I have 0 Knowledge about ECG.Teach me from basic and give me disease with ECG changes with better explaination
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram normal waves P QRS T
Reading File
Reading File
Searching Images
ECG myocardial infarction ST elevation STEMI changes
Reading File
Searching Images
ECG atrial fibrillation flutter arrhythmia heart block
Searching Images
ECG bundle branch block left right LBBB RBBB
Searching Images
ECG hyperkalemia hypokalemia electrolyte changes peaked T wave
Searching Images
ECG cardiac conduction pathway SA node AV node diagram
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
📖 ECG (Electrocardiogram) — Complete Beginner's Guide
PART 1 — What Is an ECG?
An ECG (also written EKG, from the German Elektrokardiogramm) is a recording of the tiny electrical signals your heart produces with every beat, picked up by electrodes placed on your skin. These signals are displayed as a wavy line on paper or a screen.
Think of it this way: every time a heart muscle cell fires, it creates a small voltage. The ECG captures the sum of all those voltages at different angles around your body — giving you a complete "electrical portrait" of the heart.
PART 2 — The Cardiac Conduction System (The Heart's Electrical Wiring)
Before reading the ECG, you need to understand why the electricity happens.
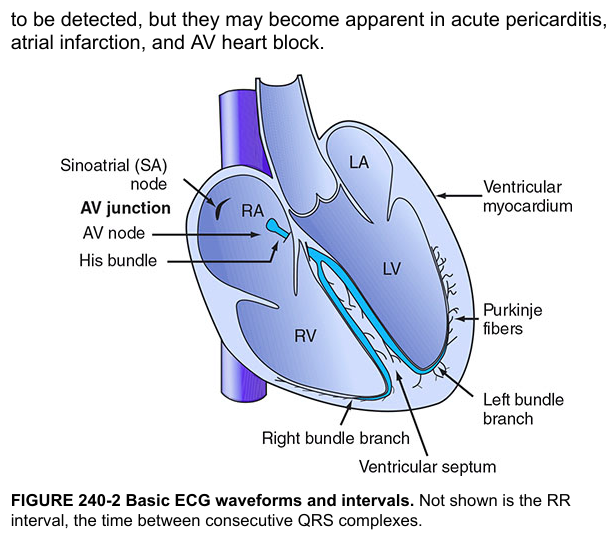
The electrical signal travels in this exact sequence:
SA Node → Atria → AV Node → Bundle of His → Left + Right Bundle Branches → Purkinje Fibers → Ventricular muscle
| Structure | Location | Role |
|---|---|---|
| SA Node (Sinoatrial) | Right atrium | The pacemaker — fires 60–100 times/min |
| Atrial muscle | Both atria | Conducts signal → atria contract |
| AV Node (Atrioventricular) | Between atria & ventricles | Delays signal ~120 ms so atria finish emptying |
| Bundle of His | Interventricular septum | Fast highway for the signal |
| Right & Left Bundle Branches | Septum | Split signal to each ventricle |
| Purkinje Fibers | Inner ventricular wall | Rapidly spread signal to all ventricular muscle |
Key concept: The AV node introduces a deliberate delay — this is what you see as the PR interval on the ECG. It lets atria push blood into ventricles before ventricles contract.
PART 3 — The ECG Paper & How to Read It
The Grid

ECG paper has a grid:
- Horizontal axis = TIME: Each small box = 0.04 sec; each large box (5 small boxes) = 0.2 sec
- Vertical axis = VOLTAGE: Each small box = 0.1 mV; 10 mm = 1 mV
The 12 Leads
A standard ECG records from 12 different "camera angles" around the heart:
| Group | Leads | What they look at |
|---|---|---|
| Limb leads | I, II, III | Frontal plane (left/right/inferior) |
| Augmented limb leads | aVR, aVL, aVF | More frontal views |
| Precordial (chest) leads | V1–V6 | Horizontal plane (front to back) |
Memory trick: Think of leads as security cameras placed around a building — each sees the same event from a different angle.
PART 4 — The ECG Waves: What Each One Means
Normal ECG Components
| Wave/Interval | What it represents | Normal duration |
|---|---|---|
| P wave | Atrial depolarization (atria contracting) | < 0.12 sec (< 3 small boxes) |
| PR interval | Conduction from SA node → start of ventricular firing (includes AV node delay) | 0.12–0.20 sec (3–5 small boxes) |
| QRS complex | Ventricular depolarization (ventricles contracting) | < 0.12 sec (< 3 small boxes) |
| ST segment | Isoelectric pause — all ventricular cells are depolarized (plateau of action potential) | Should be flat/isoelectric |
| T wave | Ventricular repolarization (ventricles resetting) | Upright in most leads |
| QT interval | QRS start → T wave end (entire ventricular electrical cycle) | < 0.44 sec (corrected) |
| U wave | Small wave after T wave (not always seen) — Purkinje repolarization | Tiny, same direction as T |
Understanding Q, R, S:
- Q wave = First downward deflection before the tall spike
- R wave = Tall upward spike (largest part of QRS)
- S wave = Downward deflection after the R wave
Pathological Q wave: A Q that is > 1 small box wide OR > 1/4 the height of the R wave = sign of old myocardial infarction (dead muscle)
PART 5 — How to Calculate Heart Rate
Method 1 (regular rhythm):
Rate = 300 ÷ number of large boxes between two R waves
- 1 large box between R waves → rate = 300 bpm
- 2 large boxes → 150 bpm
- 3 large boxes → 100 bpm
- 4 large boxes → 75 bpm ✓ (normal)
- 5 large boxes → 60 bpm ✓ (normal)
Normal heart rate: 60–100 bpm
PART 6 — Systematic Approach to Reading Any ECG
Always use this 7-step system:
- Rate — Fast, slow, or normal? (< 60 = bradycardia; > 100 = tachycardia)
- Rhythm — Regular or irregular? Is there a P before every QRS?
- P waves — Present? Upright in lead II? One P per QRS?
- PR interval — Normal (0.12–0.20 sec)?
- QRS width — Narrow (< 0.12 sec) or wide (≥ 0.12 sec)?
- ST segment — Elevated, depressed, or flat?
- T waves — Upright? Inverted? Peaked?
PART 7 — Diseases With ECG Changes
🔴 1. Myocardial Infarction (Heart Attack)
A blocked coronary artery kills heart muscle. The ECG evolves in stages:
Phase 1 — Hyperacute (minutes to 1 hour)
- Tall, peaked "hyperacute" T waves — earliest sign, often missed
Phase 2 — Acute (hours)
- ST elevation — the classic STEMI pattern (convex/"tombstone" shape)
- Reciprocal ST depression in opposite leads
Phase 3 — Hours to days
- T wave inversion develops
- Pathological Q waves appear (= dead muscle)
Phase 4 — Old/chronic
- Persistent Q waves (the permanent scar)
- ST returns to normal
Lead territories (which leads are affected tells you WHERE the heart attack is):
| Affected Leads | Territory | Artery Blocked |
|---|---|---|
| V1–V4 | Anterior wall | LAD (Left Anterior Descending) |
| II, III, aVF | Inferior wall | RCA (Right Coronary Artery) |
| I, aVL, V5–V6 | Lateral wall | LCx (Left Circumflex) |
| V1–V2 tall R wave + ST depression | Posterior wall | RCA or LCx |
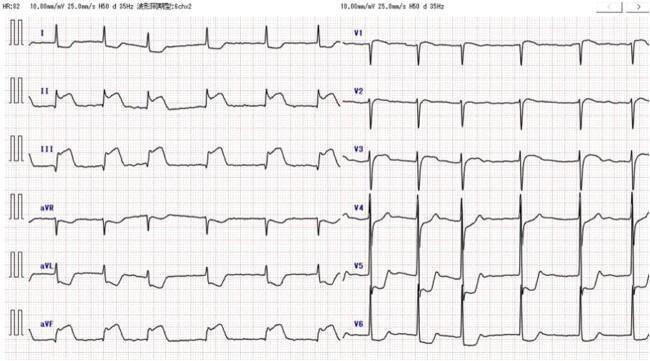
Anterior STEMI ECG:

ST elevation in V1–V6 with convex ("tombstoning") morphology, reciprocal ST depression in inferior leads II, III, aVF — classic proximal LAD occlusion
Inferior STEMI ECG:
ST elevation in II, III, aVF; reciprocal depression in I and aVL — right coronary artery territory
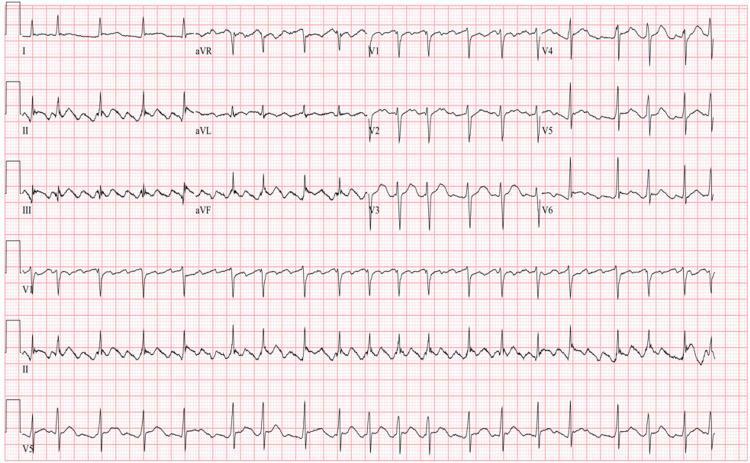
🟠 2. Atrial Fibrillation (AF)
AF is the most common arrhythmia. The atria fire chaotically (350–600 impulses/min), only some of which get through the AV node.
ECG Features:
- ❌ No P waves — replaced by irregular "fibrillatory" baseline
- Irregularly irregular RR intervals (hallmark sign — no two spaces between beats are equal)
- Narrow QRS (unless bundle branch block also present)
- Rate usually 100–160 bpm (uncontrolled)
🟠 3. Atrial Flutter
The atria fire in a regular loop at ~300 bpm, with the AV node blocking some beats.
ECG Features:
- "Sawtooth" flutter waves at ~300 bpm — most visible in leads II, III, aVF
- Regular ventricular response at 150 bpm (2:1 block), 100 bpm (3:1), or 75 bpm (4:1)
- Narrow QRS complexes
Classic "sawtooth" baseline at ~300 bpm, with variable AV block producing an irregularly irregular ventricular response
🟡 4. AV Heart Blocks (Conduction Blocks)
The AV node or bundle branches fail to conduct the signal properly.
| Type | What happens | ECG Finding |
|---|---|---|
| 1st degree | Delayed conduction | PR interval > 0.20 sec (> 5 small boxes), every P conducts |
| 2nd degree Mobitz I (Wenckebach) | Progressive delay then dropped beat | PR gets longer → longer → longer → QRS drops; then resets |
| 2nd degree Mobitz II | Sudden dropped beats without warning | Fixed PR interval, then suddenly a P wave with no QRS |
| 3rd degree (Complete block) | Atria and ventricles beat independently | P waves and QRS complexes march at completely different rates — total dissociation |
3rd degree block is a medical emergency — the ventricles use a slow escape rhythm (20–40 bpm) to survive.
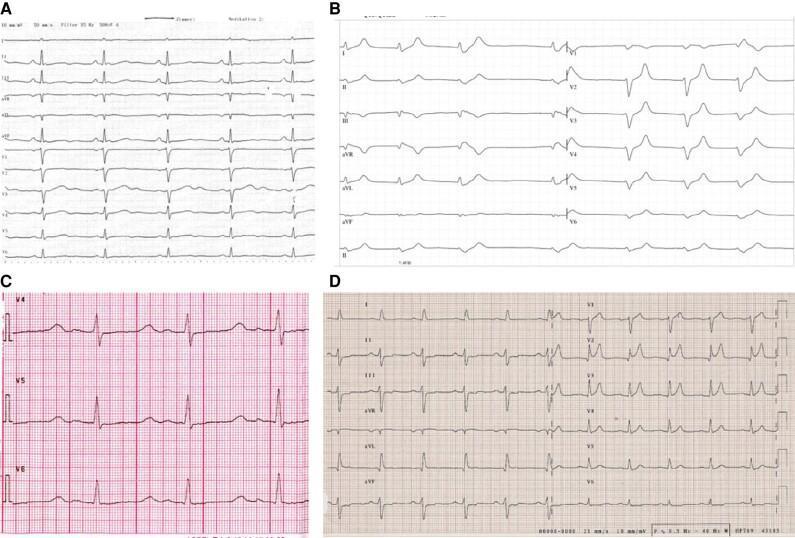
🟡 5. Bundle Branch Blocks (BBB)
The left or right bundle branch fails → one ventricle depolarizes late → wide QRS.
Key rule: QRS ≥ 0.12 sec (≥ 3 small boxes) = bundle branch block
Right Bundle Branch Block (RBBB):
- RSR' pattern in V1 ("rabbit ears" — two upward bumps)
- Wide S wave in I, V5, V6
- QRS ≥ 0.12 sec
Left Bundle Branch Block (LBBB):
- Broad, notched R wave in I, aVL, V5, V6 ("W" shape in V1, "M" shape in V6)
- Deep S wave in V1
- LBBB masks myocardial infarction changes — always treat new LBBB like a possible MI
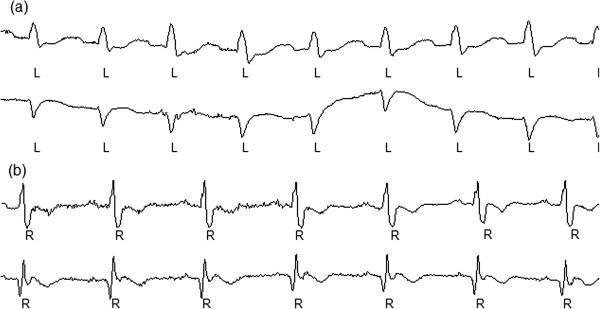
Panel (a) LBBB: broad notched R waves in lateral leads. Panel (b) RBBB: rSR' pattern with prominent S waves
🟢 6. Pericarditis (Inflammation Around the Heart)
Pericarditis has a characteristic 4-stage ECG evolution:
| Stage | Timing | ECG Change |
|---|---|---|
| Stage 1 | Acute | Diffuse ST elevation (saddle-shaped, not convex) + PR depression in most leads |
| Stage 2 | Days | ST and PR normalize |
| Stage 3 | Days–weeks | Diffuse T wave inversion |
| Stage 4 | Weeks | T waves normalize |
Key difference from MI: Pericarditis ST elevation is diffuse (all leads), saddle-shaped, and accompanied by PR depression. MI ST elevation is regional (specific territory) and convex.
🟢 7. Electrolyte Disturbances
Hyperkalemia (High Potassium)
Progression as K⁺ rises:
- Tall, peaked/tented T waves (earliest sign)
- PR prolongation, P wave flattening
- Wide QRS
- Sine wave pattern → Ventricular fibrillation → death
Hypokalemia (Low Potassium)
- Flat T waves
- Prominent U wave (a bump after the T wave — looks like QT prolongation)
- ST depression
Hypercalcemia (High Calcium)
- Short QT interval (calcium shortens ventricular repolarization)
Hypocalcemia (Low Calcium)
- Long QT interval (calcium prolongs repolarization)
🔵 8. Pulmonary Embolism (PE)
A clot in the lung causes right heart strain.
Classic (but not always present) pattern — S1Q3T3:
- S wave in lead I
- Q wave in lead III
- T wave inversion in lead III
Other PE signs:
- Sinus tachycardia (most common)
- Right bundle branch block pattern (right ventricle strain)
- T wave inversions in V1–V4
🔵 9. Wolff-Parkinson-White (WPW) Syndrome
An accessory pathway bypasses the AV node — so the ventricles start activating early before the normal conduction arrives.
ECG Features:
- Short PR interval (< 0.12 sec) — signal bypasses AV node delay
- Delta wave — a slurred upstroke at the beginning of the QRS (pre-excitation)
- Widened QRS
- Increased risk of supraventricular tachycardia
🔵 10. Long QT Syndrome
The QT interval is prolonged (corrected QT > 440 ms in men, > 460 ms in women).
Causes:
- Congenital (channelopathy)
- Drugs (antiarrhythmics like amiodarone, antibiotics, antipsychotics)
- Hypokalemia, hypomagnesemia, hypocalcemia
Risk: Can degenerate into Torsades de Pointes (a dangerous polymorphic VT that looks like a twisting helix on ECG).
PART 8 — Quick Summary Table
| Disease | Key ECG Change | Memory Trick |
|---|---|---|
| Normal sinus rhythm | P→QRS→T, rate 60–100, all intervals normal | The textbook beat |
| STEMI | ST elevation + reciprocal depression + Q waves | "Tombstoning" ST |
| NSTEMI/Ischemia | ST depression + T wave inversion | "Depressed" and "inverted" |
| Atrial fibrillation | No P waves, irregularly irregular | "Irregularly irregular" |
| Atrial flutter | Sawtooth, rate 150 bpm (2:1) | "Flutter = saw" |
| 1st degree AV block | Long PR > 0.20s | Just slow |
| 2nd degree (Wenckebach) | PR gets longer until drop | "Longer, longer, drop" |
| 3rd degree (complete block) | P and QRS completely independent | "Complete divorce" |
| RBBB | RSR' in V1, slurred S in V6 | "Rabbit ears in V1" |
| LBBB | Broad R in V6, deep S in V1 | "Notched M in V6" |
| Pericarditis | Diffuse saddle ST + PR depression | "All leads, PR dips" |
| Hyperkalemia | Tall peaked T waves → wide QRS | "Tent → sine wave" |
| Hypokalemia | Flat T, prominent U wave | "U appear when K low" |
| PE | S1Q3T3 + right strain | "S1Q3T3" |
| WPW | Short PR + delta wave | "Bypass = short PR" |
| Long QT | QT > 440 ms | "Torsades risk" |
Key References
- Goldman-Cecil Medicine, International Edition — Electrocardiographic Waves & Standards
- Costanzo Physiology, 7th Edition — Electrocardiogram
- Braunwald's Heart Disease, 15th Edition — Electrocardiography
- Roberts & Hedges' Clinical Procedures in Emergency Medicine — Electrocardiography
- Harrison's Principles of Internal Medicine, 21st Edition — Cardiac Conduction System
This is a shared conversation. Sign in to Orris to start your own chat.