Explain NST with graph
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have all the content and images needed for a thorough explanation. Here is the complete answer:
Non-Stress Test (NST)
What is the NST?
The Non-Stress Test (NST) is the most commonly used primary tool for antepartum fetal surveillance. It has been used to assess second and third trimester fetal well-being for over 40 years. The "non-stress" in its name means no uterine contractions or stressors are applied to the fetus - it simply monitors the spontaneous fetal heart rate (FHR) response to fetal movement.
The NST serves as a surrogate measure of two things:
- The developing fetal autonomic nervous system (ANS)
- The adequacy of uteroplacental function
Physiological Basis
When the fetal ANS is intact and the fetus is well-oxygenated, fetal movement triggers FHR accelerations through peripheral nerve receptor stimulation. This coupling of movement and acceleration is the foundation of the NST. A healthy fetus in active sleep will produce frequent, grouped movements - each paired with a corresponding heart rate rise.
How to Perform the NST
- The mother is placed in a semi-recumbent position
- An external cardiotocograph (CTG) is applied to continuously record the FHR
- No uterine contractions are induced
- Monitoring window: 20-40 minutes (may extend to 60-80 min if initially non-reactive to allow for fetal sleep cycles)
Interpretation: Reactive vs. Non-Reactive
Reactive NST (Normal / Reassuring)
- At least 2 FHR accelerations within a 20-minute window
- Each acceleration rises ≥15 beats/min above baseline
- Each acceleration lasts ≥15 seconds
For preterm fetuses <32 weeks: modified criteria apply - accelerations of ≥10 bpm for ≥10 seconds are acceptable, since younger fetuses have smaller but still meaningful accelerations.
Non-Reactive NST (Abnormal)
- Fails to meet the above criteria even after 40-60 minutes
- Does not automatically mean fetal jeopardy - fetal sleep state (which can last up to 40 minutes normally) is the most common cause
- Requires further evaluation: Biophysical Profile (BPP) or Contraction Stress Test (CST)
The NST Tracing - Figure 20-13
This is a reactive NST tracing showing FHR accelerations above a baseline of 130-140 bpm with good variability:
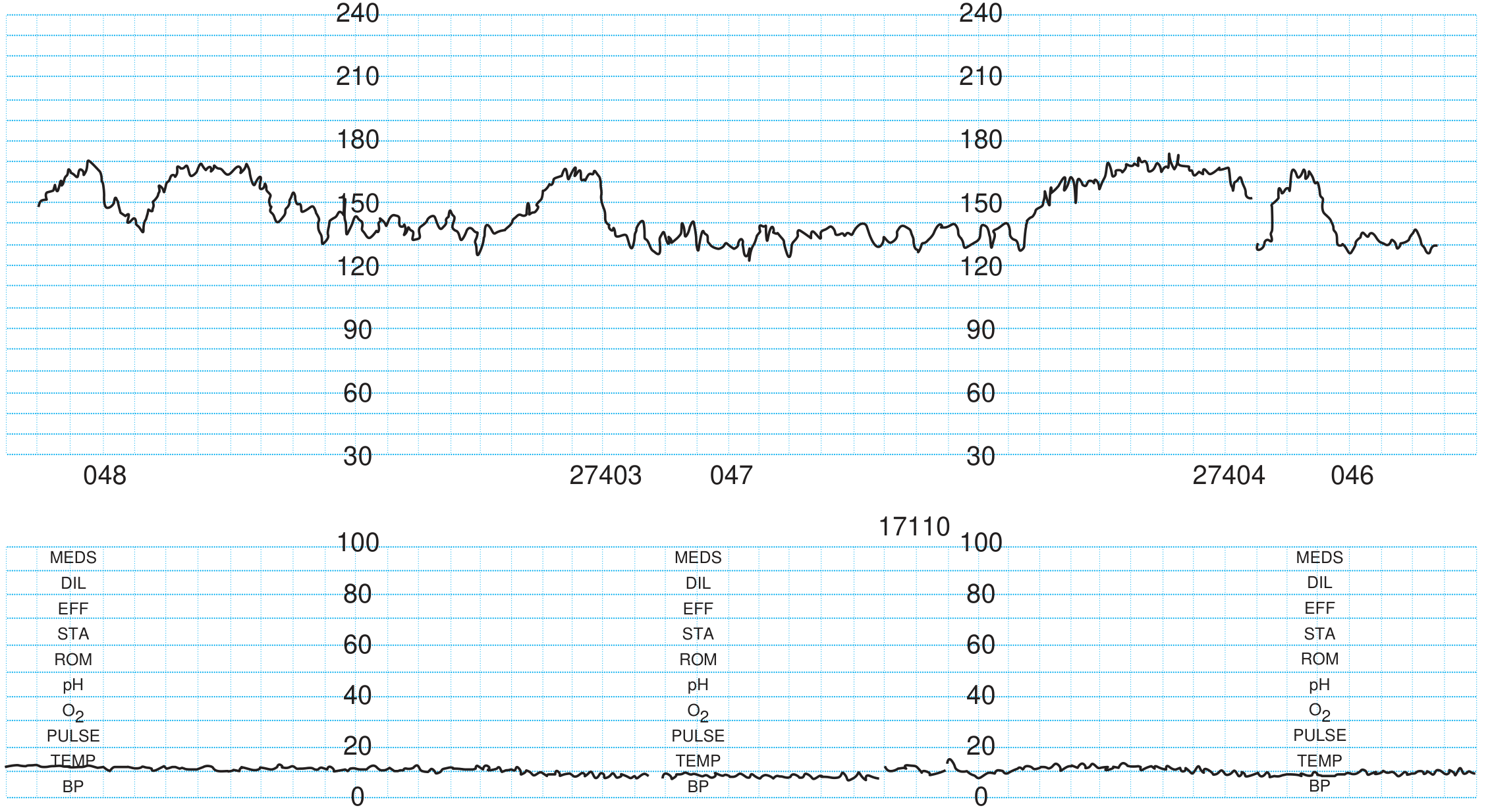
The upper channel shows the FHR (y-axis: beats/min, 30-240 scale). The upward spikes above the baseline represent accelerations associated with fetal movement. Good beat-to-beat variability (oscillations 6-25 bpm) is also visible - a sign of a healthy fetal nervous system.
FHR Variability on NST - What to Look For
Variability is one of the most important indicators of fetal well-being. Here are the four categories defined by NICHD guidelines:
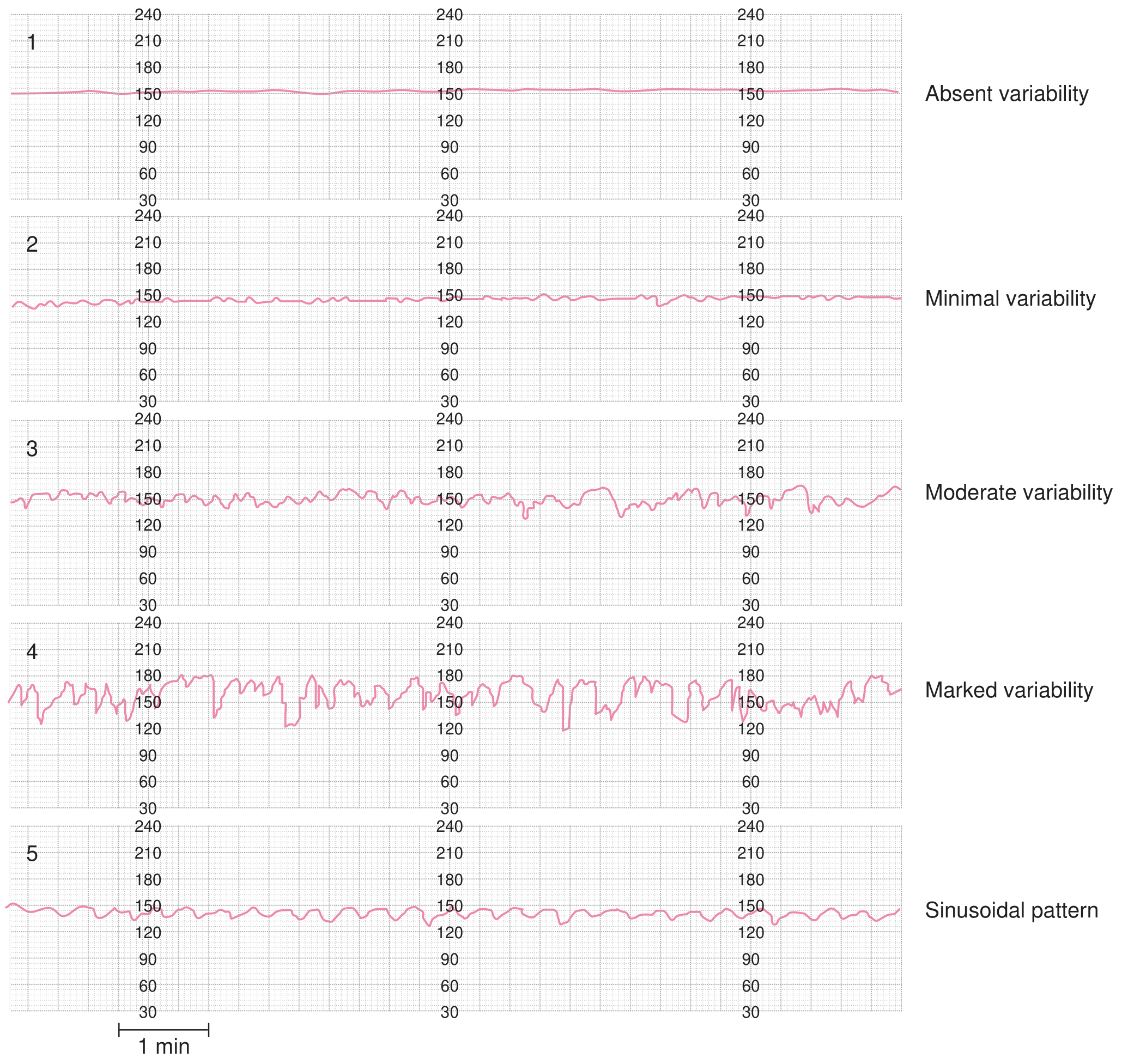
| Category | Amplitude | Clinical Significance |
|---|---|---|
| Absent | Undetectable | Ominous - associated with fetal acidosis |
| Minimal | ≤5 bpm | Could reflect sleep, CNS depressants, or compromise |
| Moderate | 6-25 bpm | Normal, reassuring |
| Marked | >25 bpm | Possibly associated with hypoxia or cord compression |
| Sinusoidal | Smooth sine wave | Ominous - seen in fetal anemia |
The presence of decreased variability + late or severe variable decelerations together is an ominous combination.
Causes of Non-Reactive NST
| Cause | Notes |
|---|---|
| Fetal sleep state | Most common; lasts 20-40 min, rarely up to 2 hours |
| Extreme prematurity | Immature ANS |
| Maternal narcotics / CNS depressants | Cross placenta and suppress fetal CNS |
| Magnesium sulfate | Decreases FHR variability and accelerations |
| Fetal cardiac anomalies | Structural limitation on rate response |
| Fetal CNS anomalies | Disrupted autonomic coupling |
| True fetal compromise / hypoxia | Acidosis suppresses cardiac reflex responses |
Accuracy and Limitations
| Parameter | Value |
|---|---|
| False-negative rate (fetal death within 1 week of reactive NST) | ~1.9 per 1000 |
| % of term fetuses non-reactive at 30 min | ~10-12% |
| % still non-reactive at 40 min | <6% |
The NST is more specific than sensitive - it is a better indicator of fetal health than fetal illness. A reactive result is reassuring; a non-reactive result does not confirm compromise and must be followed up.
NST as Part of the Biophysical Profile (BPP)
In the BPP, the NST contributes 2 points out of a maximum score of 10:
| NST Score = 2 (Normal) | NST Score = 0 (Abnormal) |
|---|---|
| Moderate variability + accelerations coupled with fetal movements on a 30-min NST | FM and accelerations not coupled; insufficient, absent, or decelerative trace |
A BPP score of 8-10 is reassuring; 6 is suspicious; ≤4 is ominous and warrants immediate intervention.
Indications for NST
- Gestational diabetes mellitus
- Chronic hypertension / pre-eclampsia
- Post-term pregnancy (≥41 weeks)
- Intrauterine growth restriction (IUGR/FGR)
- Multiple gestation
- Prior fetal demise
- Decreased fetal movement reported by mother
- Oligohydramnios
For low-to-moderate risk conditions, weekly NST starting at 32 weeks is a common protocol. Higher-risk cases require earlier and more frequent testing.
Sources: Textbook of Family Medicine, 9e; Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice
This is a shared conversation. Sign in to Orris to start your own chat.