I want to know the prognosis and course of illness of bipolar mood disorder…good and bad prognostic factors, what if the episodes are not treated what happens further, what if they are partially treated then what happens and what if they are fully treated…how will treatment change the life and course of illness
"bipolar disorder" AND prognosis AND course
PMID: 40426301
Prognosis and Course of Illness in Bipolar Mood Disorder
Overview
Natural Course (Untreated)
Episode Duration
Episode Recurrence
Acceleration Over Time - The Kindling Effect
"As the disorder progresses, the time between episodes often decreases."
- Kaplan & Sadock's Synopsis of Psychiatry
- Early in the illness, episodes are often triggered by identifiable stressors (life events, sleep disruption)
- With each successive episode, the threshold for triggering the next episode lowers - this is called kindling or sensitization
- Over time, episodes begin occurring with less provocation, sometimes spontaneously
- After approximately five episodes, the interepisode interval stabilizes at around 6 to 9 months
- 5 to 15% of patients with untreated or poorly controlled bipolar disorder develop rapid cycling (4 or more episodes per year)
Long-Term Outcomes Without Treatment
| Outcome | Proportion |
|---|---|
| No recurrence (7%) | Very rare |
| Well but multiple relapses | 45% |
| Partial remission only | 30% |
| Chronically ill | 10% |
| Significant social decline | 1 in 3 |
- On average, patients experience 9 manic episodes across their lifetime
- 40% of all patients have more than 10 episodes
- One-third of all bipolar I patients develop chronic symptoms and measurable social decline (loss of job, relationships, independence)
Prognostic Factors
Good Prognostic Factors
- Short duration of manic episodes
- Later (advanced) age of onset
- Few suicidal thoughts
- Few coexisting psychiatric or medical problems
- Good premorbid occupational functioning
- Strong social support
Poor Prognostic Factors
- Poor premorbid occupational status
- Alcohol or substance use disorder (comorbid SUD roughly doubles lifetime risk - 61% of bipolar I patients have lifetime SUD vs. 27% in unipolar depression)
- Psychotic features during episodes
- Depressive features predominating (mixed states)
- Interepisode depressive symptoms (residual depression between episodes)
- Male gender (men tend to have more manic episodes; women more depressive/mixed)
- Comorbid anxiety disorders
- Early age of onset (childhood/adolescent onset carries worse long-term prognosis)
- Rapid cycling pattern
- Poor treatment adherence
What Happens with Each Scenario
1. No Treatment at All
- Episodes are longer and more severe
- Each episode causes neurobiological changes that lower the threshold for the next one (kindling)
- Episodes become more frequent and eventually more autonomous (less stress-dependent)
- Rapid cycling develops in a significant minority
- Cumulative cognitive impairment, especially memory and executive function
- Social decline: job loss, broken relationships, financial ruin, legal problems
- Suicide risk is high: lifetime suicide attempt rate in bipolar disorder is 25-50%; completed suicide occurs in approximately 15% of untreated/undertreated patients
- Significant periods of hospitalization accumulate
2. Partial Treatment (Irregular or Inadequate)
- Episodes still recur, but may be somewhat attenuated in severity
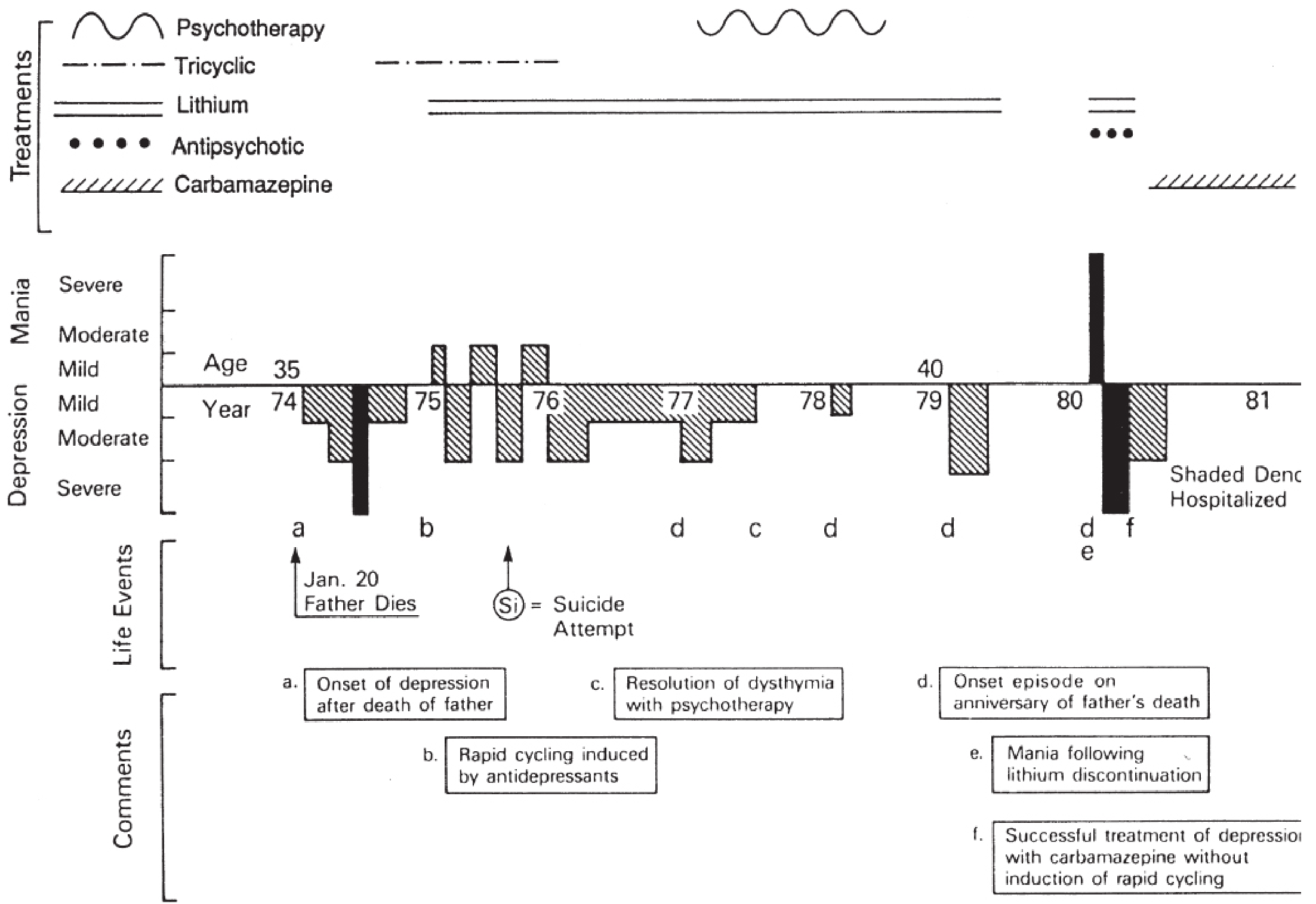
- Stopping lithium abruptly is particularly dangerous - it is associated with a rebound mania that is often worse than the original episode (as shown in the life chart above, point "e")
- The kindling process continues - each breakthrough episode further sensitizes the brain
- Antidepressants used without a mood stabilizer can induce rapid cycling (as shown in the life chart, point "b")
- Partial response leads to residual symptoms between episodes, which are themselves a poor prognostic marker
- Functional impairment (work, relationships) continues to accumulate even when episodes are "incomplete"
- The window for optimal treatment response narrows with each successive episode
- More depressive episodes
- Higher number of suicide attempts
- Earlier age of onset
- Longer total illness duration
- Greater probability of a Bipolar II diagnosis
3. Full, Adequate, Continuous Treatment
- Lithium prophylaxis is the best-studied intervention. It reduces episode frequency and severity - however, only 50 to 60% of patients achieve significant symptom control with lithium alone, highlighting that full treatment still requires persistence and often combination strategies
- About 40 to 50% of patients have a second episode within 2 years even with treatment - but the gap without treatment would be shorter and episodes more severe
- Only 7% of patients have no recurrence at all (with or without treatment - this represents the naturally good-outcome group)
- On long-term follow-up with treatment, 15% are entirely well, and another 45% are well but with occasional relapses - that is 60% achieving good functional outcomes
- Suicide risk drops markedly; lithium in particular has a specific anti-suicidal effect beyond just mood stabilization
- Cognitive decline is slowed or prevented
- Occupational and social functioning is preserved
- Hospitalizations become fewer and shorter
- Psychotherapy (CBT, family therapy, psychoeducation) as an adjunct to medication improves adherence, reduces relapse rates, and helps patients recognize prodromal symptoms early
Bipolar II: A Note on Course
Summary Table
| Scenario | Episode Frequency | Severity | Functional Impact | Suicide Risk | Long-term |
|---|---|---|---|---|---|
| No treatment | Increasing, kindling | Worsening | Severe decline | Very high | Chronic deterioration |
| Partial treatment | Still recurrent | Moderate | Ongoing impairment | Elevated | Gradual decline |
| Full treatment | Reduced, stable | Attenuated | Preserved function | Significantly reduced | 60% achieve good outcome |
- Kaplan & Sadock's Synopsis of Psychiatry - COURSE and PROGNOSIS sections, pp. 1148-1150
- Mena SA et al., "Impact of Duration of Untreated Bipolar Disorder on Clinical Outcomes: A Systematic Review." Early Intervention in Psychiatry, 2025. PMID 40426301
Can you give me indian and nice guidelines of for how long the medications should be continued based on number and types of episodes
NICE guidelines bipolar disorder maintenance treatment duration how long medications episodes 2024
Indian psychiatric society bipolar disorder treatment guidelines maintenance duration number of episodes 2023 2024
https://pmc.ncbi.nlm.nih.gov/articles/PMC12900052
https://pmc.ncbi.nlm.nih.gov/articles/PMC12900052
https://www.nice.org.uk/guidance/cg185/chapter/1-recommendat…
NICE CG185 bipolar disorder 1.7.8 1.7.9 1.7.10 1.7.11 long term treatment duration years stop medication
Indian psychiatric society bipolar disorder CPG 2024 2025 maintenance treatment first episode two episodes lifetime prophylaxis duration years
Maintenance Treatment Duration in Bipolar Disorder: Indian & NICE Guidelines
Understanding the Phases First
| Phase | Starts when | Goal | Duration |
|---|---|---|---|
| Acute | Episode begins | Resolve the episode | Weeks |
| Continuation | Acute episode remits | Prevent relapse of the SAME episode | Up to 6 months |
| Maintenance | After continuation phase | Prevent NEW episodes (recurrence) | Months to lifetime |
NICE CG185 Guidance on Maintenance Duration
After an Episode of Mania
- Within 4 weeks of resolution, discuss whether to continue treatment for mania or move to long-term treatment
- If the person decides to continue mania treatment only (not full long-term): offer it for a further 3-6 months, then review (NICE 1.5.14-1.5.15)
After an Episode of Bipolar Depression
- Within 4 weeks of resolution, discuss whether to continue or start long-term treatment
- If they choose to continue only the depression treatment: offer it for a further 3-6 months, then review (NICE 1.6.11-1.6.12)
Long-Term (Maintenance) Treatment
- Offer lithium as first-line long-term pharmacological treatment (NICE 1.7.7)
- Long-term treatment decisions should be guided by: severity and frequency of episodes, associated risks, symptoms between episodes, and previous treatment response (NICE 1.7.1)
- NICE does not prescribe a fixed number of years - it recommends ongoing review as a shared decision
When Stopping Long-Term Treatment (NICE 1.7.11)
- Discuss how to recognize early signs of relapse
- Stop treatment gradually (not abruptly - this is especially important for lithium)
- Monitor closely during tapering
After Stopping
- Continue monitoring symptoms, mood and mental state for 2 years after medication has stopped entirely (NICE 1.7.12)
- This may be done in primary care
IPS (Indian Psychiatric Society) 2025 CPG Guidelines
General Maintenance Principle
"Even where indications for life-long prophylaxis are not prominent, maintenance treatment should be continued for at least 12-18 months after stabilization of a manic episode, with further continuation depending on a discussion with the patient and family, and continued risk-benefit analysis."
- IPS CPG 2025
Episode-Count-Based Guidance
| Number / Type of Episode | IPS Recommendation |
|---|---|
| First manic episode - no risk factors | Minimum 12-18 months maintenance; individualized decision to stop thereafter |
| First manic episode with any of the following: severe episode, required hospitalization, psychotic features, positive family history of BD, significant social/occupational implications of another relapse | Strongly recommend starting long-term maintenance treatment |
| Two or more episodes | Long-term maintenance strongly indicated; continuation beyond 2 years is standard |
| Multiple recurrences / frequent relapses | Life-long prophylaxis is indicated |
| Rapid cycling (4+ episodes/year) | Long-term / lifelong treatment; lithium + valproate or add-on atypical antipsychotic |
Critical Indian Data Point
"An Indian study found that 80% of patients who underwent planned discontinuation of lithium, following extended periods of maintenance treatment and clinical euthymia, had relapsed within 10 months of discontinuation."
- IPS CPG 2025
When Discontinuing (IPS)
- Any discontinuation must be under clinician supervision
- Taper in small steps with close monitoring
- Provide education on early warning signs of relapse
- Prepare contingency plans
- Ensure clinician accessibility during the process
- Defer discontinuation if significant life events or stressors are anticipated
The Classic Episode-Based Framework (Widely Used in Teaching)
| Number of Episodes | Recommended Maintenance Duration |
|---|---|
| 1st episode (uncomplicated) | At least 1-2 years after remission |
| 1st episode (with severity markers*) | At least 2-5 years, possibly longer |
| 2nd episode | At least 2-5 years |
| 3rd episode or more | Lifelong / indefinite maintenance |
| Any episode with: severe mania, psychosis, suicide attempt, rapid cycling, strong family history | Consider lifelong from the outset |
Practical Points - Both Guidelines Agree On
- Lithium is the gold standard for long-term maintenance - it has the best evidence and a proven anti-suicidal effect
- Never stop abruptly - particularly lithium; abrupt discontinuation triggers rebound mania worse than the original
- Stopping treatment is high-risk - 80-90% of patients relapse after discontinuation
- Maintenance treatment should be reviewed regularly, not maintained blindly; dose adjustment and monitoring (renal, thyroid, metabolic) are ongoing
- Psychotherapy and psychoeducation should accompany pharmacotherapy throughout
- Comorbidities (substance use, anxiety) must be treated concurrently - they independently worsen prognosis regardless of mood stabilizer adherence
- The decision to stop is always individualized - age, severity of past episodes, occupational/social risk, patient preference, and side effect burden all factor in
Sources
- IPS CPG 2025 - Bipolar Disorder (PMC12900052) - Indian Psychiatric Society
- NICE CG185 - Bipolar Disorder: Assessment and Management (last updated September 2025)
- The Maudsley Prescribing Guidelines in Psychiatry, 15th Edition - Prophylaxis in Bipolar Disorder chapter