Fibroadenoma Breast** - gross and microscopic features 2. Prognostic, Predictive factors in Carcinoma Breast 3. Classify Breast Tumours* 1. Breast Carcinoma* - classify*, Grading, Staging, Prognostic Factors; risk factors, Invasive Ductal Carcinoma answer in detail covering imp points as welll in exaam point of view 2mbbs pathology refer harsh moham add diagrams as well cover required points for muhs exam Add histo pathology diagram and gross as well FOR EXAM diagram draw
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is the complete, exam-oriented answer for MUHS 2nd MBBS Pathology (Robbins Cotran / Harsh Mohan framework):
BREAST PATHOLOGY - MUHS 2nd MBBS EXAM NOTES
Based on Robbins, Cotran & Kumar - Pathologic Basis of Disease
PART 1 - FIBROADENOMA OF THE BREAST ⭐⭐
Definition
Fibroadenoma is the most common benign tumor of the female breast. It is a biphasic tumor (contains both epithelial and stromal components) arising from the intralobular stroma.
Pathogenesis / Etiology
- Two-thirds harbor driver mutations in MED12 gene (encodes a subunit of the Mediator complex, which regulates RNA Polymerase II-dependent transcription)
- ~1/3 also harbor mutations in RARA (retinoic acid receptor alpha - an estrogen target gene)
- Hormonally responsive tumor - grows under estrogen influence
- Note: The same MED12 mutation is found in uterine leiomyomas - a useful exam fact
GROSS FEATURES
| Feature | Description |
|---|---|
| Size | Variable - <1 cm to replacing most of the breast |
| Shape | Well-circumscribed, rounded/lobulated |
| Consistency | Rubbery, firm |
| Colour | Gray-white |
| Cut surface | Bulges above surrounding tissue; contains slit-like spaces lined by epithelium |
| Capsule | Present (well-encapsulated) |
| Margins | Push surrounding tissue - NOT infiltrative |
Exam Tip: "Well-circumscribed rubbery gray-white nodule that BULGES above surrounding tissue with slit-like spaces" = Fibroadenoma gross
MICROSCOPIC FEATURES (Histopathology)
Two classic patterns:
1. Pericanalicular Pattern
- Delicate myxoid stroma surrounds patent (open) ducts
- Ducts remain round/oval
- Stroma proliferates around the ducts
2. Intracanalicular Pattern
- Stroma compresses and distorts ductal elements into cleft-like or slit-like spaces
- Epithelial-lined clefts are compressed
- More common
Stroma
- Delicate, often myxoid - resembles normal intralobular stroma
- In older females: stroma becomes densely hyalinized and epithelium becomes atrophic
Epithelium
- Two-layered: inner luminal cells + outer myoepithelial cells
- No atypia in benign fibroadenoma
DIAGRAM - FIBROADENOMA MICROSCOPY:
┌─────────────────────────────────────────┐
│ Pericanalicular: Intracanalicular: │
│ │
│ [Stroma]──┐ [Stroma]──────┐ │
│ ┌──O──┘ vs. ──[Slit]── │ │
│ │ DUCT compressed │ │
│ (round/oval) duct lumen │ │
└─────────────────────────────────────────┘
Clinical Features
- Age: 20s-30s (peak in reproductive age)
- Frequently multiple and bilateral
- Grow during pregnancy (may mimic carcinoma due to rapid growth)
- Regress after menopause
- Rare malignant transformation (<0.1%)
- Treatment: Excision (lumpectomy)
PART 2 - CLASSIFICATION OF BREAST TUMOURS ⭐⭐
WHO Classification of Breast Tumours
A. Epithelial Tumours
I. In Situ Carcinoma
- Ductal Carcinoma In Situ (DCIS)
- Comedo type (with central necrosis)
- Non-comedo type (cribriform, micropapillary, papillary, solid)
- Lobular Carcinoma In Situ (LCIS)
- Classic LCIS
- Pleomorphic LCIS
II. Invasive Carcinoma
- Invasive carcinoma of No Special Type (NST) - formerly Invasive Ductal Carcinoma (IDC) - 75% of all invasive carcinomas
- Invasive Lobular Carcinoma (ILC) - 10-15%
- Tubular Carcinoma
- Cribriform Carcinoma
- Mucinous (Colloid) Carcinoma
- Papillary Carcinoma
- Medullary Pattern Carcinoma (now classified as IDC-NST with medullary pattern)
- Metaplastic Carcinoma
- Inflammatory Carcinoma
B. Mesenchymal Tumours
- Fibroadenoma (most common benign)
- Phyllodes Tumor (benign/borderline/malignant)
- Angiosarcoma
- Myofibroblastoma
- Lipoma
- Fibromatosis
C. Nipple Tumours
- Paget's Disease of Nipple
- Nipple Adenoma
D. Lymphoma and Metastases
Classification Diagram - Breast Cancer
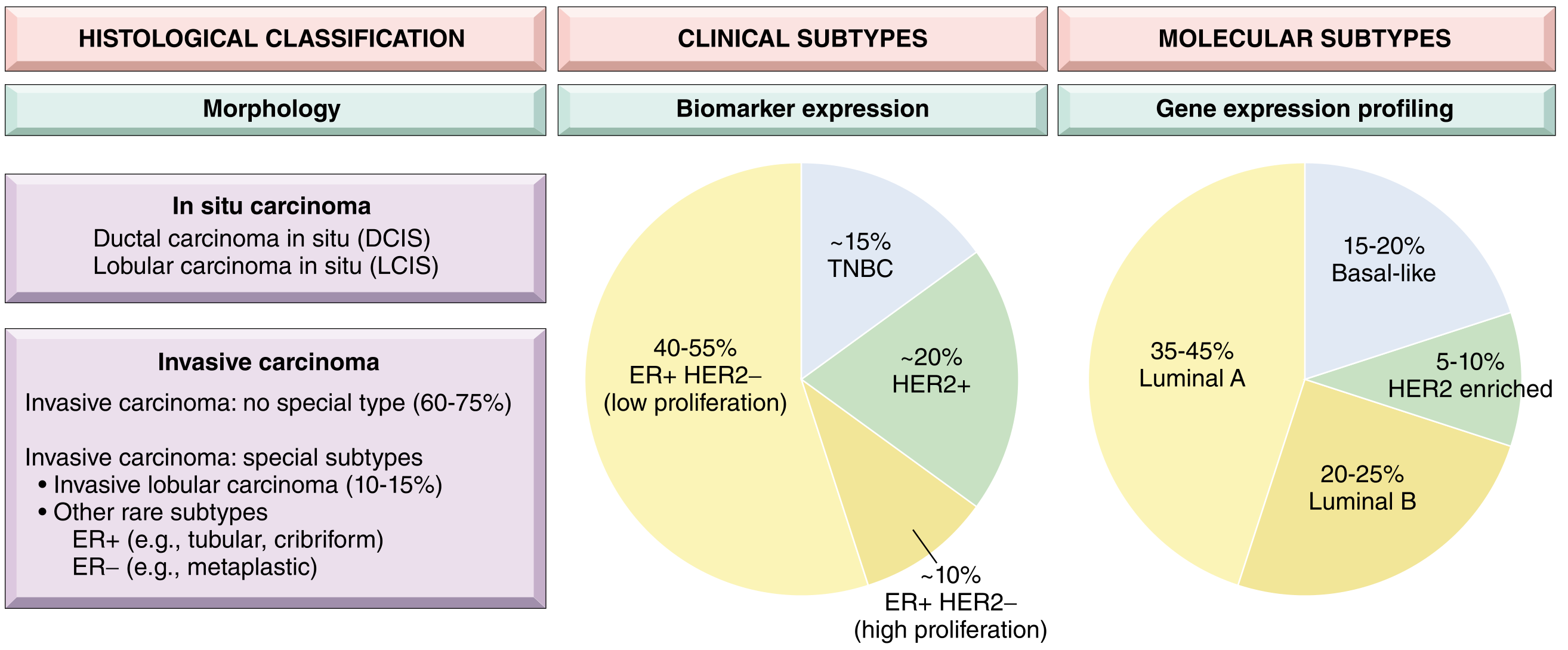
Fig: Breast Cancer Classification - Histological, Biomarker (Clinical), and Molecular Subtypes. Note that Luminal (ER+/HER2-) tumors make up 40-55% of all breast cancers.
Clinical/Biomarker Classification (Most Important for Exams)
| Clinical Subtype | ER | PR | HER2 | Molecular Subtype | % |
|---|---|---|---|---|---|
| Luminal (low proliferation) | + | +/- | - | Luminal A | 35-45% |
| Luminal (high proliferation) | + | +/- | - | Luminal B | 20-25% |
| HER2-positive | +/- | +/- | + | HER2-enriched | 5-10% / ~20% overall |
| Triple Negative (TNBC) | - | - | - | Basal-like | ~15% |
PART 3 - CARCINOMA BREAST (DETAILED) ⭐⭐⭐
Epidemiology
- Most common malignancy globally in females
- Surpassed lung cancer as most common cancer overall in 2020 (2.3 million new cases)
- Lifetime risk: 1 in 8 for females living to age 90 years (USA)
- 75% diagnosed after age 50
- Leading cause of cancer death in females worldwide
RISK FACTORS FOR BREAST CARCINOMA
High Risk (Relative Risk >4)
- Female sex (99% of cases)
- Increasing age
- Germline mutations - BRCA1 / BRCA2 (high penetrance)
- Strong family history (>1 first-degree relative, young age, multiple cancers)
- Personal history of breast cancer
- High breast density
Moderate Risk (Relative Risk 2.1-4.0)
- Germline mutations of moderate penetrance (PALB2, CHEK2, ATM)
- High-dose radiation to chest at young age (<18 years)
- Family history (1 first-degree relative)
Low Risk (Relative Risk 1.1-2.0)
- Early menarche (age <12 years)
- Late menopause (age >55 years)
- Late first pregnancy (age >35 years)
- Nulliparity
- Absence of breastfeeding
- Exogenous hormone therapy (OCP, HRT)
- Postmenopausal obesity
- Physical inactivity
- High alcohol consumption
Protective Factors
- Early pregnancy (<20 years)
- Prolonged breastfeeding
- Bilateral prophylactic mastectomy (reduces risk by ~90%)
- ER antagonists (chemoprevention in high-risk patients)
Exam Mnemonic for Hormonal Risk Factors: "NEON-M" - Nulliparity, Early menarche, Obesity (postmenopausal), No breastfeeding, Menopause (late)
BRCA Genes
- BRCA1 (chromosome 17q) - associated with TNBC/basal-like tumors; also increases risk of ovarian cancer
- BRCA2 (chromosome 13q) - associated with luminal tumors; also increases risk of male breast cancer
- Women with BRCA mutations have up to 80% lifetime risk of breast cancer
PATHOGENESIS
Two pathways:
LOW-GRADE PATHWAY: HIGH-GRADE PATHWAY:
Columnar cell lesions High-grade DCIS
↓ ↓
Flat epithelial atypia High-grade invasive
↓ carcinoma (HER2+, TNBC)
Atypical hyperplasia
↓ Genetics: Loss 13q,
Low-grade DCIS/LCIS gain 11q13, 17q12
↓ amplification
Low-grade ER+ invasive Ca
(Luminal A/B)
Genetics: Loss 16q, gain 1q
CLASSIFICATION OF BREAST CARCINOMA (Exam Format)
A. In Situ Carcinomas
1. Ductal Carcinoma In Situ (DCIS)
- Most common type of in situ carcinoma
- Confined within ducts, basement membrane intact
- Detected by mammography as calcifications
- Subtypes:
- Comedo type (most aggressive): Necrotic center + calcification; high-grade nuclei; HER2 amplification
- Non-comedo: Cribriform, micropapillary, solid, papillary
2. Lobular Carcinoma In Situ (LCIS)
- Marker of increased risk + precursor lesion
- Loss of E-cadherin expression (key feature)
- Small loosely cohesive cells filling lobular acini
- When carcinoma develops in LCIS patients: 2/3 in same breast, 1/3 contralateral
- Management: Bilateral risk-reduction strategies
B. Invasive (Infiltrating) Carcinomas
1. Invasive Carcinoma of No Special Type (IDC - NST) - 75%
(See detailed section below)
2. Invasive Lobular Carcinoma (10-15%)
- Loss of E-cadherin - cells are dyscohesive
- Indian-file / single-file pattern of infiltration
- Contains signet ring cells (intracytoplasmic mucin)
- Minimal desmoplasia - difficult to detect on imaging
- Metastasizes to: peritoneum, retroperitoneum, leptomeninges, GI tract, ovaries, uterus
3. Mucinous (Colloid) Carcinoma
- Soft, rubbery, gelatinous with pushing/circumscribed borders
- Tumor cells in pools of extracellular mucin
- Good prognosis - ER+
4. Tubular Carcinoma
- Well-differentiated; small angulated tubules
- Excellent prognosis; ER+
5. Medullary Pattern Carcinoma
- Previously called Medullary carcinoma; now IDC-NST with "medullary pattern"
- Large pleomorphic cells, prominent TILs (tumor infiltrating lymphocytes), solid growth
- Often TNBC
6. Paget's Disease of Nipple
- Large, pale cells (Paget cells) in nipple epidermis
- Always associated with underlying DCIS or invasive carcinoma
- Presents as eczema-like rash of nipple
7. Inflammatory Breast Carcinoma
- Rapid onset, skin erythema, warmth, edema ("peau d'orange" without a palpable mass)
- Due to dermal lymphatic invasion by tumor emboli
- Very poor prognosis (Stage IIIB)
PART 4 - INVASIVE DUCTAL CARCINOMA (IDC) - DETAILED ⭐⭐⭐
Definition
Invasive (Infiltrating) Ductal Carcinoma - No Special Type (IDC-NST) is the most common invasive breast carcinoma, accounting for approximately 75% of all invasive breast carcinomas. It represents a heterogeneous group of tumors that do not fit any specific special histological subtype.
GROSS FEATURES of IDC
| Feature | Description |
|---|---|
| Size | Usually 2-3 cm at presentation (without screening) |
| Shape | Irregular, stellate (star-shaped) margins |
| Consistency | Hard, stony (scirrhous) |
| Cut surface | Gritty sensation when cut/scraped - characteristic grating sound |
| Color | Chalky-white streaks (desmoplastic stroma) + foci of calcification |
| Borders | Irregular, infiltrating (NOT well-circumscribed) |
| Skin changes | Skin dimpling/retraction in central tumors; nipple retraction |
GROSS DIAGRAM OF IDC:
Skin dimpling
↓
___________
/ Irregular/
/ stellate \ ← Spiculated margins
| HARD mass |
\ GRITTY / ← Chalky-white streaks
\___(Ca)___/ (desmoplastic stroma)
|
Chest wall
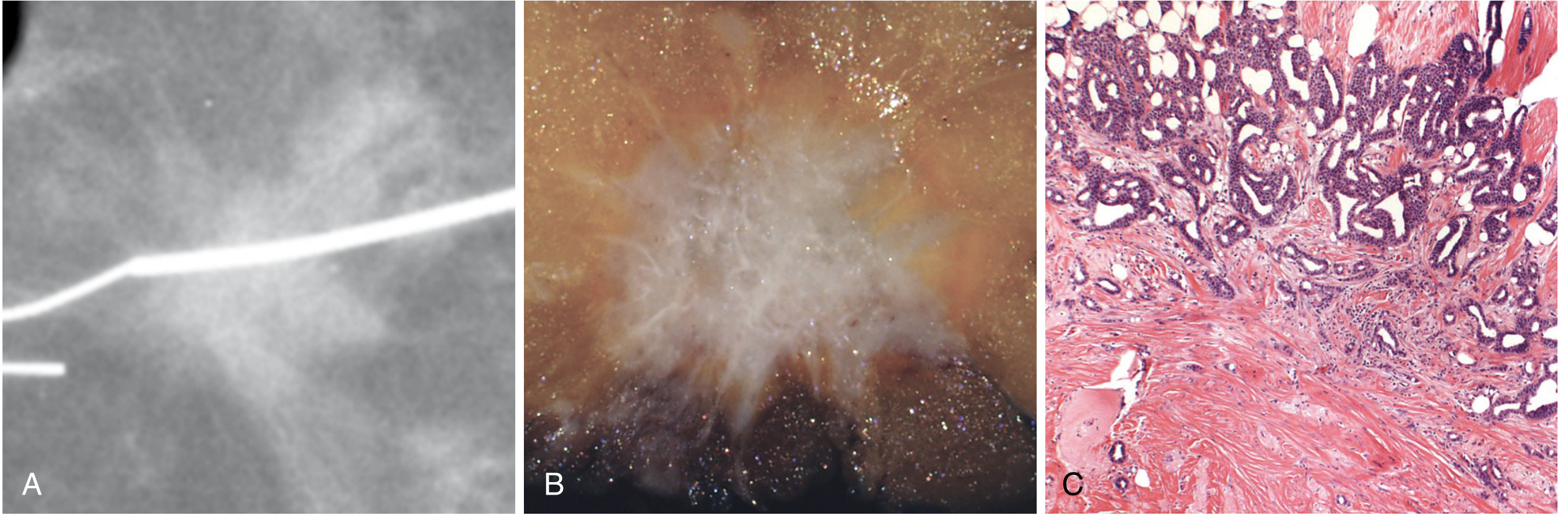
Fig 23.20 - Robbins: Invasive breast carcinoma of no special type. (A) Mammogram: irregular radiodense mass with spiculated margins. (B) Gross: irregular hard mass. (C) Histology: exuberant desmoplastic stromal response.
MICROSCOPIC FEATURES (Histopathology) of IDC
Key Microscopic Findings:
- Invasive nests, cords, tubules, or sheets of tumor cells infiltrating fibrous stroma
- Desmoplastic stromal reaction - dense fibrous stroma surrounding tumor cell nests (hallmark)
- No organized ductal/lobular architecture
- Variable nuclear pleomorphism depending on grade
- Mitotic figures present
- Calcifications may be present
- Some tumors have TILs (tumor infiltrating lymphocytes) - especially TNBC
GRADING OF BREAST CARCINOMA - Nottingham Histologic Score (Elston-Ellis Modification of Bloom-Richardson) ⭐⭐⭐
This is the most important grading system - tested frequently in MUHS exams.
Three Parameters (Each scored 1-3):
| Parameter | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| 1. Tubule Formation | >75% of tumor forms tubules | 10-75% tubule formation | <10% tubule formation |
| 2. Nuclear Pleomorphism | Small, regular, uniform nuclei | Moderate increase in size/variability | Marked variation in size, shape, nucleoli |
| 3. Mitotic Count | Low (1-2 per HPF) | Intermediate (3-4 per HPF) | High (≥5 per HPF) |
Total Score Interpretation:
- 3-5 = Grade 1 (Well differentiated) - Good prognosis
- 6-7 = Grade 2 (Moderately differentiated) - Intermediate prognosis
- 8-9 = Grade 3 (Poorly differentiated) - Poor prognosis
GRADING DIAGRAM:
Grade 1: Grade 2: Grade 3:
┌──────────┐ ┌──────────┐ ┌──────────┐
│ O O O │ │ O Clust │ │ ████████ │
│ Tubules │ vs │ Clusters │ vs │ Solid │
│ uniform │ │ some │ │ sheets, │
│ nuclei │ │ atypia │ │ necrosis │
└──────────┘ └──────────┘ └──────────┘
Score 3-5 Score 6-7 Score 8-9
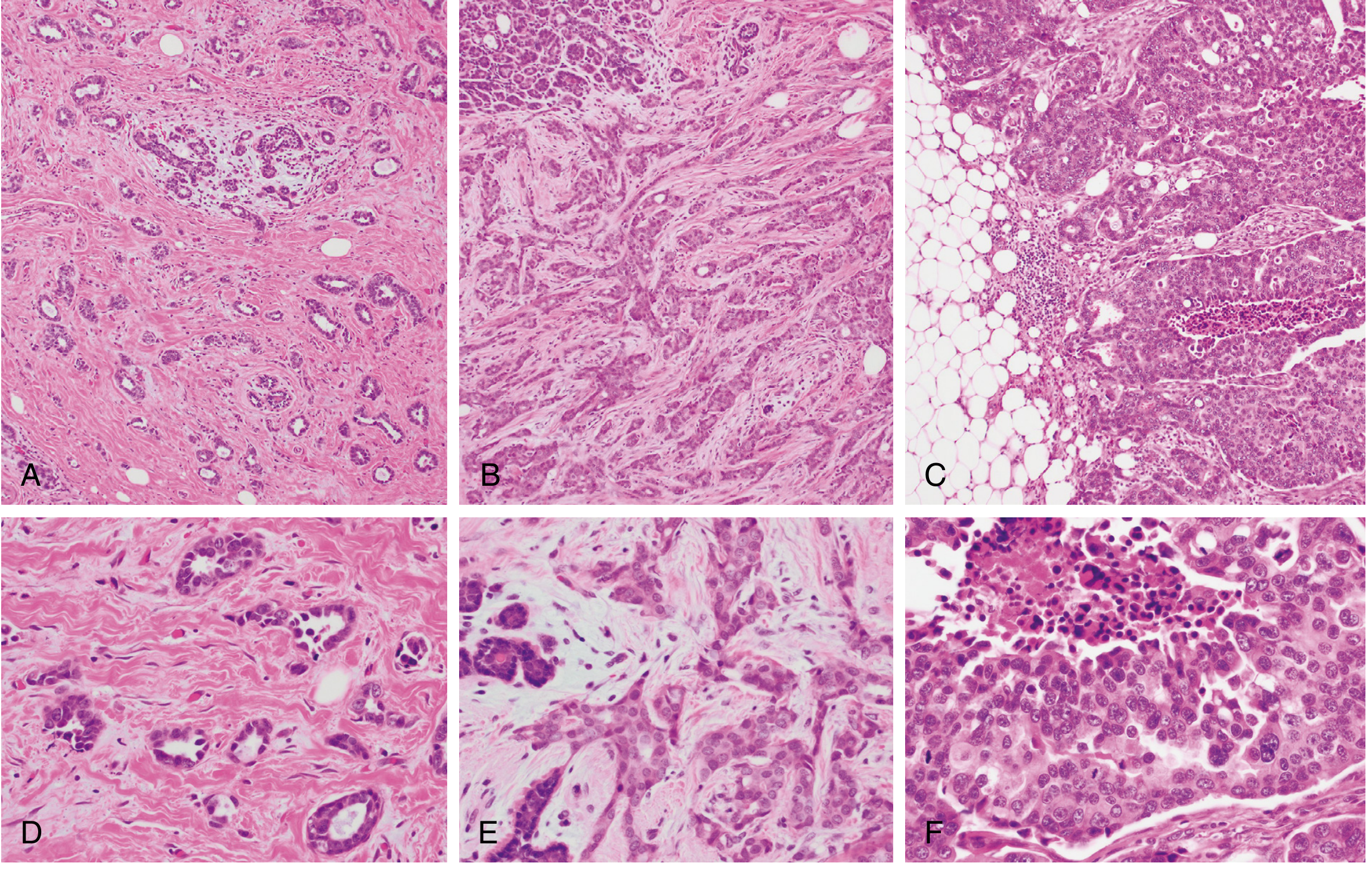
Fig 23.21 - Robbins: Invasive breast carcinoma grading. (A,D) Grade 1: tubule formation, small monomorphic nuclei, rare mitoses. (B,E) Grade 2: less tubule formation, solid nests, pleomorphic nuclei, occasional mitoses. (C,F) Grade 3: ragged sheets, enlarged pleomorphic nuclei, tumor necrosis, high mitotic rate.
STAGING OF BREAST CARCINOMA - TNM System (AJCC 8th Edition) ⭐⭐⭐
TNM Categories:
- T = Primary Tumor size
- Tis = In situ (DCIS/LCIS)
- T1 = ≤2 cm
- T2 = >2 cm but ≤5 cm
- T3 = >5 cm
- T4 = Any size with skin/chest wall involvement or inflammatory carcinoma
- N = Regional Lymph Nodes
- N0 = No metastasis
- N1 = 1-3 positive axillary nodes
- N2 = 4-9 positive nodes
- N3 = ≥10 positive nodes
- M = Distant Metastasis
- M0 = Absent
- M1 = Present
Stage Groups and Prognosis:
| Stage | T | N | M | 10-Year Survival |
|---|---|---|---|---|
| 0 | Tis (DCIS) | N0 | M0 | 97% |
| I | ≤2 cm | N0 or micromet | M0 | 87% |
| II | >2 cm or 2-5 cm | 1-3 nodes or 0-3 nodes | M0 | 65% |
| III | >5 cm / any + skin/chest wall / inflammatory | Variable | M0 | 40% |
| IV | Any | Any | M1 | 5% |
AJCC 8th Edition Update: The current staging also incorporates Grade + ER + PR + HER2 status to assign a PROGNOSTIC STAGE that may differ from the anatomic stage. For example, a TNBC may be "up-staged" because of its aggressive biology.
PART 5 - PROGNOSTIC AND PREDICTIVE FACTORS ⭐⭐⭐
Key Definitions
- Prognostic factor: Indicates likely outcome (survival, recurrence) independent of therapy
- Predictive factor: Indicates likely response to specific treatment
- Note: Tumor biology factors (ER, HER2) are BOTH prognostic AND predictive; tumor extent factors (size, nodes) are primarily PROGNOSTIC
MAJOR PROGNOSTIC FACTORS (In order of importance)
1. Distant Metastases (Most Important Overall)
- Once present, cure is unlikely
- Palliation still possible in ER+ and HER2+ tumors
- Common sites: bone, lung, liver, brain
2. Axillary Lymph Node Status (Most Important in Absence of Distant Mets)
| Nodal Status | 10-Year Disease-Free Survival |
|---|---|
| No positive nodes | 70-80% |
| 1-3 positive nodes | 35-40% |
| >10 positive nodes | 10-15% |
- Sentinel lymph node biopsy: identifies first draining node with radiotracer/blue dye
- If sentinel node negative - no full axillary dissection needed
3. Tumor Size
- Smaller tumors = better prognosis
- Tumors ≤1 cm with no node involvement = excellent prognosis
4. Histologic Grade
- Grade 1 (well diff.) > Grade 2 > Grade 3 (poorly diff.) in terms of prognosis
5. Molecular/Biomarker Factors
ER (Estrogen Receptor)
- Prognostic + Predictive
- ER+ (≥1% nuclear staining) responds to endocrine therapy (Tamoxifen, Aromatase Inhibitors)
- Low ER (1-10%) = worse prognosis than high ER expression
PR (Progesterone Receptor)
- ER+/PR+ = best outcome
- ER+ but PR-low = worse outcome
HER2 (Human Epidermal Growth Factor Receptor 2)
- Prognostic + Predictive
- HER2 positivity = aggressive behavior
- Responds to HER2-targeting agents: Trastuzumab (Herceptin), Pertuzumab, T-DM1
- Assessed by IHC (3+ = positive) or FISH (gene amplification)
6. Molecular Subtype
| Subtype | Prognosis |
|---|---|
| Luminal A (ER+/PR+/HER2-/low Ki67) | Best |
| Luminal B (ER+, high proliferation) | Intermediate-Good |
| HER2-enriched | Intermediate (improved with targeted therapy) |
| Triple Negative (TNBC) | Worst (no targeted therapy available for most) |
7. Tumor Infiltrating Lymphocytes (TILs)
- Prominent TILs = better prognosis and better response to neoadjuvant chemotherapy
- Especially important in HER2+ and TNBC
8. Proliferation Rate (Ki-67)
- Low Ki-67 = slower growing = better prognosis
- High Ki-67 = high-grade, aggressive
9. Gene Expression Profiling
- Oncotype DX, MammaPrint, Prosigna
- Used mainly to identify ER+/HER2- patients who can safely avoid chemotherapy
10. Response to Neoadjuvant Chemotherapy
- Pathologic Complete Response (pCR) = no residual invasive disease after pre-surgery chemo
- pCR in TNBC and HER2+ = significantly better prognosis
Recurrence Patterns by Molecular Subtype
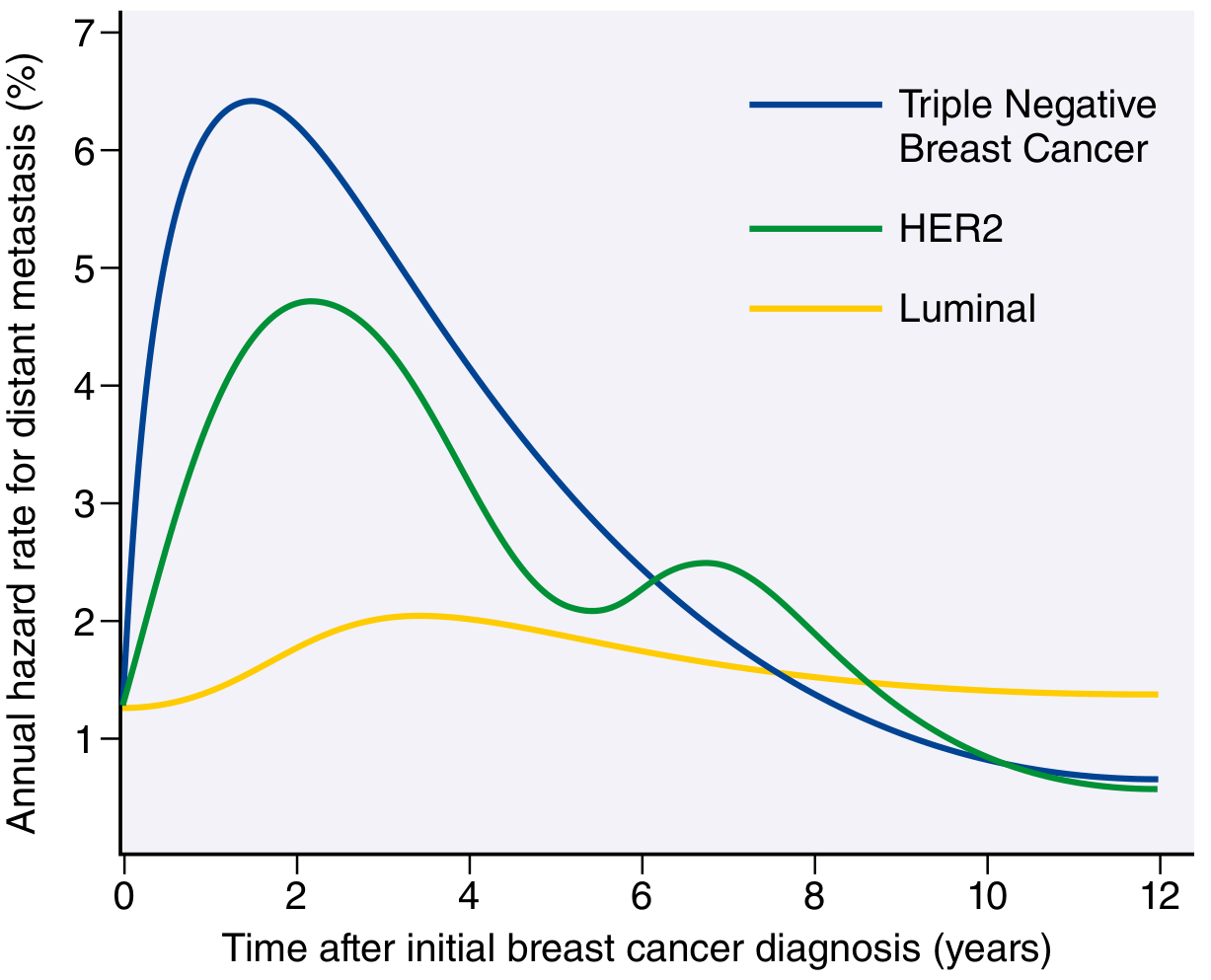
Fig 23.23 - Robbins: Recurrence patterns by subtype. TNBC has highest early recurrence (peaks 1-2 years), mostly resolves by 8 years. HER2+ shows bimodal pattern. Luminal (ER+) has lowest early recurrence but continues recurring for many years (late recurrences due to tumor dormancy).
PREDICTIVE FACTORS (Summary)
| Treatment | Predictive Biomarker |
|---|---|
| Endocrine therapy (Tamoxifen/AIs) | ER positivity |
| Trastuzumab (Herceptin) | HER2 overexpression/amplification |
| PARP inhibitors (Olaparib) | Germline BRCA1/BRCA2 mutation |
| PI3K inhibitors (Alpelisib) | PIK3CA mutation |
| Immune checkpoint inhibitors | PD-L1 expression, TMB, MSI |
| TRK inhibitors | NTRK gene fusion |
QUICK SUMMARY TABLE FOR MUHS EXAM
| Feature | Fibroadenoma | IDC (NST) |
|---|---|---|
| Nature | Benign biphasic tumor | Malignant epithelial tumor |
| Age | 20-30s | >40 years |
| Gross | Well-circumscribed, rubbery, gray-white, slit-like spaces | Hard, scirrhous, stellate, irregular margins |
| Micro | Pericanalicular/intracanalicular patterns; myxoid stroma; no atypia | Invasive cords/sheets, desmoplastic stroma, nuclear pleomorphism |
| Hormones | Grows in pregnancy; regresses at menopause | Risk ↑ with prolonged estrogen exposure |
| Mutation | MED12, RARA | TP53, PIK3CA, BRCA (germline) |
| Prognosis | Excellent | Depends on stage and molecular subtype |
IMPORTANT EXAM DIAGRAMS - DRAWN
Diagram 1: IDC Histopathology Schema
LOW POWER (IDC - Scirrhous type): HIGH POWER:
Fat Tumor nests Nuclear pleomorphism
O ╔══╗ ╔═╗ Large irregular
O ══╪══╪══╪═╪══ Dense fibrous nuclei, prominent
O ╚══╝ ╚═╝ stroma nucleoli
↑ Invasive (desmoplasia)
tumor clusters Mitotic figures:
│ │
Lymphatics (⊗)← Mitosis
invaded──→ ══
(LVI) Gland formation:
minimal (Grade 3)
Diagram 2: Fibroadenoma Histopathology
PERICANALICULAR: INTRACANALICULAR:
~Stroma~Stroma~ ~~Stroma~~
~~( O )~~( O )~~ vs. ~~[ ─ ]~~
~Stroma~Stroma~ ~~[cleft]~~
~~( O )~~( O )~~ ~~Stroma~~
Round patent ducts Compressed slit-like
surrounded by stroma epithelial spaces
(CLEFTS)
Stroma: Myxoid/loose
Diagram 3: DCIS Types
COMEDO DCIS: CRIBRIFORM DCIS:
┌──────────────┐ ┌──────────────┐
│▓▓▓Necrosis▓▓▓│ │ ○ ○ ○ ○ ○ │
│▓(calcific.)▓▓│ │○ ○ Sieve- ○ │
│ High-grade │ │ like holes │
│ nuclei ring │ │ Low-grade │
└──────────────┘ └──────────────┘
Most aggressive Good prognosis
HER2 amplification ER+
ONE-LINERS FOR VIVA / SHORT ANSWERS
- Most common benign tumor of breast = Fibroadenoma
- Most common malignant tumor of breast = IDC-NST (Invasive ductal carcinoma)
- Grading system used = Nottingham Histologic Score (Bloom-Richardson modified by Elston & Ellis)
- Three parameters of Nottingham grading = Tubule formation + Nuclear pleomorphism + Mitotic count
- Sentinel node biopsy uses = Radiotracer or blue dye
- Most important prognostic factor overall = Distant metastases
- Most important prognostic factor in absence of mets = Axillary lymph node status
- Loss of E-cadherin = Invasive lobular carcinoma / LCIS
- Indian file pattern = Invasive lobular carcinoma
- Skin dimpling in breast cancer = Cooper's ligament involvement by tumor fibrosis
- Paget cells = Large pale cells in nipple epidermis, always indicating underlying carcinoma
- ER+ breast cancer responds to = Tamoxifen (premenopausal), Aromatase Inhibitors (postmenopausal)
- HER2+ responds to = Trastuzumab (Herceptin)
- TNBC = ER-, PR-, HER2- ; associated with BRCA1 mutation, basal-like subtype
- Fibroadenoma mutation = MED12 (same as uterine leiomyoma)
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.), pp. 971-985
This is a shared conversation. Sign in to Orris to start your own chat.