended for recurrent HSV (they don't predict shedding at delivery)
-
Caesarean section is indicated if active genital lesions or prodromal symptoms are present at the time of labor
-
Creasy & Resnik's Maternal-Fetal Medicine
-
Andrews' Diseases of the Skin
Specific serological tests cannot be used to determine the response to treatment True or false?
Finding Sources
✅ TRUE
Specific (treponemal) serological tests cannot be used to monitor treatment response in syphilis.
Understanding the Two Types of Syphilis Tests
| Feature | Non-treponemal (Non-specific) | Treponemal (Specific) |
|---|---|---|
| Examples | RPR, VDRL | FTA-ABS, TPPA, MHA-TP, EIA, CIA |
| What they detect | Antibodies to cardiolipin-lecithin-cholesterol (reagin) | Antibodies directly against T. pallidum |
| Quantitative? | Yes - reported as titers (e.g., 1:32) | No - qualitative (positive/negative) |
| Monitor treatment? | YES | NO |
| Revert after cure? | Yes - titers fall and can become negative | No - remain positive for life |
Why Treponemal Tests Cannot Monitor Treatment
"Treponemal tests remain positive in 95% of patients, even after treatment, and are not used to monitor treatment response and cannot distinguish active from treated syphilis."
- Textbook of Family Medicine
"These treponemal tests are highly specific for syphilis, but they may remain positive for life even after successful treatment and cure."
- Rosen's Emergency Medicine
Once positive, treponemal tests stay positive permanently (the "serofast" state) - they indicate past exposure, not active disease or treatment failure.
What IS Used to Monitor Treatment
Non-treponemal tests (RPR/VDRL) with serial quantitative titers are the correct tool:
"After treatment for early syphilis, a persistent fall by fourfold or more (e.g., a decline from 1:32 to 1:8) is considered an adequate response."
- Harrison's Principles of Internal Medicine, 22nd Edition
Treatment response criteria:
- Adequate response: ≥4-fold (2-dilution) decrease in RPR/VDRL titer within 6-12 months
- Treatment failure / reinfection: <4-fold decrease, or 4-fold increase in titer
- RPR/VDRL sensitivity is 100% in secondary syphilis - the stage with highest titers
Summary
| Test Type | Use for Diagnosis? | Use for Treatment Monitoring? |
|---|---|---|
| Treponemal (FTA-ABS, TPPA) | ✅ Yes - confirms positive screen | ❌ No - stays positive for life |
| Non-treponemal (RPR, VDRL) | ✅ Yes - screening | ✅ Yes - serial titers track response |
The statement is TRUE - specific (treponemal) serological tests cannot be used to determine response to treatment. Only non-specific (non-treponemal) quantitative tests like RPR and VDRL serve this purpose.
- Textbook of Family Medicine, 9th Edition
- Harrison's Principles of Internal Medicine, 22nd Edition
- Rosen's Emergency Medicine
Fever settles down within 8-12 hours after the initiation of correct antibiotic True or false?
Finding Sources
Finding Sources
Reading File
❌ FALSE
This statement is false — and it refers to the Jarisch-Herxheimer (JH) reaction in syphilis treatment.
Rather than settling down in 8-12 hours, the correct antibiotic (penicillin) for syphilis actually causes fever to SPIKE within the first few hours after treatment begins.
The Jarisch-Herxheimer Reaction
When syphilis is treated with penicillin, patients commonly experience the JH reaction - an acute worsening of symptoms caused by the correct antibiotic:
"The Jarisch-Herxheimer reaction is a self-limited clinical syndrome consisting of fever, headache, flare of mucocutaneous lesions, tender lymphadenopathy, pharyngitis, malaise, myalgia, and leukocytosis. It occurs within the first 24 hours after initiating therapy. The fever peaks 6 to 8 hours after the onset, usually around 39°C (102.2°F), but it can be as high as 42°C (107.6°F)."
- Fitzpatrick's Dermatology
Timeline of the JH Reaction
| Time after antibiotic | What happens |
|---|---|
| Within 2-4 hours | Onset of fever, rigors, myalgia, headache |
| 6-8 hours | Fever peaks (~39°C, up to 42°C) |
| 8-12 hours | Fever is still present / defervescing |
| 24 hours | Reaction fully resolves |
So at 8-12 hours, the fever is actually at or just past its peak - it has not settled. The fever resolves by around 24 hours, not 8-12 hours.
Pathogenesis
The JH reaction is thought to result from cytokine release triggered by lipoproteins released from dying T. pallidum organisms as the antibiotic kills them. It is NOT an allergic reaction to penicillin - this distinction is clinically important.
Clinical Significance
- Patients must be warned before treatment that this reaction will occur
- It does not mean the antibiotic is wrong - it is actually a sign the treatment is working
- Management: rest, hydration, paracetamol (limited evidence)
- In pregnant women: JH reaction can cause premature labor or fetal distress - requires monitoring, but treatment must not be delayed given the risk of congenital syphilis
- If anaphylaxis occurs instead, this is a true penicillin allergy requiring drug change
Correction of the Statement
The statement as written is FALSE on two counts:
- Fever does not settle in 8-12 hours - it peaks at 6-8 hours
- Fever resolves by ~24 hours, not 8-12 hours
- Fitzpatrick's Dermatology, Chapter 170
- Creasy & Resnik's Maternal-Fetal Medicine
- Tintinalli's Emergency Medicine
Typhoid Fever settles down within 8-12 hours after the initiation of correct antibiotic True or false?
Finding Sources
Reading File
Finding Sources
Reading File
❌ FALSE
Fever in typhoid takes days to settle after starting correct antibiotics - nowhere near 8-12 hours.
What the Evidence Says
From Harrison's Principles of Internal Medicine (22nd Ed.), the defervescence timeline with correct antibiotics is:
| Antibiotic | Time to Fever Resolution |
|---|---|
| Azithromycin | 4-6 days |
| Ceftriaxone / Cefotaxime / Cefixime | ~1 week (~7 days) |
| Fluoroquinolones (susceptible strains) | ~5-7 days |
| Chloramphenicol / Ampicillin (older agents) | 3-5 days |
"Oral azithromycin results in defervescence in 4–6 days... Ceftriaxone and cefixime clear fever in ~1 week."
- Harrison's Principles of Internal Medicine, 22nd Edition
Why Fever Takes So Long to Settle in Typhoid
Typhoid is caused by Salmonella enterica serotype Typhi - an intracellular pathogen that:
- Survives and replicates inside macrophages
- Causes a sustained, step-ladder pattern fever that persists for weeks if untreated
- Even with the correct antibiotic, the intracellular location means it takes days for the drug to clear the organism and for the host's inflammatory response to subside
Untreated typhoid fever can persist for up to 4 weeks.
Treatment Duration Note
"Therapy should be administered for at least 10 days or for 5 days after fever resolution."
- Harrison's Principles of Internal Medicine, 22nd Edition
This further confirms fever resolution is an event that occurs days into treatment, not hours - and antibiotics must be continued for 5 more days even after the fever finally settles.
Summary
| Claim | Reality |
|---|---|
| Fever settles in 8-12 hours | ❌ FALSE |
| Actual defervescence time | 4-7 days depending on antibiotic used |
| Untreated fever duration | Up to 4 weeks |
- Harrison's Principles of Internal Medicine, 22nd Edition - Chapter on Enteric Fever
This is a shared conversation. Sign in to Orris to start your own chat.