Enumerate shoulder stabilizers and its function in clinical test as per standard DNB theory examination of 10 marks.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive content from three major orthopaedic textbooks. Let me compile the complete DNB-style 10-mark answer.
Shoulder Stabilizers and Their Function - Clinical Tests
(Standard DNB Theory - 10 Marks)
INTRODUCTION
The glenohumeral joint is a ball-and-socket joint that sacrifices stability for the greatest range of motion of any joint in the body. The humeral head is large relative to the shallow glenoid fossa, making the joint inherently unstable. Stability is maintained by a balance of static and dynamic stabilizers.
(Miller's Review of Orthopaedics 9th Ed.; Campbell's Operative Orthopaedics 15th Ed.)
A. STATIC STABILIZERS
1. Bony Anatomy
- The humeral head has an inclination of 125° and retroversion of 25°
- The glenoid has a slight retrotilt that contributes to posterior containment
- The humeral head surface area is larger than the glenoid - only ~25-30% contact at any time
- Bony articulation provides minimal inherent stability
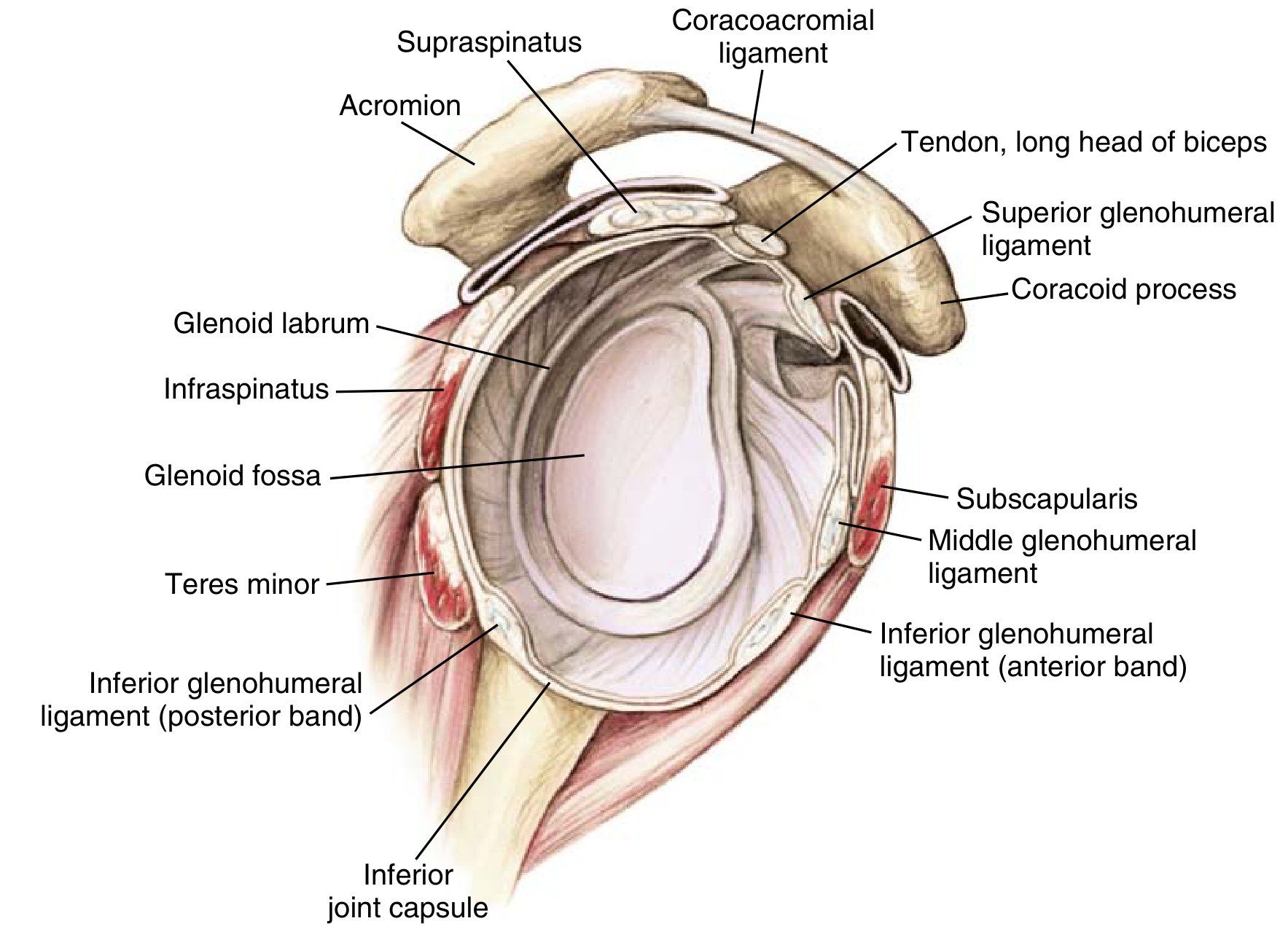
2. Glenoid Labrum
- Fibrocartilaginous rim around the glenoid
- Deepens the socket by 50% and increases surface area
- Acts as a "bumper" against translation of the humeral head
- Anatomic variants: sublabral foramen (anterosuperior) and Buford complex (absent anterosuperior labrum + cord-like MGHL)
3. Glenohumeral Ligaments (Capsule)
The capsule and its thickenings form the primary static restraints. As summarized in Miller's Review (Table 2.1):
| Structure | Function |
|---|---|
| Glenoid labrum | Increases surface area, deepens socket, static stabilizer |
| Coracohumeral ligament (CHL) | Restrains inferior translation and external rotation of the adducted arm |
| Superior GHL (SGHL) | Restrains ER and inferior translation of the adducted or slightly abducted arm |
| Middle GHL (MGHL) (absent in up to 30%) | Restrains anterior translation with arm abducted to 45 degrees |
| IGHL - Anterior band | Restrains anterior and inferior translation with arm in ER + abduction to 90 degrees (position of apprehension) - MOST IMPORTANT |
| IGHL - Posterior band | Restrains posterior and inferior translation with arm in IR + abduction to 90 degrees |
Key point: The IGHL anterior band is the single most important static stabilizer. It is the structure torn in a Bankart lesion.
4. Negative Intra-articular Pressure
- Vacuum seal of the closed capsule generates negative pressure
- Enhances the stabilizing effect of capsuloligamentous structures
- Loss of this vacuum (capsule venting) produces significant inferior translation - the basis of the sulcus sign
B. DYNAMIC STABILIZERS
1. Rotator Cuff Muscles
The rotator cuff provides concavity-compression - compressing the humeral head into the glenoid fossa, resisting translation.
| Muscle | Primary Action | Stabilizing Role |
|---|---|---|
| Supraspinatus | Initiates abduction | Superior compressor; resists superior translation |
| Infraspinatus | External rotation | Posterior compressor; resists posterior translation |
| Teres minor | External rotation (weak) | Assists posterior compression |
| Subscapularis | Internal rotation | Anterior compressor; resists anterior translation |
Together they form a compressive force couple that centers the humeral head in the glenoid throughout all positions of motion.
2. Biceps Tendon (Long Head)
- Runs through the bicipital groove within the rotator interval
- Dynamic stabilizer against anterior and inferior translation
- The transverse humeral ligament stabilizes the biceps tendon in the groove
3. Periscapular / Scapulothoracic Muscles
- Serratus anterior, trapezius, rhomboids, levator scapulae
- Position the scapula (and therefore the glenoid) optimally under the humeral head
- Scapulothoracic dyskinesia impairs glenohumeral stability - important in MDI
4. Deltoid
- Works synergistically with the rotator cuff
- The rotator cuff must fix the fulcrum (humeral head against glenoid) for the deltoid to effectively elevate the arm
5. Proprioception
- Mechanoreceptors in the capsule and ligaments provide proprioceptive feedback
- Failure of proprioception contributes to instability, especially in MDI
- Patients with MDI have reduced proprioception compared to normal controls
C. CLINICAL TESTS FOR SHOULDER INSTABILITY
1. Apprehension Test (Crank Test)
- Technique: Patient supine; arm abducted 90°, elbow at 90°; examiner slowly externally rotates the arm
- Positive: Patient experiences a sense of apprehension (fear of dislocation), not merely pain
- Tests: Anterior capsulolabral complex and IGHL anterior band
- Significance: Anterior glenohumeral instability
2. Relocation Test (Fowler / Jobe Test)
- Technique: Immediately after apprehension test; examiner applies a posteriorly directed force on the proximal humerus
- Positive: Relief of apprehension
- Significance: Confirms anterior instability; most sensitive test for anterior instability (positive predictive value 96%)
- Together, apprehension + relocation tests are the most diagnostic combination for anterior shoulder instability
3. Load-and-Shift Test
- Technique: Patient supine; arm abducted 90°, elbow bent; examiner loads (compresses) the humeral head into glenoid, then applies anterior and posterior translatory force
- Grading:
- 1+: Translation up to the glenoid rim (0-1 cm)
- 2+: Translation over the glenoid rim and reduces (1-2 cm)
- 3+: Translation over the glenoid rim, does not reduce (>2 cm) = frank dislocation
- Significance: Quantifies degree of instability; can assess anterior, posterior, and inferior laxity
4. Sulcus Sign (Inferior Instability)
- Technique: Patient seated, arm at side; examiner applies inferior traction to the arm
- Positive: A sulcus (dimple) appears below the acromion; graded by gap in cm (1+: <1 cm; 2+: 1-2 cm; 3+: >2 cm)
- Clinical pearl: If the sulcus sign persists with the arm in >45° ER, it indicates incompetency of the rotator interval (SGHL + CHL)
- Significance: Inferior laxity; multidirectional instability (MDI)
5. Posterior Jerk Test
- Technique: Patient seated; arm abducted 90° and maximally internally rotated; examiner applies axial compressive force and then horizontally adducts the arm across the body
- Positive: A "clunk" or "jerk" felt as the humeral head subluxates posteriorly, then spontaneously reduces
- Significance: Posterior glenohumeral instability
6. Kim Test
- Technique: Patient seated; arm abducted 90°; examiner applies axial compression and superiorly directed force while simultaneously adducting and depressing the arm
- Positive: Sudden pain or jerk
- Significance: Posteroinferior labral tear; posterior instability
7. Bony Apprehension Test
- Technique: Arm placed at below 45° abduction and 45° ER (below the classic apprehension position)
- Positive: Apprehension or pain at this low angle of abduction
- Significance: Suggests significant bony Bankart lesion or moderate-to-severe anterior glenoid bone loss (as opposed to soft-tissue Bankart)
8. Gagey Test (Hyperabduction Test)
- Technique: Examiner stabilizes the scapula and passively abducts the arm
- Positive: Hyperabduction >105° (or >15° asymmetric increase compared to contralateral)
- Significance: Incompetency of the IGHL complex; MDI
D. KEY SUMMARY TABLE (Miller's Table 4.7)
| Test | Technique | Significance |
|---|---|---|
| Apprehension test | Supine, 90° abduction + ER | Apprehension = anterior instability |
| Relocation test | Posterior force after apprehension | Relief = anterior instability |
| Load-and-shift test | Ant/post force on humeral head | Grade of translation = laxity/instability |
| Jerk test | Posterior force, arm adduction + FF | "Clunk" = posterior subluxation |
| Sulcus sign | Inferior force, arm at side | Increased gap = inferior laxity/MDI |
CLINICAL CORRELATIONS (DNB High-Yield Points)
| Pathology | Stabilizer Involved | Relevant Clinical Test |
|---|---|---|
| Bankart lesion (anterior dislocation) | IGHL anterior band + labrum | Apprehension-relocation test |
| Bony Bankart (>25% glenoid loss) | Bony glenoid | Bony apprehension test (at <45° ABD) |
| Reverse Bankart (posterior dislocation) | IGHL posterior band + posterior labrum | Jerk test, Kim test |
| MDI | Patulous inferior capsule + rotator interval | Sulcus sign, Gagey test, Beighton score |
| Rotator cuff tear | Dynamic stabilizers | Drop arm, Jobe, Hornblower's |
| HAGL lesion | Humeral avulsion of IGHL | MR arthrogram, anterior instability tests |
Sources: Miller's Review of Orthopaedics 9th Ed. (Tables 2.1 & 4.7) | Rockwood and Green's Fractures in Adults 10th Ed. 2025 (Ch. 35) | Campbell's Operative Orthopaedics 15th Ed. 2026 (Ch. 13, 52)
This is a shared conversation. Sign in to Orris to start your own chat.