Adult male 24 with high IgE level
Reading File
Finding Sources
Finding Sources
Searching PubMed
elevated IgE causes differential diagnosis
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Now I have excellent textbook content. Let me compile a comprehensive answer.
High IgE in a 24-Year-Old Male - Clinical Approach
Normal Reference Range
In adults, total serum IgE mean is ~13.2 kU/L, with the upper limit of normal at roughly +1 SD (~41 kU/L). The distribution is heavily right-skewed, so many labs use logarithmic transformation for reference ranges. A key point: an elevated IgE strongly suggests allergic disease, but a normal IgE does not rule it out.
Causes of Elevated IgE
1. Atopic/Allergic Conditions (most common)
- Allergic rhinitis - one of the most prevalent causes in young adults
- Atopic dermatitis (eczema)
- Allergic asthma
- Food allergy - peanuts, tree nuts, shellfish, etc.
- Insect venom hypersensitivity
- Occupational allergy (e.g., latex)
Note: Total IgE is moderately useful for atopic conditions, but allergen-specific IgE testing is far more sensitive and specific for diagnosing the exact trigger.
2. Parasitic Infections (classic cause of markedly elevated IgE)
IgE levels >1000 kU/L are regularly found in patients with parasitic infestations. Conditions to consider in a 24-year-old:
| Parasite | Disease |
|---|---|
| Toxocara canis | Visceral larva migrans |
| Capillaria philippinensis | Intestinal capillariasis |
| Schistosoma mansoni | Schistosomiasis |
| Ancylostoma spp. | Hookworm (ancylostomiasis) |
| Filarial worms | Filariasis |
| Echinococcus spp. | Echinococcosis |
IgE levels fall considerably after successful antiparasitic treatment.
3. Allergic Bronchopulmonary Aspergillosis (ABPA)
- Requires IgE >1000 IU/mL as a major criterion
- Seen in patients with asthma or cystic fibrosis
- Also requires positive Aspergillus skin test or specific IgE to A. fumigatus
- This is one of the most diagnostically useful indications for total IgE measurement
4. Primary Immunodeficiency Syndromes with High IgE
| Syndrome | Gene/Mechanism |
|---|---|
| Hyper-IgE (Job) Syndrome | STAT3 mutation (autosomal dominant) |
| DOCK8 deficiency | DOCK8 mutation (autosomal recessive) |
| Wiskott-Aldrich Syndrome | WAS gene defect (X-linked) |
| Nezelof Syndrome | Partial cellular immunodeficiency |
| Omenn Syndrome | Partial T-cell deficiency |
| DiGeorge Syndrome | 22q11.2 deletion |
Hyper-IgE (Job) Syndrome specifically features:
- IgE levels from 2,000 to 50,000 kU/L (extremely high)
- Recurrent staphylococcal infections (skin abscesses, pneumonia with pneumatoceles)
- Eczema and eosinophilia
- Coarse facial features
- Despite markedly elevated IgE and strong immediate skin-test reactivity, asthma is NOT common
5. Other/Miscellaneous
- Certain malignancies (some lymphomas, especially Hodgkin's)
- IgE myeloma (very rare)
- Graft-versus-host disease
- Heavy smoking
Approach to Investigation in This Patient
Initial workup:
- Complete blood count with differential - look for eosinophilia (common in parasitic infection and hyper-IgE syndrome)
- Quantify total IgE level - the degree of elevation guides the differential:
- Mildly elevated (41-200 kU/L): atopy most likely
- Moderately elevated (200-1000 kU/L): atopy, early parasitic disease
- Markedly elevated (>1000 kU/L): parasitic infection, ABPA, or hyper-IgE syndrome most likely
- Allergen-specific IgE panel - guided by history (inhalants, foods, occupation)
- Stool O&P (ova and parasites) x3 + serology for relevant parasites based on travel/exposure history
- Chest X-ray / pulmonary function - if respiratory symptoms
- Aspergillus-specific IgE and precipitins - if asthma or pulmonary infiltrates present
If hyper-IgE syndrome suspected (very high IgE + recurrent abscesses + eczema):
- STAT3 gene mutation testing
- Immunology referral
Key Clinical Pearl
The degree of IgE elevation is the most helpful guide to the differential:
- Total IgE in allergic disease typically ranges from mildly to moderately elevated
- Total IgE in ABPA must exceed 1000 IU/mL to meet diagnostic criteria
- Total IgE in hyper-IgE syndrome is usually 2000-50,000 kU/L - extreme elevation
- Total IgE in parasitic disease regularly exceeds 1000 kU/L
A thorough travel history, skin examination (eczema, abscesses), and pulmonary assessment will guide the workup.
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods (56th ed.); Quick Compendium of Clinical Pathology (5th ed.); Cummings Otolaryngology Head and Neck Surgery; Fishman's Pulmonary Diseases and Disorders
Itch
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Pruritus (Itch) - Comprehensive Overview
In the context of this patient (24M, high IgE), pruritus is the cardinal symptom linking his elevated IgE to the clinical picture - most likely atopic dermatitis, urticaria, or an allergic/parasitic process. Here is the full framework.
Definition & Epidemiology
Pruritus is the most common symptom in dermatology. The WHO Global Burden of Disease study lists it among the 50 most frequent interdisciplinary symptoms. It is considered chronic when present for more than 6 weeks, and an estimated one-fifth of the global population has chronic pruritus with significantly impaired quality of life.
IFSI Classification of Chronic Pruritus
The International Forum for the Study of Itch (IFSI) classifies pruritus by two axes:
By skin appearance:
- Group I - Pruritus on inflamed skin (e.g., atopic dermatitis, urticaria, psoriasis)
- Group II - Pruritus on normal-appearing skin (systemic or neurologic cause more likely)
- Group III - Pruritus with chronic scratch lesions (prurigo nodularis)
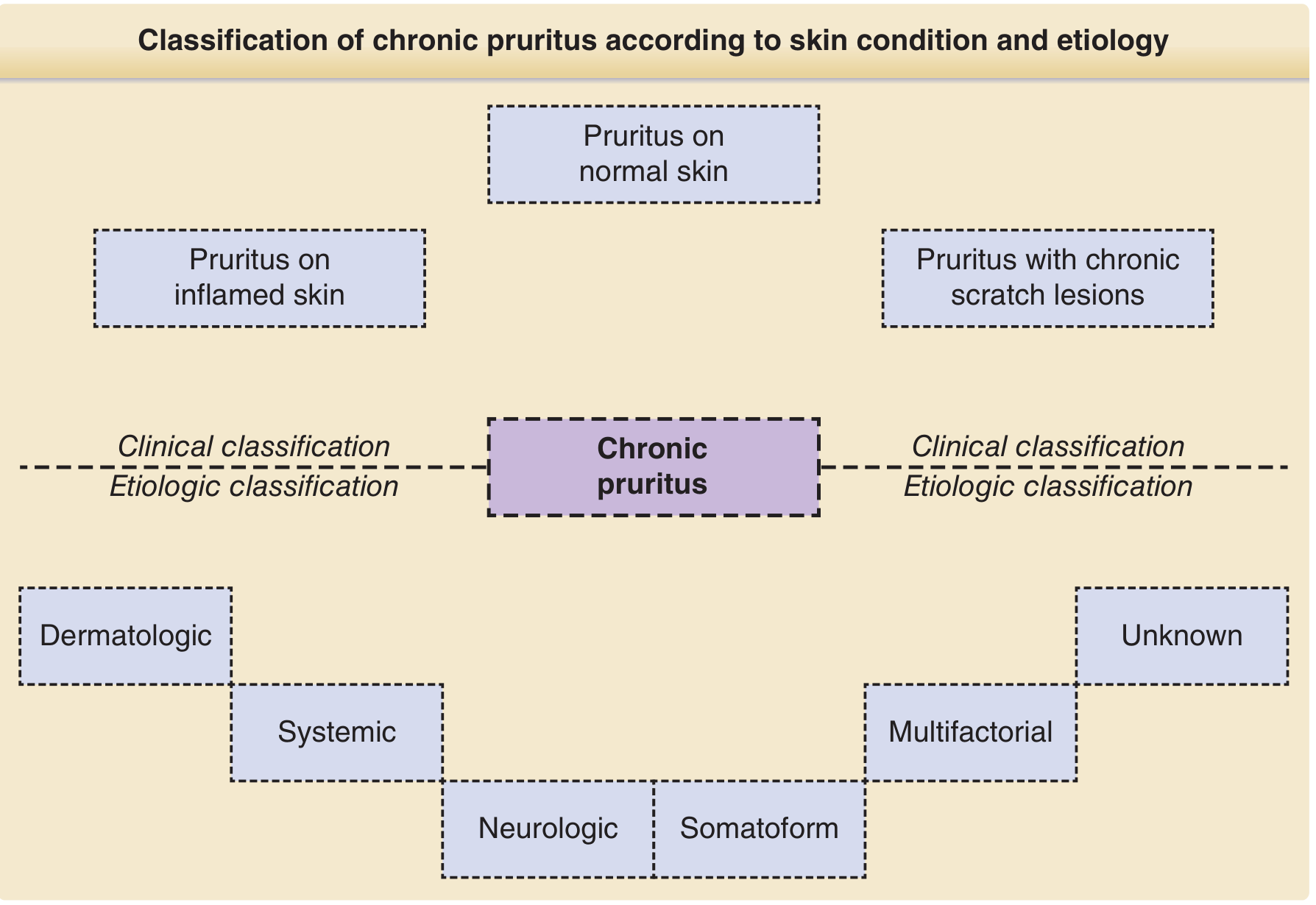
By etiology:
| Category | Examples |
|---|---|
| Dermatologic | Atopic dermatitis, urticaria, psoriasis, contact dermatitis, scabies |
| Systemic | Renal failure (uremic pruritus), cholestasis, thyroid disease, hematologic malignancy (polycythemia vera, lymphoma), iron deficiency, parasitic infection |
| Neurologic | Notalgia paresthetica, postherpetic neuralgia, multiple sclerosis, brachioradial pruritus |
| Somatoform | Psychogenic/functional pruritus |
| Multifactorial | Multiple overlapping causes (e.g., AD + stress) |
| Unknown | No identifiable cause |
In This Patient (High IgE + Pruritus)
The combination of high IgE and itch points toward these diagnoses:
1. Atopic Dermatitis (AD) - Most Likely
- Pruritus is the defining and most distressing symptom of AD - it is one of the major diagnostic criteria (Hanifin-Rajka criteria: pruritus is obligatory)
- Other major features: facial/extensor rash in infants, flexural lichenification, personal/family history of atopic triad (AD, asthma, allergic rhinitis)
- In AD, histamine is NOT the primary mediator of itch - this explains why antihistamines have relatively poor efficacy in AD compared to urticaria
- The itch-scratch cycle worsens the skin barrier and promotes S. aureus colonization (>70% of AD patients)
- Nocturnal pruritus is characteristic and leads to sleep disruption, anxiety, and depression (43-57% of adult AD patients screen positive for these comorbidities)
2. Urticaria
- Pruritic wheals are IgE/mast cell-driven
- Histamine IS the dominant mediator here - antihistamines work well
- H1 antihistamines are first-line (loratadine, fexofenadine, cetirizine)
3. Parasitic Infection (especially with IgE >1000 kU/L)
- Pruritus can be prominent (e.g., hookworm causing cutaneous larva migrans, schistosomiasis - "swimmer's itch")
Pathophysiology of IgE-Mediated Itch
- Allergen cross-links IgE on mast cells/basophils
- Degranulation releases histamine, tryptase, prostaglandins, leukotrienes
- Histamine binds H1 receptors on unmyelinated C-fibers in skin
- Signal travels via dorsal root ganglia → spinothalamic tract → somatosensory cortex
- In AD specifically, additional mediators dominate: IL-31 (the "itch cytokine"), substance P, TSLP, IL-4/IL-13 - which is why anti-IL-31 (nemolizumab) and dupilumab (anti-IL-4Rα) are more effective than antihistamines in AD
Management of Pruritus - Step-by-Step
General Measures (all causes)
- Emollients daily to prevent xerosis and restore skin barrier
- Avoid identified allergens and irritants
- Cool environment (heat worsens itch)
- Topical antipruritic compounds: urea, menthol, polidocanol
Targeted Therapy by Etiology
| Cause | Treatment |
|---|---|
| Atopic dermatitis | Topical corticosteroids, topical calcineurin inhibitors (tacrolimus, pimecrolimus), dupilumab (anti-IL-4Rα), cyclosporine for severe disease |
| Urticaria | H1 antihistamines (1st line) → H2 antagonist + montelukast (add-on) → omalizumab (anti-IgE, 2nd line for chronic urticaria refractory to antihistamines) |
| Neuropathic pruritus | Gabapentinoids (gabapentin, pregabalin) |
| Cholestatic pruritus | Cholestyramine, rifampicin, naltrexone, UVB phototherapy |
| Uremic/renal pruritus | UVB phototherapy (80-90% improvement), naltrexone |
| Paraneoplastic | Antidepressants (paroxetine), treat underlying malignancy |
Antihistamines in Detail
- Sedating (1st gen): Diphenhydramine, hydroxyzine - useful at bedtime for nocturnal itch; anticholinergic side effects (urinary retention, dry mouth, constipation)
- Non-sedating (2nd gen): Loratadine, fexofenadine, cetirizine - preferred daytime use, can dose up to 4x daily for chronic urticaria
- Doxepin: Dual H1/H2 blocker + TCA; 10-75 mg at night; also available as 5% topical cream (short-term)
- Key point: Antihistamines provide poor itch control in AD because histamine is not the primary pruritogen there
Phototherapy
- NB-UVB effective for renal, cholestatic, polycythemia vera-associated, and chronic urticaria-associated pruritus
- PUVA effective for aquagenic pruritus and photodermatoses
Biologics & Emerging Therapies
- Omalizumab (anti-IgE): Approved for chronic spontaneous urticaria refractory to antihistamines - particularly relevant for a patient with high IgE
- Dupilumab (anti-IL-4Rα): First-line biologic for moderate-to-severe AD
- Nemolizumab (anti-IL-31Rα): Targets the primary itch cytokine in AD
- Remibrutinib (BTK inhibitor): Phase III data shows promise in chronic spontaneous urticaria resistant to H1 antagonists
Bottom Line for This Patient
Given high IgE + itch in a 24-year-old male:
- The most likely diagnosis is atopic dermatitis or allergic urticaria
- If IgE is markedly elevated (>1000), consider parasitic infection or ABPA alongside
- Start workup: CBC with differential (eosinophil count), allergen-specific IgE panel, stool O&P if travel history suggests parasites
- Empirical management: emollients + non-sedating H1 antihistamine while workup proceeds
- If AD confirmed: step up to topical corticosteroids or calcineurin inhibitors; biologics (dupilumab) for moderate-severe disease
- If chronic urticaria: antihistamines → omalizumab if refractory (directly targets IgE axis)
Sources: Fitzpatrick's Dermatology (Vol 1&2); Harrison's Principles of Internal Medicine 22E; Henry's Clinical Diagnosis and Management by Laboratory Methods
If the patient has no rash on normal skin on face scalp, plam and foot
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
This is exactly what's needed. Now I have a complete, authoritative answer.
Pruritus on Normal Skin (IFSI Group II) + High IgE - No Primary Rash
This is now a "generalized unexplained pruritus" presentation. The absence of rash on face, scalp, palms, and soles effectively rules out most primary dermatologic causes and shifts the differential firmly toward systemic, hematologic, parasitic, or early occult dermatologic disease.
Revised Differential Diagnosis (High Priority)
The combination of normal skin + high IgE + generalized pruritus in a 24-year-old male makes these the leading diagnoses:
1. Parasitic Infection (Top Priority with High IgE)
- Scabies - classic distribution spares the face and scalp in adults (face involvement mainly in infants). Burrows are found in interdigital webs, wrists, elbows, axillae, genitals, belt line. The itch is worse at night and mediated by immunologic sensitization to the mite. However, IgE is only modestly elevated in typical scabies.
- Tissue-invasive helminths (hookworm, ascariasis, strongyloidiasis, toxocariasis, filariasis, schistosomiasis) - these markedly elevate IgE (>1000 kU/L) and cause generalized pruritus without a primary rash. Travel history is critical.
- Onchocerciasis ("river blindness") - causes persistent severe generalized pruritus often without a visible rash initially; endemic to sub-Saharan Africa/Latin America
2. Hematologic Malignancy
| Condition | Pruritus Prevalence | Key Features |
|---|---|---|
| Hodgkin lymphoma | up to 30% | Generalized, nocturnal, with chills/sweating; may precede diagnosis; severe pruritus = poor prognosis indicator |
| Polycythemia vera | 30-50% | Aquagenic pruritus (triggered by water/bathing); JAK2 V617F mutation; ruddy complexion |
| Non-Hodgkin lymphoma | ≤10% | Less common |
| Hypereosinophilic syndrome | Variable | High eosinophils + high IgE |
| Cutaneous T-cell lymphoma (Sézary) | 60-90% | Can precede visible skin changes |
A population-based study found patients with chronic pruritus without skin findings had a 2-fold increased risk of hematologic malignancy and 3.7-fold increased risk of bile duct malignancy - making workup mandatory in this patient.
3. Early/Occult Bullous Dermatoses
- Bullous pemphigoid (pre-bullous phase) - presents as intense generalized pruritus for weeks/months before blisters appear; IgE can be elevated; more common in elderly but reported in young adults
- Dermatitis herpetiformis - pruritic, associated with celiac disease; anti-tTG IgA antibodies diagnostic; lesions may be excoriated and not recognized as primary
4. Systemic/Metabolic Causes
| Condition | Mechanism |
|---|---|
| Renal failure (uremic pruritus) | Retained pruritogens, μ-opioid receptor upregulation |
| Primary biliary cholangitis / cholestasis | Bile acids, endogenous opioids; often the presenting symptom (80%) |
| Thyroid disease (hyper- or hypothyroidism) | Both can cause generalized pruritus |
| Iron deficiency (even without anemia) | Reduced tissue iron → impaired itch threshold |
| Diabetes mellitus | Peripheral neuropathy, dry skin |
| Hyperparathyroidism | Calcium/phosphate deposition in skin |
5. Drug-Induced Pruritus
- Opioids (histamine release from mast cells)
- ACE inhibitors, statins, diuretics, NSAIDs
- Always take a full medication history
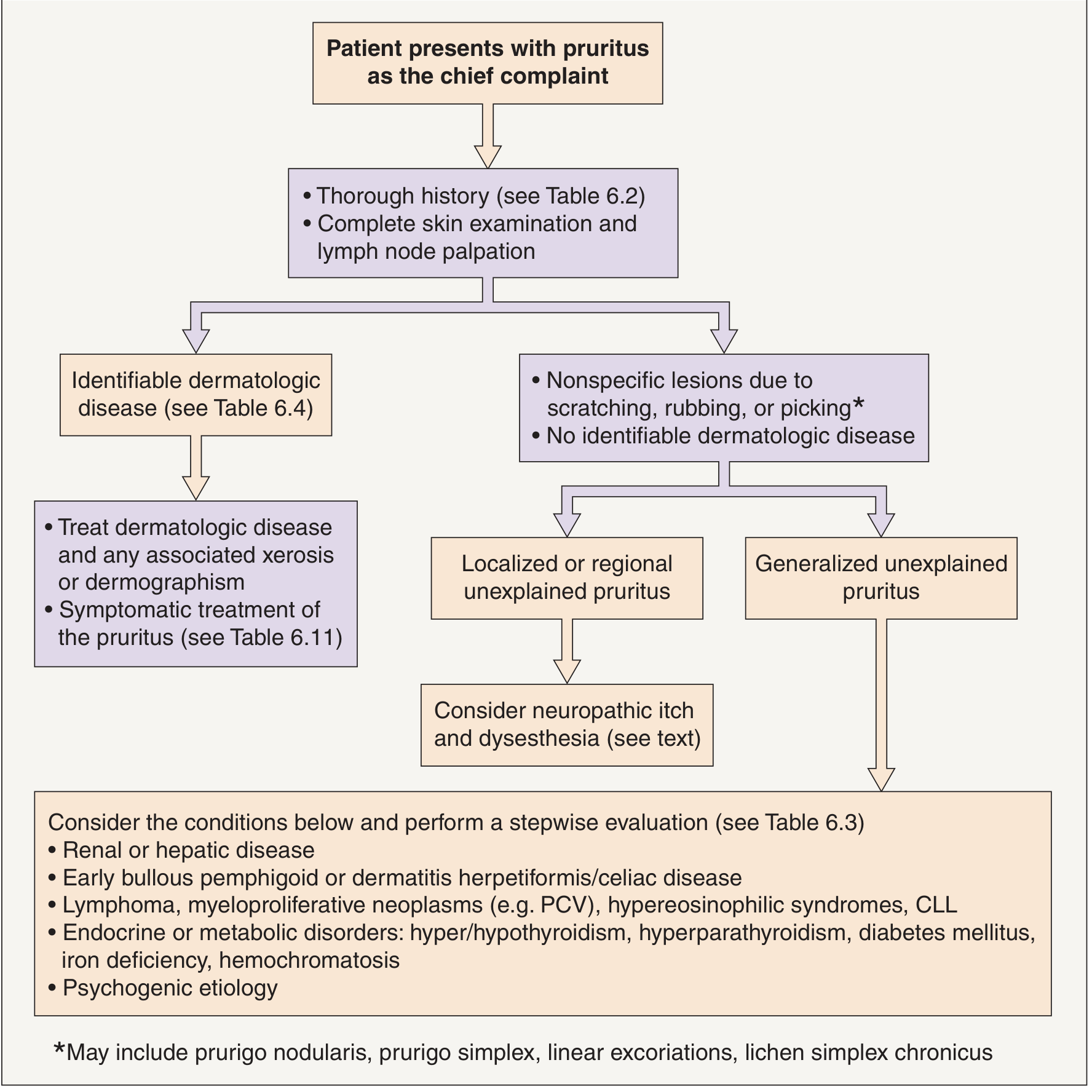
Stepwise Investigation (from Dermatology textbook - Table 6.3)
Basic Initial Evaluation (Order First)
- CBC with differential and platelets - look for eosinophilia (parasites, hypereosinophilic syndrome), polycythemia, lymphocytosis
- ESR, CRP
- Creatinine, BUN - renal disease
- LFTs: transaminases, alkaline phosphatase, bilirubin - hepatic/cholestatic disease
- LDH - lymphoma marker
- TSH - thyroid disease
- Fasting glucose - diabetes
- Serum ferritin, iron, TIBC - iron deficiency
Additional Evaluation (Based on Initial Results)
- Skin biopsy with direct immunofluorescence - even normal-appearing skin can show bullous pemphigoid or dermatitis herpetiformis
- Serum total and allergen-specific IgE - already elevated; now test specific allergens
- Serum protein electrophoresis / immunofixation - paraprotein
- Viral hepatitis panel (HBV, HCV) + HIV testing
- Anti-BP180 and anti-BP230 antibodies - bullous pemphigoid
- Anti-tissue transglutaminase IgA - dermatitis herpetiformis/celiac
- Serum tryptase - mastocytosis
- Stool for ova and parasites (x3 samples)
- Parathyroid function (Ca, PO4, PTH)
Imaging
- Chest X-ray or CT - lymphadenopathy, mediastinal mass (Hodgkin)
- Abdominal/pelvic ultrasound or CT - hepatosplenomegaly, lymphadenopathy
- Lymph node ultrasonography
Physical Examination Focus
- Palpate all peripheral lymph node groups (cervical, supraclavicular, axillary, inguinal) - essential in pruritus without skin disease
- Look for hepatosplenomegaly
- Skin: assess for dermographism, excoriations, subtle burrows
Most Likely Diagnosis in This Patient
Given: 24M + high IgE + generalized pruritus + normal skin (no rash)
| Priority | Diagnosis | Why |
|---|---|---|
| 1st | Parasitic infection (helminths) | High IgE + normal skin is the classic presentation; ask about travel |
| 2nd | Hodgkin lymphoma | Young male, nocturnal pruritus, high IgE seen in ~30%; urgent to exclude |
| 3rd | Hypereosinophilic syndrome | High IgE + eosinophilia + generalized pruritus |
| 4th | Pre-bullous bullous pemphigoid | Can present with pruritus alone for months before blisters |
| 5th | Iron deficiency / thyroid disease | Common, easily tested |
Order CBC with differential immediately - eosinophil count is the single most important result to differentiate parasitic vs. hematologic vs. systemic cause in a young patient with high IgE and normal skin.
Sources: Dermatology 2-Volume Set 5e (Bolognia); Fitzpatrick's Dermatology; Harrison's Principles of Internal Medicine 22E; Harriet Lane Handbook 23e; Andrews' Diseases of the Skin
This is a shared conversation. Sign in to Orris to start your own chat.