Kreb cycle
Reading File
Finding Sources
Searching the Web
Krebs cycle steps enzymes NADH FADH2 overview biochemistry
Reading File
Loading Image
Reading File
Here is a thorough breakdown of the Krebs cycle based on Guyton & Hall's Textbook of Medical Physiology.
The Krebs Cycle (Citric Acid Cycle / TCA Cycle)
Named after Hans Krebs who discovered it, the citric acid cycle is also called the tricarboxylic acid (TCA) cycle. It is the second major stage of aerobic cellular respiration, occurring in the mitochondrial matrix.
Entry Point: Acetyl-CoA
Before the cycle begins, pyruvate (from glycolysis) is converted to acetyl-CoA in the mitochondria by pyruvate dehydrogenase. This step releases one CO2 and one NADH per pyruvate. Since glucose yields two pyruvates, two acetyl-CoA molecules enter the cycle per glucose.
The 8 Steps of the Krebs Cycle
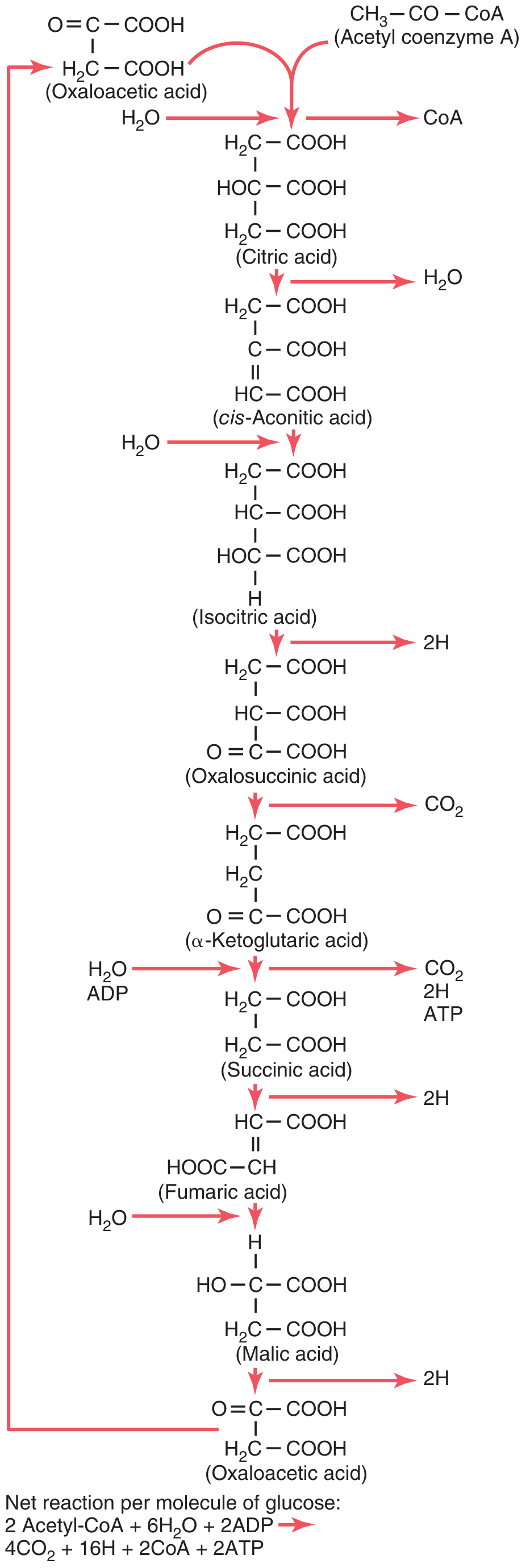
Figure 68.6 from Guyton & Hall - Chemical reactions of the citric acid cycle
| Step | Reaction | Enzyme | Products |
|---|---|---|---|
| 1 | Oxaloacetate + Acetyl-CoA → Citrate | Citrate synthase | CoA released |
| 2 | Citrate → cis-Aconitate → Isocitrate | Aconitase | H2O removed, then added |
| 3 | Isocitrate → Oxalosuccinate → α-Ketoglutarate | Isocitrate dehydrogenase | 2H (→ NADH), CO2 |
| 4 | α-Ketoglutarate → Succinyl-CoA | α-Ketoglutarate dehydrogenase | 2H (→ NADH), CO2 |
| 5 | Succinyl-CoA → Succinate | Succinyl-CoA synthase | GTP (= ATP) |
| 6 | Succinate → Fumarate | Succinate dehydrogenase | 2H (→ FADH2) |
| 7 | Fumarate → Malate | Fumarase | H2O added |
| 8 | Malate → Oxaloacetate | Malate dehydrogenase | 2H (→ NADH) |
Oxaloacetate is regenerated at step 8, allowing the cycle to continue.
Net Products Per Acetyl-CoA (one turn)
| Product | Amount | Fate |
|---|---|---|
| CO2 | 2 molecules | Expired via lungs |
| NADH | 3 molecules | Oxidative phosphorylation → ~7.5 ATP |
| FADH2 | 1 molecule | Oxidative phosphorylation → ~1.5 ATP |
| GTP/ATP | 1 molecule | Direct energy |
Per glucose molecule (2 turns of the cycle):
- 4 CO2
- 6 NADH
- 2 FADH2
- 2 ATP (from GTP)
- Total from Krebs alone: ~2 ATP directly; NADH/FADH2 then yield ~20 more ATP via oxidative phosphorylation
Key Regulatory Enzymes
Three enzymes act as major control points, all inhibited by high-energy states:
- Citrate synthase - inhibited by ATP, NADH, succinyl-CoA, citrate
- Isocitrate dehydrogenase - inhibited by ATP/NADH; activated by ADP/Ca2+
- α-Ketoglutarate dehydrogenase - inhibited by succinyl-CoA, NADH; activated by Ca2+
Role of Dehydrogenases and NAD+
As stated in Guyton & Hall: "Twenty of the 24 hydrogen atoms [released per glucose] immediately combine with nicotinamide adenine dinucleotide (NAD+), a derivative of the vitamin niacin."
The remaining 4 hydrogen atoms (released between succinate → fumarate) combine with FAD instead, forming FADH2. All these carriers then feed into the electron transport chain for the bulk of ATP production via oxidative phosphorylation.
Amphibolic Nature (Both Anabolic and Catabolic)
The Krebs cycle is not purely catabolic. Its intermediates serve as precursors for biosynthesis:
- α-Ketoglutarate → glutamate and other amino acids
- Succinyl-CoA → heme (porphyrin) synthesis
- Oxaloacetate → aspartate, gluconeogenesis
- Citrate → exported to cytoplasm for fatty acid synthesis
Overall Energy Yield from One Glucose Molecule
| Stage | ATP yield |
|---|---|
| Glycolysis | 2 ATP (net) |
| Pyruvate → Acetyl-CoA | ~5 ATP (via 2 NADH) |
| Krebs cycle (2 turns) | ~20 ATP (via NADH, FADH2) + 2 GTP |
| Total | ~30-32 ATP |
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 68 (Metabolism and Temperature Regulation), p. 836.
Create a visual study guide/poster on the 8 Krebs cycle enzymes
Generating Image
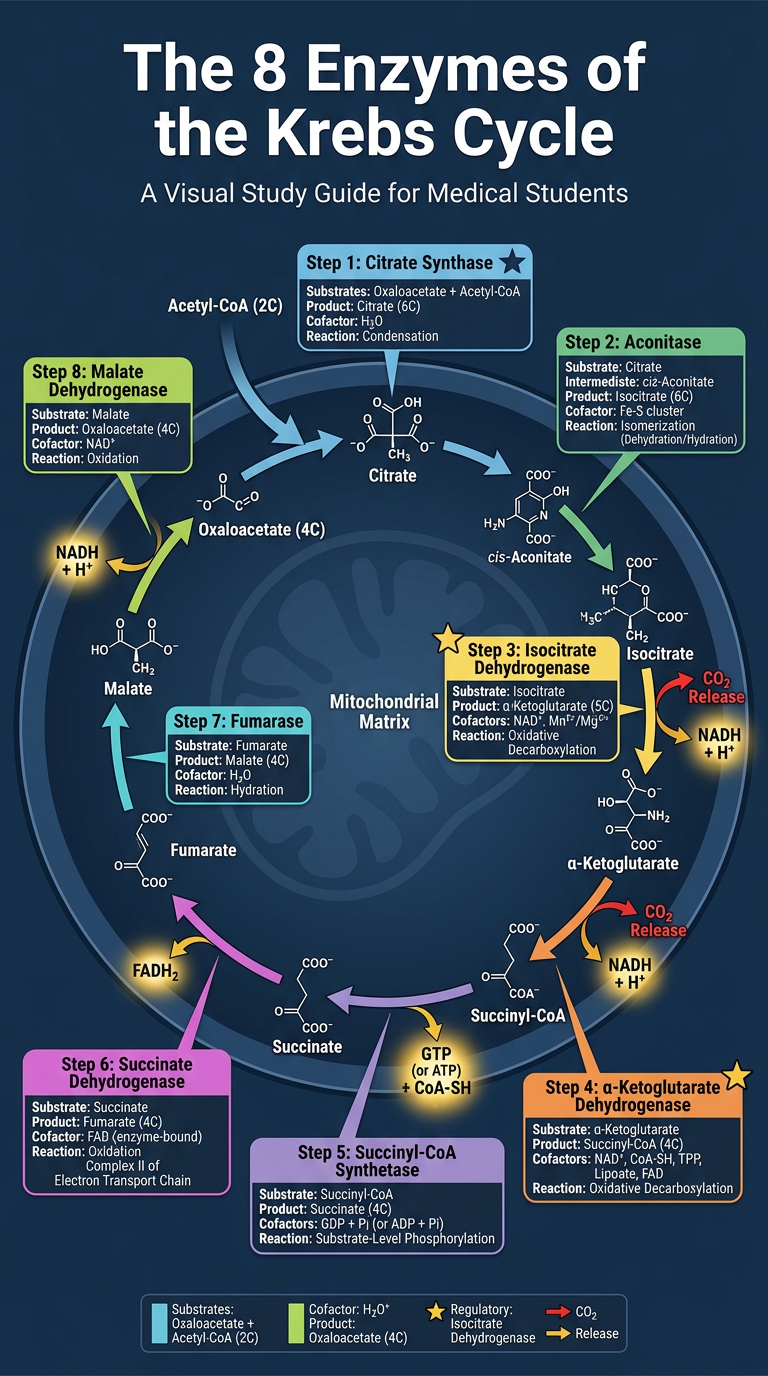
Here's a quick reference summary to go along with the poster:
| # | Enzyme | Substrate → Product | Cofactor/Product | Notes |
|---|---|---|---|---|
| 1 | Citrate Synthase | Oxaloacetate + Acetyl-CoA → Citrate | CoA released | ⭐ Regulatory; inhibited by ATP, NADH, citrate |
| 2 | Aconitase | Citrate → Isocitrate | - | Goes via cis-Aconitate intermediate |
| 3 | Isocitrate Dehydrogenase | Isocitrate → α-Ketoglutarate | NADH, CO2 | ⭐ Regulatory; activated by ADP/Ca2+ |
| 4 | α-Ketoglutarate Dehydrogenase | α-Ketoglutarate → Succinyl-CoA | NADH, CO2 | ⭐ Regulatory; requires B vitamins (thiamine, lipoate) |
| 5 | Succinyl-CoA Synthetase | Succinyl-CoA → Succinate | GTP | Only step producing direct ATP equivalent |
| 6 | Succinate Dehydrogenase | Succinate → Fumarate | FADH2 | Embedded in inner mitochondrial membrane; also Complex II of ETC |
| 7 | Fumarase | Fumarate → Malate | H2O added | Simple hydration reaction |
| 8 | Malate Dehydrogenase | Malate → Oxaloacetate | NADH | Regenerates oxaloacetate to restart the cycle |
Memory tip for the 8 enzymes in order:
Citrus Are In A Sunny South Florida Most days (Citrate synthase - Aconitase - Isocitrate DH - Alpha-KG DH - Succinyl-CoA synthetase - Succinate DH - Fumarase - Malate DH)
Regulation of blood ph biochemistry
Finding Sources
Finding Sources
Searching the Web
regulation of blood pH biochemistry buffer systems bicarbonate respiratory renal
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough biochemistry overview of blood pH regulation, drawn from Basic Medical Biochemistry (6e), Lippincott's Illustrated Biochemistry (8e), and Ganong's Review of Medical Physiology (26e).
Regulation of Blood pH
Normal Blood pH
| Parameter | Normal Value |
|---|---|
| Arterial blood pH | 7.36 - 7.44 (mean 7.40) |
| [H+] at pH 7.4 | ~40 nEq/L (4 × 10⁻⁸ mol/L) |
| Compatible range for life | 6.8 - 7.8 |
| Intracellular pH | ~7.1 (range 6.9 - 7.4) |
Metabolism produces roughly 22,000 mEq of acid per day. Without buffering, this would drop blood pH to < 1. Three lines of defense maintain pH within the narrow normal range.
Line 1: Chemical Buffer Systems (Immediate - seconds)
A buffer resists pH change when acid or base is added by converting strong acids/bases into weak ones. Maximum buffering occurs at a pH ± 1 unit of the pKa.
The Henderson-Hasselbalch Equation
$$\text{pH} = \text{pKa} + \log\frac{[\text{A}^-]}{[\text{HA}]}$$
For the bicarbonate system specifically:
$$\text{pH} = 6.1 + \log\frac{[\text{HCO}3^-]}{0.03 \times P{aCO_2}}$$
At normal values: pH = 6.1 + log(24 / 1.2) = 6.1 + log(20) = 6.1 + 1.3 = 7.4
A. Bicarbonate-Carbonic Acid Buffer System (ECF - most important)
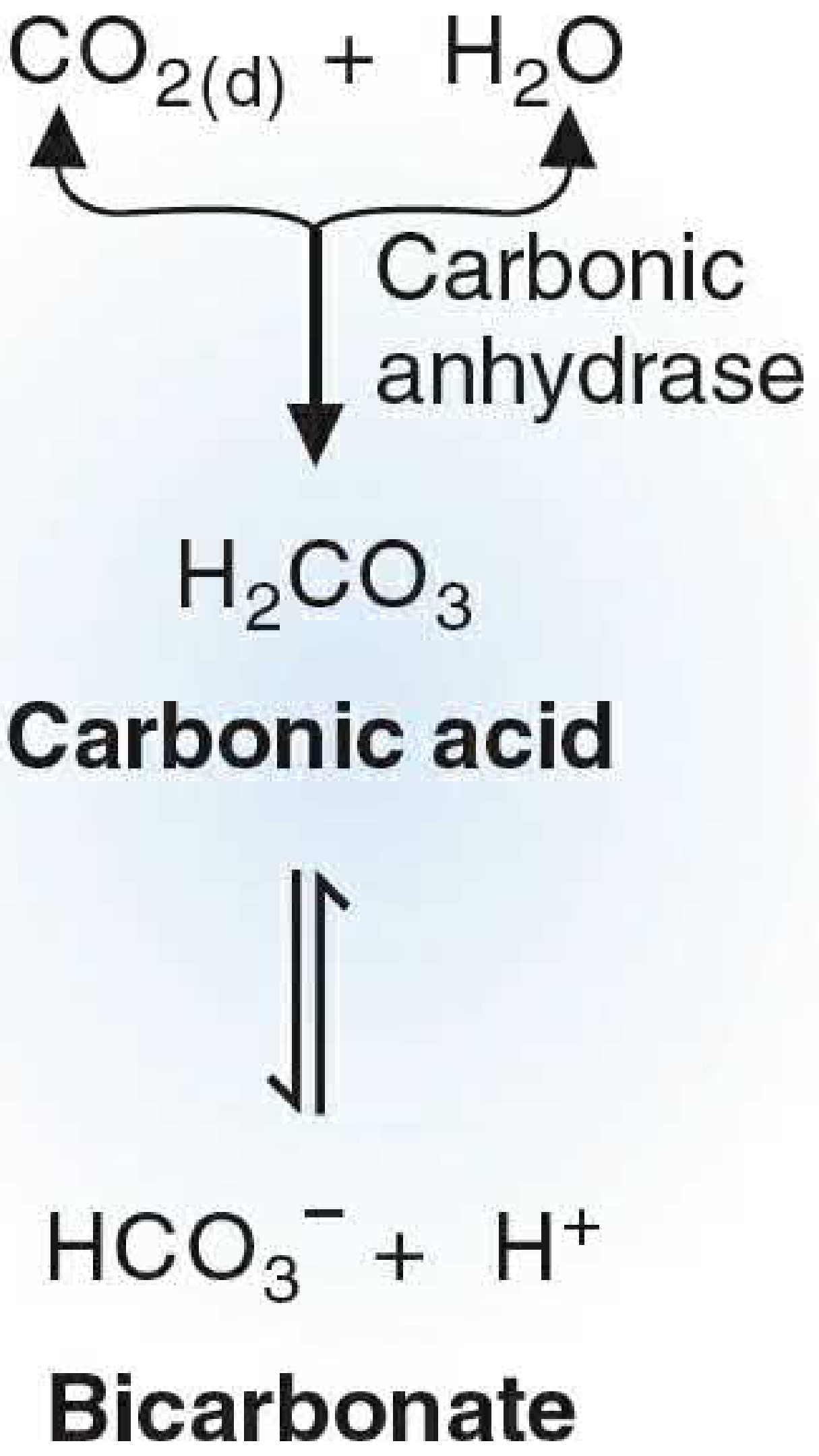
Figure 4.8, Basic Medical Biochemistry 6e - The bicarbonate buffer system
The central reaction:
CO₂ + H₂O ⇌ H₂CO₃ ⇌ HCO₃⁻ + H⁺
Catalyzed by carbonic anhydrase (CA). This system is uniquely powerful because:
- CO₂ is controlled by the lungs (volatile acid)
- HCO₃⁻ is controlled by the kidneys
- Both components can be independently regulated, giving far more flexibility than a simple chemical buffer
Although the pKa is 6.1 (not ideal for buffering at pH 7.4), the open system keeps the ratio [HCO₃⁻]/[CO₂] = 20:1 and maintains pH at 7.4.
B. Hemoglobin Buffer System (RBCs - very important)
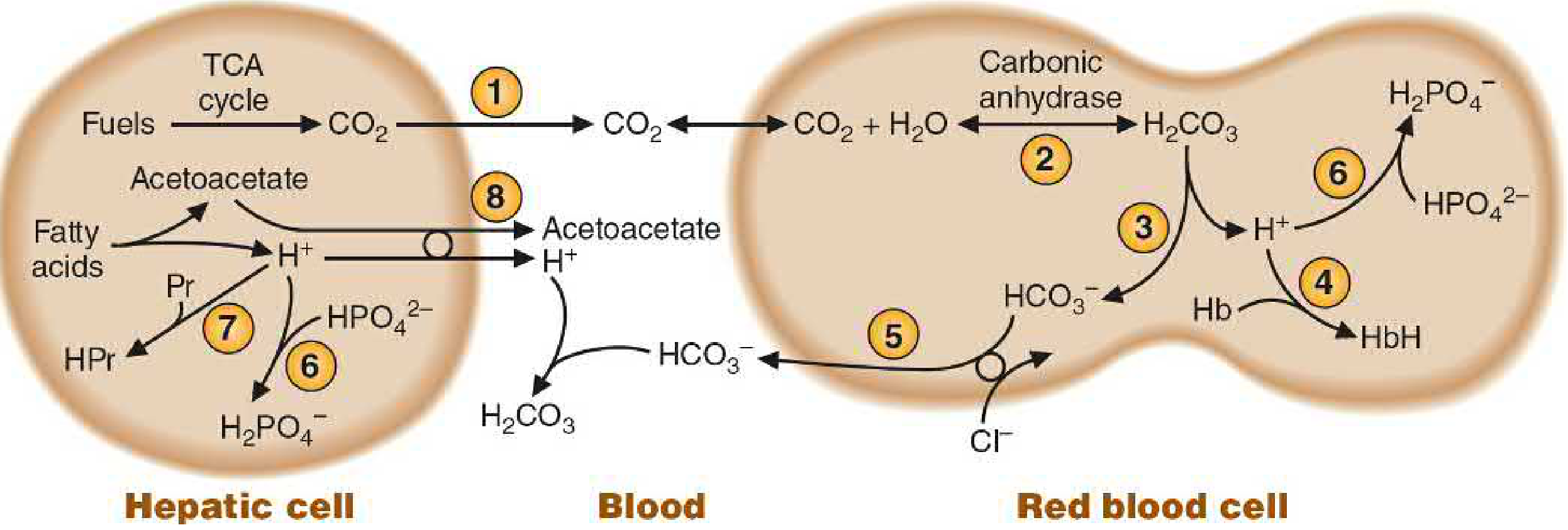
Figure 4.9, Basic Medical Biochemistry 6e - Integrated buffering systems of the body
- CO₂ from the TCA cycle diffuses into RBCs
- Carbonic anhydrase (high in RBCs) converts CO₂ → H₂CO₃ → HCO₃⁻ + H⁺
- H⁺ is buffered by histidine residues on hemoglobin (pKa 6.7) → forms HbH
- HCO₃⁻ is exported to plasma in exchange for Cl⁻ (chloride shift)
- In the lungs, the process reverses: HbH releases H⁺, HCO₃⁻ re-enters RBCs, CO₂ is exhaled
Deoxyhemoglobin is a better buffer than oxyhemoglobin (Bohr effect).
C. Phosphate Buffer System (ICF and Urine)
HPO₄²⁻ / H₂PO₄⁻ system, pKa = 6.8. More effective intracellularly and in urine than in blood (low phosphate concentration in plasma limits its role there).
D. Protein Buffer System
Plasma proteins and intracellular proteins buffer via ionizable amino acid side chains (especially histidine). Accounts for a large fraction of intracellular buffering.
Line 2: Respiratory Regulation (Minutes - hours)
The lungs regulate CO₂, which directly shifts the bicarbonate equilibrium:
- Acidosis (↓ pH): Peripheral chemoreceptors detect ↑ H⁺/CO₂ → stimulate respiratory center → hyperventilation → blows off CO₂ → pH rises
- Alkalosis (↑ pH): Respiratory center is depressed → hypoventilation → CO₂ retained → pH falls
This can correct pH changes 10-75× faster than renal compensation, but cannot fully compensate for metabolic disorders.
| Condition | Lungs respond by |
|---|---|
| Metabolic acidosis | Hyperventilation (↓ PaCO₂) |
| Metabolic alkalosis | Hypoventilation (↑ PaCO₂) |
Line 3: Renal Regulation (Hours - days, most powerful long-term)
The kidneys regulate pH by:
- Reabsorbing HCO₃⁻ (80% reabsorbed in proximal tubule)
- Secreting H⁺ into tubular lumen
- Excreting titratable acid (phosphate buffers) and ammonium (NH₄⁺)
Renal H⁺ Secretion Mechanisms
| Location | Transporter | Details |
|---|---|---|
| Proximal tubule | Na⁺-H⁺ exchanger (NHE3) | Secondary active; driven by Na⁺ gradient from Na/K ATPase |
| Distal tubule / Collecting duct | H⁺-ATPase (proton pump) | Primary active; Na⁺-independent; stimulated by aldosterone |
Inside tubular cells, carbonic anhydrase II forms H₂CO₃ from CO₂ + H₂O → dissociates to H⁺ (secreted into lumen) + HCO₃⁻ (enters blood). Net effect: for every H⁺ secreted, one HCO₃⁻ is added back to blood.
Summary: The Four Acid-Base Disorders
| Disorder | Primary Change | Compensation |
|---|---|---|
| Metabolic Acidosis | ↓ HCO₃⁻ | ↑ Ventilation (↓ PaCO₂) |
| Metabolic Alkalosis | ↑ HCO₃⁻ | ↓ Ventilation (↑ PaCO₂) |
| Respiratory Acidosis | ↑ PaCO₂ | Kidneys retain HCO₃⁻, excrete H⁺ |
| Respiratory Alkalosis | ↓ PaCO₂ | Kidneys excrete HCO₃⁻, retain H⁺ |
Quick Comparison of Buffer Systems
| Buffer System | Location | pKa | Regulated By |
|---|---|---|---|
| Bicarbonate/H₂CO₃ | ECF/blood | 6.1 | Lungs + Kidneys |
| Hemoglobin | RBCs | 6.7 | O₂/CO₂ exchange |
| Phosphate | ICF, urine | 6.8 | Kidneys |
| Proteins | ICF, plasma | ~6-7 | Metabolism |
Sources:
- Basic Medical Biochemistry: A Clinical Approach, 6e, Chapter 4, pp. 96-98
- Lippincott's Illustrated Biochemistry, 8e, Chapter 1, pp. 33-34
- Ganong's Review of Medical Physiology, 26e, Chapter 39, pp. 711-712
Generate a clinical practice guide on ABG interpretation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Running Command
Writing File
Running Command
Running Command
Your ABG Clinical Practice Guide is ready:
ABG Clinical Practice Guide
Presentation · PPTX
What's Inside (8 Slides)
| Slide | Content |
|---|---|
| 1 - Title | Cover slide with sources cited |
| 2 - Normal Values | Reference cards for pH, PaCO₂, HCO₃⁻, PaO₂, SaO₂, Base Excess + Henderson-Hasselbalch equation |
| 3 - 5-Step Method | Systematic step-by-step ABG interpretation framework |
| 4 - Compensation Formulas | All 6 formulas: Winter's, metabolic alkalosis, acute/chronic resp. acidosis/alkalosis |
| 5 - Anion Gap Analysis | AG formula + full MUDPILES vs HARDUPS mnemonics |
| 6 - Causes | All 4 disorders in a color-coded quad layout with key etiologies |
| 7 - Worked Cases | 3 clinical examples (DKA, COPD exacerbation, vomiting) with step-by-step analysis |
| 8 - Quick Reference | Master summary table + A-a gradient formula + Delta-Delta ratio + VBG vs ABG comparison |
Sources: Rosen's Emergency Medicine 10e, Frameworks for Internal Medicine, Ganong's Medical Physiology 26e, Basic Medical Biochemistry 6e, Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.