Hypoplastic left heart syndrome at 16 weeks
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypoplastic left heart syndrome" AND "prenatal diagnosis"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive information to give a thorough answer. Here is everything synthesized:
Hypoplastic Left Heart Syndrome (HLHS) at 16 Weeks
Definition and Anatomy
HLHS is a spectrum of congenital heart disease involving underdevelopment of the entire left side of the heart - the mitral valve, left ventricular (LV) cavity, LV outflow tract, aortic valve, ascending aorta, and aortic arch. The left ventricle is functionally insufficient to sustain systemic cardiac output. In the classic and most severe form (mitral atresia + aortic atresia), there is effectively no left heart inflow or outflow.
- Creasy & Resnik's Maternal-Fetal Medicine, p.469
- The Developing Human: Clinically Oriented Embryology, p.848
Pathophysiology
In fetal life, the right ventricle (RV) maintains both circulations simultaneously. Pulmonary venous return reaches the left atrium but cannot exit forward through the atretic mitral valve; it must shunt left-to-right across the foramen ovale (FO) into the RA, where it mixes with systemic venous return. The RV then ejects combined output into the pulmonary artery. The aorta is perfused in a retrograde direction via the patent ductus arteriosus (PDA). The hypoplastic ascending aorta carries only coronary and cerebral blood in reverse.
At birth, survival depends on two things:
- PDA patency - for systemic blood flow (the newborn is "ductal dependent")
- Unobstructed FO - for left atrial decompression
Fuster & Hurst's The Heart, 15th Edition, p.2034
Detection at 16 Weeks
HLHS can be detected as early as the first trimester in some cases. By 16 weeks, the following features are identifiable on fetal echocardiography:
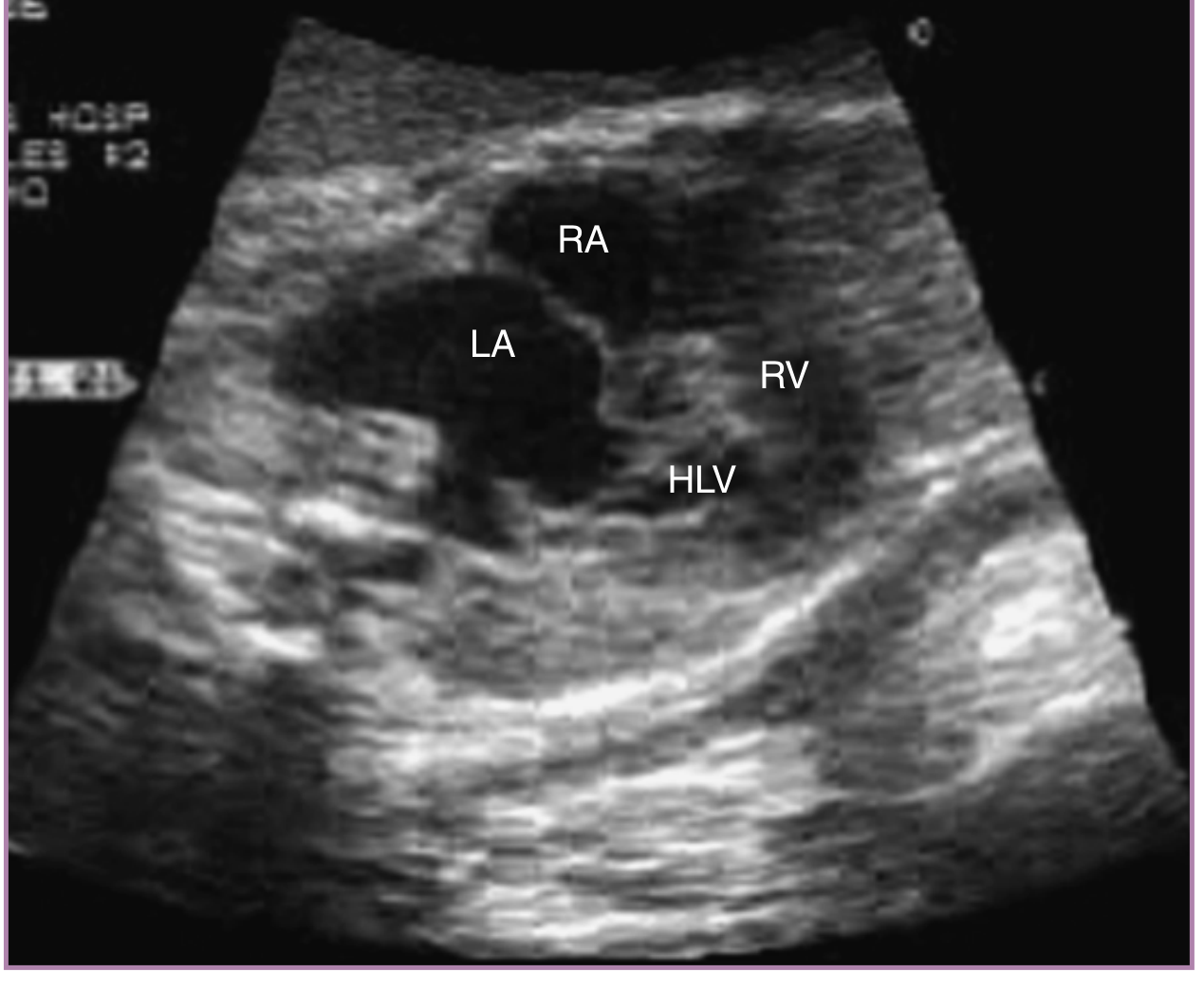
Four-chamber view (4CV) abnormalities:
- Markedly asymmetric cardiac chambers - the RV dominates, the LV is tiny or slit-like
- No identifiable mitral valve inflow (in atresia) or a small, restricted mitral valve
- The LV endocardium may appear bright (endocardial fibroelastosis, EFE) from elevated pressure
- Intact ventricular septum (in classic mitral + aortic atresia)
Outflow tract views:
- Aortic root is markedly small or atretic
- Retrograde flow in the transverse aortic arch on color Doppler (filling from the PDA back toward the head and coronaries)
Foramen ovale assessment:
- Restrictive FO (bowing of the septum toward the RA, thickened atrial septum, reversed or blunted spectral Doppler) is a critical negative prognostic finding
- A restrictive or intact FO causes left atrial hypertension → pulmonary venous congestion → pulmonary vascular disease (irreversible if prolonged)
Important caveat at 16 weeks: Some forms of HLHS evolve during fetal life. Severe aortic stenosis at 16-18 weeks may cause a dilated, dysfunctional LV that progresses to HLHS by term. A relatively formed LV at midgestation in the setting of mitral/aortic stenosis does NOT rule out HLHS at birth. Serial monitoring is mandatory. - Creasy & Resnik's MFM, p.469-470
Associated Abnormalities
- Aneuploidy risk: increased - genetic counseling and chromosomal microarray (or amniocentesis/CVS) should be offered
- CNS abnormalities: increased risk for congenital or acquired central nervous system anomalies
- Gene mutations: complex polygenic/multifactorial inheritance; neural crest cell migration disturbances are implicated in pathogenesis - The Developing Human, p.848
Prenatal Management
| Step | Action |
|---|---|
| Referral | Fetal echocardiography at a tertiary MFM/pediatric cardiology center |
| Genetic workup | Chromosomal microarray; consider CVS or amniocentesis if not done |
| FO surveillance | Serial Doppler assessment of the foramen ovale (every 2-4 weeks) |
| Counseling | Multidisciplinary team - MFM, pediatric cardiologist, cardiac surgeon, neonatology, palliative care |
| Delivery planning | Deliver at a center with NICU + cardiac surgery capability |
| Delivery mode | Vaginal delivery generally safe; controlled cesarean if FO is restrictive/intact atrial septum suspected |
Fetal interventions available (not at 16 weeks, but later in gestation):
- Fetal aortic valvuloplasty (FAV): for evolving HLHS with critical aortic stenosis - aims to restore forward LV flow and prevent LV hypoplasia. Technical success ~74-83% in major series; ~30-38% achieve biventricular circulation postnatally. Procedure-related fetal death rate ~16%. - Creasy & Resnik's MFM, p.785
- Fetal atrial septoplasty: percutaneous balloon dilation of a restrictive FO in the second trimester to relieve left atrial hypertension and prevent pulmonary vascular disease
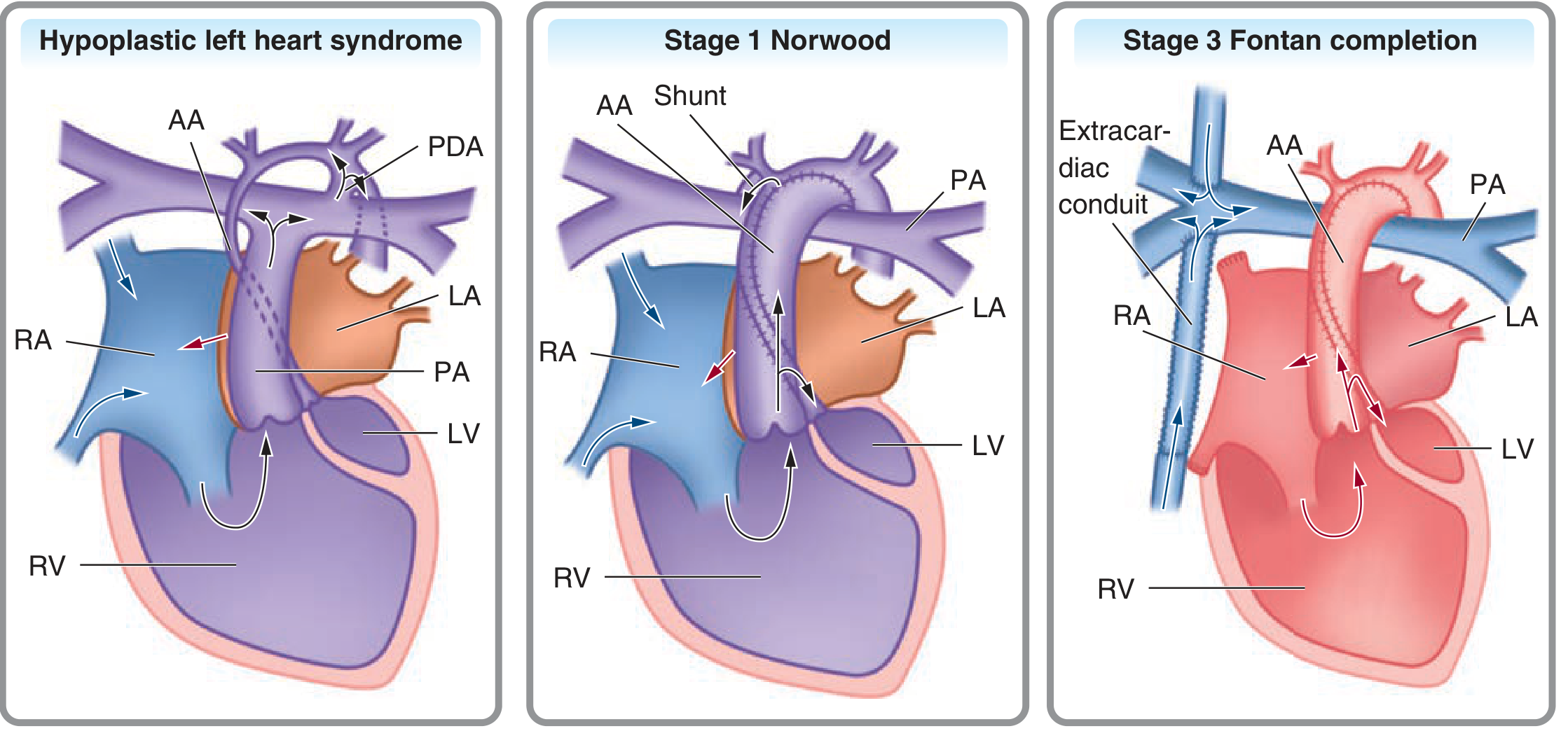
Postnatal Management: Three-Stage Palliation
HLHS is not repairable - the left heart is permanently insufficient. Palliation creates a functional single-RV circulation:
- Stage 1 - Norwood procedure (within the first 1-2 weeks of life):
- Hypoplastic aortic arch reconstructed using the proximal pulmonary trunk + homograft patch (Damus-Kaye-Stansel)
- Distal pulmonary artery is divided from the branch pulmonaries
- Pulmonary blood flow maintained by a modified Blalock-Taussig (BT) shunt or a RV-PA conduit (Sano modification)
- RV now ejects into the reconstructed systemic circulation
- Stage 2 - Glenn procedure (~3-6 months):
- Superior vena cava connected to the right pulmonary artery (bidirectional Glenn or hemi-Fontan)
- Removes ~50% of the volume load from the single RV
- Stage 3 - Fontan procedure (~2-3 years):
- Inferior vena cava connected to the pulmonary artery via an extracardiac conduit or lateral tunnel
- All systemic venous return now flows passively into the pulmonary circulation
- RV becomes a dedicated systemic pump
Alternatives: Cardiac transplantation (limited by donor organ availability); comfort/palliative care only (parental choice).
Prognosis
- 5-year survival: ≥80% at the best-performing high-volume centers
- Many patients do well early; long-term data are still maturing as the surgical era is relatively recent
- Significant proportion have neurodevelopmental delay (from altered cerebral perfusion in utero and perioperatively)
- Long-term survivors face progressive RV failure potentially requiring cardiac transplantation in adulthood
- Fontan circulation complications: elevated systemic venous pressure causes hepatic venous congestion → cirrhosis → some require liver transplantation in adulthood; also plastic bronchitis and protein-losing enteropathy are known late complications
- The overall HLHS arc from diagnosis to Fontan has shifted from near-universal lethality (pre-1980s) to majority survival with surgical palliation today
Creasy & Resnik's MFM, p.470 | Fuster & Hurst's The Heart 15th Ed., p.2034-2035
Recent evidence note: A 2024 systematic review and meta-analysis (PMID 37596875) examined fetal cardiac intervention specifically for HLHS with intact or restrictive atrial septum, confirming the rationale for fetal atrial septoplasty. A 2023 review (PMID 38204904) specifically covers prenatal diagnosis of HLHS and updates current knowledge on sonographic detection and outcomes, consistent with the textbook sources above.
This is a shared conversation. Sign in to Orris to start your own chat.