Effect of ccb on pulse rate
Reading File
Searching the Web
calcium channel blockers effect on heart rate pulse rate dihydropyridine non-dihydropyridine
Finding Sources
Searching PubMed
"calcium channel blockers" AND "heart rate"
Reading File
Finding Sources
Reading File
Reading File
Here is a thorough breakdown of how calcium channel blockers (CCBs) affect pulse rate:
Effect of CCBs on Pulse Rate
CCBs are divided into two main subclasses, and their effects on heart rate are opposite.
1. Dihydropyridines (DHPs) - Increase Pulse Rate
Examples: Nifedipine, amlodipine, felodipine, nicardipine, isradipine, nisoldipine
Mechanism:
- DHPs bind preferentially to L-type calcium channels in vascular smooth muscle, causing potent peripheral arterial vasodilation with minimal direct cardiac effect.
- The sudden drop in systemic vascular resistance triggers baroreceptor-mediated reflex sympathetic activation.
- This reflex leads to increased heart rate (reflex tachycardia) and maintenance or even increase in cardiac output.
Key points:
- Reflex sympathetic activation with slight tachycardia maintains or increases cardiac output in most patients.
- Short-acting nifedipine produces the most pronounced reflex tachycardia and is associated with increased cardiovascular risk - it should NOT be used for hypertension unless the patient is already on a beta-blocker.
- Long-acting formulations (e.g., amlodipine) cause less pronounced tachycardia due to a slower, more gradual onset of vasodilation.
- In overdose, as toxicity becomes severe, tachycardia may eventually transition to bradycardia.
2. Non-Dihydropyridines (Non-DHPs) - Decrease Pulse Rate
Examples: Verapamil (phenylalkylamine), Diltiazem (benzothiazepine)
Mechanism:
- Both verapamil and diltiazem block L-type calcium channels in the myocardium AND vascular smooth muscle.
- This depresses SA nodal automaticity (negative chronotropy) and AV nodal conduction (negative dromotropy).
- Net effect: slowed heart rate (bradycardia) and reduced cardiac output.
Key clinical points:
- Verapamil has the greatest cardiac depressant effect and causes the most heart rate slowing.
- Diltiazem has intermediate effects - less cardiac depression than verapamil, less vasodilation than DHPs.
- Both are used for rate control in atrial fibrillation and SVT precisely because of their AV nodal slowing effect.
- Contraindicated in combination with beta-blockers due to synergistic depression of SA/AV nodal conduction and risk of complete heart block.
- Contraindicated in heart failure with reduced ejection fraction (HFrEF).
Summary Table
| Property | Dihydropyridines (e.g., amlodipine) | Non-DHPs (e.g., verapamil, diltiazem) |
|---|---|---|
| Primary site of action | Vascular smooth muscle | Heart + vascular smooth muscle |
| Effect on pulse rate | Increases (reflex tachycardia) | Decreases (bradycardia) |
| Mechanism of HR change | Baroreceptor-mediated reflex | Direct SA/AV node depression |
| Cardiac output | Maintained or increased | Decreased |
| Use in AF rate control | No | Yes |
| Use in SVT | No | Yes |
| Risk with beta-blocker combo | Lower | High (AV block risk) |
Clinical Application
- When a patient on a dihydropyridine has bothersome palpitations or tachycardia, a beta-blocker is often added - this is why the combination of DHP + beta-blocker is a standard angina regimen.
- Diltiazem is the preferred non-DHP CCB in ACS (non-ST elevation) for patients who cannot tolerate beta-blockers, as it slows heart rate and reduces ischemia.
- In overdose, all CCBs can eventually cause bradycardia, AV block, and cardiovascular collapse, regardless of subclass.
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed.; Goldman-Cecil Medicine; Rosen's Emergency Medicine
Approach to bilateral lower limb swelling
Finding Sources
Searching the Web
approach to bilateral lower limb swelling clinical evaluation causes investigations
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Excellent - I have all the key content needed. Here is a thorough, structured answer:
Approach to Bilateral Lower Limb Swelling
Pathophysiology of Edema
Edema forms when fluid accumulates in the interstitial space due to one or more of the following mechanisms:
- Increased capillary hydrostatic pressure - e.g., heart failure, venous obstruction
- Decreased plasma oncotic pressure - e.g., hypoalbuminemia (liver disease, nephrotic syndrome, malnutrition)
- Increased capillary permeability - e.g., inflammation, allergy
- Increased interstitial oncotic pressure - e.g., myxedema (hypothyroidism)
- Lymphatic obstruction - e.g., lymphedema
Step 1: Determine Distribution (Pivotal Point)
Bilateral leg edema almost always points to a systemic cause - this is the single most important initial distinction.
"Although there are some local diseases that can present with bilateral leg edema, the first step in such patients is always to look for systemic causes." - Symptom to Diagnosis, 4th Ed.
Differential Diagnosis of Bilateral Lower Limb Swelling
A. Systemic Causes (most common)
1. Cardiovascular
| Condition | Mechanism | Key Clues |
|---|---|---|
| Heart failure (HFrEF / HFpEF) | Raised venous hydrostatic pressure | Dyspnea, elevated JVP, S3 gallop, crackles |
| Constrictive pericarditis | Impaired cardiac filling | Kussmaul's sign, pericardial knock, ascites |
| Pulmonary hypertension | Right heart strain / RV failure | Exertional dyspnea, loud P2, RV heave |
2. Hepatic
- Cirrhosis - hypoalbuminemia + portal hypertension
- Key clues: jaundice, spider angiomata, gynecomastia, splenomegaly, ascites, flat/low JVP (distinguishes from cardiac)
3. Renal
- Chronic kidney disease - sodium and water retention
- Nephrotic syndrome - massive proteinuria (>3.5 g/day), hypoalbuminemia, hyperlipidemia; periorbital edema is characteristic
- Key test: urine albumin/creatinine ratio, BUN/creatinine
4. Nutritional / GI
- Malnutrition, malabsorption, protein-losing enteropathy
- Mechanism: hypoalbuminemia reducing plasma oncotic pressure
5. Endocrine
- Hypothyroidism (Myxedema) - non-pitting edema from increased interstitial glycosaminoglycans
- Note: true hypothyroid edema is typically non-pitting, so it will NOT respond to diuretics
6. Medications (common and often missed)
| Drug Class | Examples |
|---|---|
| Calcium channel blockers | Amlodipine, nifedipine (DHP class - afferent arteriolar dilation) |
| Direct vasodilators | Hydralazine, minoxidil |
| Beta-blockers | - |
| Hormones | Estrogens, progesterones, testosterone, corticosteroids |
| NSAIDs | Sodium/water retention |
| Thiazolidinediones | Pioglitazone (common cause) |
| MAO inhibitors | - |
7. Hematologic
- Severe anemia - high-output state with peripheral vasodilation
B. Local / Vascular Causes
| Condition | Key Features |
|---|---|
| Bilateral DVT | Painful, asymmetric, risk factors (malignancy, immobility); less commonly bilateral |
| Bilateral pelvic/retroperitoneal mass | Lymphadenopathy, pelvic malignancy obstructing venous/lymphatic drainage |
| Chronic venous insufficiency | Pitting edema, worse at end of day, relieved by elevation, skin changes (hyperpigmentation, lipodermatosclerosis), varicosities |
| Bilateral lymphedema | Non-pitting, "tree trunk" pattern, Stemmer sign positive, buffalo hump on dorsum of foot |
| Lipedema | Bilateral, non-pitting, excessive subcutaneous fat, spares the feet, not affected by elevation - common in obese women, often familial |
Step 2: History
Key questions to ask:
- Onset and duration - acute (DVT, acute HF) vs. chronic (venous insufficiency, cirrhosis)
- Diurnal variation - worse by evening = venous/gravitational; worse in morning = cardiac/renal
- Associated symptoms:
- Dyspnea, orthopnea, PND → Heart failure
- Abdominal distension, jaundice → Cirrhosis
- Frothy urine → Nephrotic syndrome
- Fatigue, cold intolerance, constipation → Hypothyroidism
- Drug history - especially CCBs, steroids, NSAIDs, thiazolidinediones
- Risk factors - alcohol use, viral hepatitis exposure, malignancy, immobility, cardiac disease, diabetes, hypertension
- Family history - lymphedema (Milroy disease, Meige disease)
Step 3: Physical Examination
| Finding | Suggests |
|---|---|
| Elevated JVP | Heart failure, constrictive pericarditis |
| Flat/low JVP | Cirrhosis, nephrotic syndrome, malnutrition |
| Pitting edema | Cardiac, renal, hepatic, venous, medication-induced |
| Non-pitting edema | Lymphedema, myxedema |
| Ascites + splenomegaly | Cirrhosis |
| S3 gallop, crackles | Heart failure |
| Periorbital edema | Nephrotic syndrome |
| Stemmer sign (inability to pinch skin at base of second toe) | Lymphedema |
| Tree trunk pattern, buffalo hump | Lymphedema |
| Skin changes (pigmentation, ulcers above/behind medial malleolus) | Chronic venous insufficiency |
| Responds to overnight elevation | Cardiac/venous edema; not lymphedema |
| Spider angiomata, gynecomastia, palmar erythema | Cirrhosis |
Step 4: Investigations
First-line (all patients)
| Test | Evaluates |
|---|---|
| CBC | Anemia, infection |
| Serum albumin | Hypoalbuminemia (hepatic, nephrotic, nutritional) |
| Liver function tests (ALT, AST, bilirubin, ALP, PT) | Cirrhosis / hepatic cause |
| Renal function (BUN, creatinine) | CKD |
| Urine albumin/creatinine ratio or 24-hr urine protein | Nephrotic syndrome |
| Urinalysis | Proteinuria, casts |
| Thyroid function (TSH) | Hypothyroidism |
| Blood glucose / HbA1c | Diabetes (risk factor for cardiac/renal disease) |
Second-line (selected patients)
| Test | Indication |
|---|---|
| ECG | Suspected cardiac cause |
| Chest X-ray | Cardiomegaly, pleural effusions, pulmonary edema |
| Echocardiogram | Suspected HF, pulmonary hypertension, constrictive pericarditis |
| BNP / NT-proBNP | Confirming/ruling out heart failure |
| Hepatitis B and C serologies | Suspected cirrhosis |
| Abdominal ultrasound | Cirrhosis, ascites, portal hypertension |
| Duplex venous ultrasound | Suspected DVT or venous insufficiency |
| Lymphoscintigraphy / MRI | Suspected lymphedema |
| CA-125, pelvic ultrasound | Suspected ovarian malignancy causing venous obstruction |
Diagnostic Flowchart
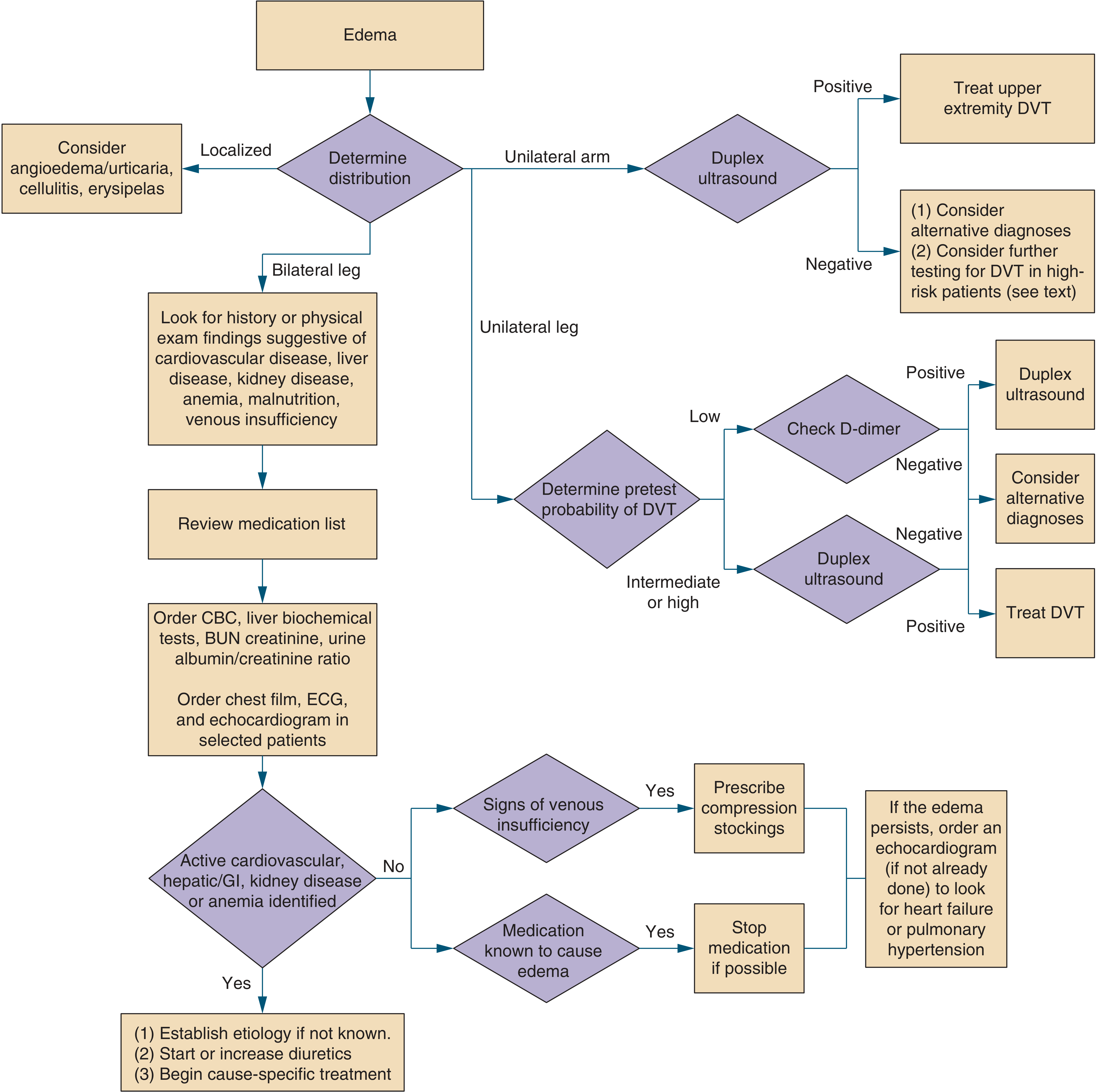
Figure: Diagnostic approach to edema - Symptom to Diagnosis, 4th Ed.
Step 5: Management Principles (cause-directed)
| Cause | Management |
|---|---|
| Heart failure | Diuretics (furosemide), ACEi/ARB, beta-blockers, fluid/salt restriction |
| Cirrhosis | Salt restriction, spironolactone +/- furosemide, treat underlying cause |
| Nephrotic syndrome | Treat underlying glomerular disease, diuretics, ACEi (reduce proteinuria) |
| Medication-induced | Stop/switch offending drug if possible |
| Hypothyroidism | Thyroxine replacement |
| Chronic venous insufficiency | Compression stockings, limb elevation |
| Lymphedema | Complex decongestive therapy (CDT), compression garments; does not respond to diuretics |
| DVT | Anticoagulation |
Key clinical pearls:
- Always check bilateral vs. unilateral first - bilateral = systemic until proven otherwise.
- JVP is one of the most useful bedside signs to distinguish cardiac (elevated) from hepatic/renal (normal or low) causes.
- Non-pitting edema = lymphedema or myxedema - diuretics will not help.
- A thorough drug history will identify a reversible cause in many patients.
- When no systemic cause is found after workup, consider venous insufficiency, lymphedema, or lipedema.
Sources: Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.; Sabiston Textbook of Surgery; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.