Lung Carcinoma neetpg inicet
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have comprehensive information to compile a thorough NEET PG / INICET-focused answer on Lung Carcinoma. Let me present this in a well-organized, high-yield format.
Lung Carcinoma - NEET PG / INICET High-Yield Notes
1. Epidemiology & Risk Factors
- Most common cause of cancer death worldwide in both sexes
- Smoking is the #1 risk factor for ALL types - risk is 60x higher with heavy smoking (2 packs/day x 20 years) vs. nonsmokers
- ~90% of lung cancers occur in current or recent smokers
- Women are more susceptible to tobacco carcinogens than men
- Other risk factors: asbestos, radon, arsenic, nickel, chromium, air pollution, radiation
- Asbestos + smoking = synergistic (multiplicative) risk
2. WHO Classification (2021)
| Type | Key Points |
|---|---|
| Adenocarcinoma | Most common overall |
| Squamous cell carcinoma | Central, hilar |
| Large cell carcinoma | Peripheral |
| Small cell carcinoma | Central, neuroendocrine |
| Carcinoid tumor | Low-grade neuroendocrine |
| Adenosquamous carcinoma | Mixed |
| Sarcomatoid carcinoma | Giant/spindle cell variants |
3. Histologic Types - Key Features (MOST TESTED)
A. Adenocarcinoma
- Most common type overall (including in nonsmokers, women)
- Peripheral location (subpleural)
- Arises from: atypical adenomatous hyperplasia → adenocarcinoma in situ (AIS) (formerly bronchioloalveolar carcinoma)
- Lepidic growth pattern = growth along pre-existing alveolar walls without stromal invasion (AIS = pure lepidic, ≤3 cm)
- Key mutations: EGFR (~20%, nonsmokers/women), KRAS (~30%), ALK fusions (4-6%, nonsmokers, signet ring morphology), ROS1, HER2, MET
- EGFR and KRAS mutations are mutually exclusive
- ALK fusions: often have signet ring morphology; treated with crizotinib/alectinib
- Targetable with TKIs (gefitinib, erlotinib for EGFR; crizotinib for ALK)
B. Squamous Cell Carcinoma (SCC)
- Central/hilar location (arises from bronchial epithelium)
- Arises from: squamous dysplasia → squamous CIS (via squamous metaplasia)
- Histology: keratin pearls, intercellular bridges
- Strongly associated with smoking
- Paraneoplastic: PTHrP → hypercalcemia (most classic association)
- Key mutation: p16/CDKN2A (~50%)
- Cavitation common
C. Small Cell Carcinoma (SCLC)
- Central location, near major bronchi
- Neuroendocrine origin (Kulchitsky cells)
- Oat-cell appearance: scant cytoplasm, hyperchromatic nuclei, fine chromatin ("salt and pepper"), indistinct nucleoli
- IHC markers: chromogranin A, synaptophysin, CD56, NSE
- Dense core granules on electron microscopy
- Paraneoplastic syndromes (most common of all types):
- SIADH → hyponatremia (ADH secretion)
- Cushing syndrome → ACTH secretion
- Lambert-Eaton myasthenic syndrome (anti-VGCC antibodies)
- Anti-Hu antibody → encephalomyelitis/sensory neuropathy
- Key mutations: TP53 (~90%), RB (~90%), 3p deletion (~90%)
- Virtually always metastatic at diagnosis → NOT surgical → chemotherapy + radiotherapy
- Responds to chemo initially but invariably recurs
- Median survival with treatment: ~1 year; 5-year survival: only 5%
- Less responsive to immune checkpoint inhibitors than NSCLC
D. Large Cell Carcinoma
- Peripheral location
- Diagnosis of exclusion (no squamous, glandular, or neuroendocrine differentiation)
- Poorly differentiated; abundant cytoplasm, prominent nucleoli
- Large cell neuroendocrine carcinoma (LCNEC) is a subset
4. Comparison Table: SCLC vs. NSCLC (MUST MEMORIZE)
| Feature | SCLC | NSCLC (Adeno/SCC) |
|---|---|---|
| Morphology | Scant cytoplasm; small hyperchromatic nuclei; fine chromatin; indistinct nucleoli | Abundant cytoplasm; pleomorphic nuclei; coarse chromatin; prominent nucleoli |
| Neuroendocrine markers (chromogranin, synaptophysin, CD56) | Present | Absent |
| Mucin | Absent | Present in adenocarcinoma |
| PTH-rP | - | SCC (hypercalcemia) |
| ACTH/ADH secretion | Predominantly SCLC | Occasionally |
| 3p deletion | ~90% | ~80% |
| RB mutations | ~90% | ~20% |
| TP53 mutations | ~90% | ~50% |
| p16/CDKN2A mutations | ~10% | ~50% |
| KRAS mutations | Rare | ~30% (adenocarcinoma) |
| EGFR mutations | Absent | ~20% (adenocarcinoma) |
| ALK fusions | Absent | 4-6% (adenocarcinoma) |
| Response to chemotherapy | Often complete (but recurs) | Incomplete |
| Response to checkpoint inhibitors | Unresponsive | Responsive |
| Surgery | Not curative (always metastatic) | Potentially curative if localized |
(Source: Robbins & Kumar Basic Pathology, Table 11.6)
5. Paraneoplastic Syndromes (HIGH YIELD)
| Syndrome | Mediator | Tumor Type |
|---|---|---|
| SIADH (hyponatremia) | ADH | SCLC (predominantly) |
| Cushing syndrome | ACTH | SCLC (predominantly) |
| Hypercalcemia | PTHrP | Squamous cell carcinoma |
| Lambert-Eaton syndrome | Anti-VGCC autoantibodies | SCLC |
| Hypertrophic pulmonary osteoarthropathy + clubbing | - | Any (esp. adeno) |
| Gynecomastia | Gonadotropins | Any |
| Peripheral neuropathy / encephalomyelitis | Anti-Hu antibody | SCLC |
| Carcinoid syndrome | Serotonin/bradykinin | Carcinoid |
| Trousseau syndrome (DVT/thromboembolism) | Hypercoagulable | Adenocarcinoma |
| Acanthosis nigricans | - | Any |
Key rule: SCLC predominantly produces ACTH and ADH; SCC predominantly produces PTHrP (hypercalcemia). Any histologic type may occasionally produce any hormone.
6. Molecular Pathogenesis
- 3p deletion - earliest molecular event (even in histologically normal smoker bronchial epithelium = "field effect")
- TP53 mutations - relatively late event
- KRAS mutations - relatively late event (adenocarcinoma)
- Sequence for SCC: Normal epithelium → Squamous metaplasia → Squamous dysplasia → CIS → Invasive SCC
- Sequence for adeno: Normal → Atypical adenomatous hyperplasia → AIS → Minimally invasive → Invasive adenocarcinoma
7. Clinical Features
- Cough, hemoptysis, dyspnea, wheezing (central tumors cause obstruction)
- SVC syndrome - SCLC (most common cause) compresses SVC
- Horner syndrome - Pancoast tumor (superior sulcus) compresses cervical sympathetic chain → ptosis, miosis, anhidrosis
- Pancoast tumor (superior sulcus tumor): shoulder/arm pain, Horner syndrome, rib erosion
- Recurrent laryngeal nerve palsy - hoarseness
- Phrenic nerve palsy - elevated hemidiaphragm
- Pleural effusion, pericardial involvement
8. Diagnosis
- Chest X-ray / CT scan for detection and staging
- Sputum cytology - positive in central tumors (SCC, SCLC)
- Bronchoscopy + biopsy (central tumors)
- CT-guided needle biopsy (peripheral lesions)
- PET-CT for staging
- Mediastinoscopy for N2 nodal staging
- Molecular testing mandatory: EGFR, ALK, KRAS, ROS1, PD-L1 for NSCLC
9. Treatment Summary
| Type | Treatment |
|---|---|
| NSCLC (early, stages I-II) | Surgery (lobectomy) |
| NSCLC (locally advanced) | Chemo + radiation ± surgery |
| NSCLC with EGFR mutation | Gefitinib/Erlotinib/Osimertinib |
| NSCLC with ALK fusion | Crizotinib/Alectinib/Brigatinib |
| NSCLC with high PD-L1 | Pembrolizumab (checkpoint inhibitor) |
| NSCLC with KRAS G12C | Sotorasib |
| SCLC (limited) | Chemo (cisplatin/etoposide) + radiotherapy |
| SCLC (extensive) | Chemotherapy (+ atezolizumab in some) |
10. Quick One-Liners for MCQs
- Most common lung cancer overall = Adenocarcinoma
- Most common in smokers = Adenocarcinoma (also most common in nonsmokers)
- Most central tumor = SCLC or SCC
- Most peripheral = Adenocarcinoma or Large cell
- Cavitation most common in = SCC (also large cell)
- "Oat cells" = SCLC
- "Keratin pearls" = SCC
- Best treated with surgery = NSCLC (early)
- Never surgical = SCLC (usually)
- PTHrP hypercalcemia = SCC
- SIADH + Cushing = SCLC
- Lambert-Eaton = SCLC
- Lepidic growth / AIS = Adenocarcinoma
- EGFR mutation + female + nonsmoker = Adenocarcinoma
- ALK fusion + signet ring = Adenocarcinoma
- 3p deletion earliest molecular change = All lung cancers
- RB mutation 90% = SCLC
- p16/CDKN2A mutation 50% = NSCLC (SCC)
- Finger clubbing + periostitis = Hypertrophic pulmonary osteoarthropathy
- Pancoast tumor location = Apex of lung (superior sulcus)
- Pancoast tumor = SCC most commonly
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Fishman's Pulmonary Diseases and Disorders
Provide images related to this
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have all the key images. Let me present them in a well-organized, annotated format for NEET PG/INICET study.
Lung Carcinoma - Images from Robbins Pathology
IMAGE 1: Pathology of Lung Carcinomas - Complete Panel (Robbins Basic Pathology)
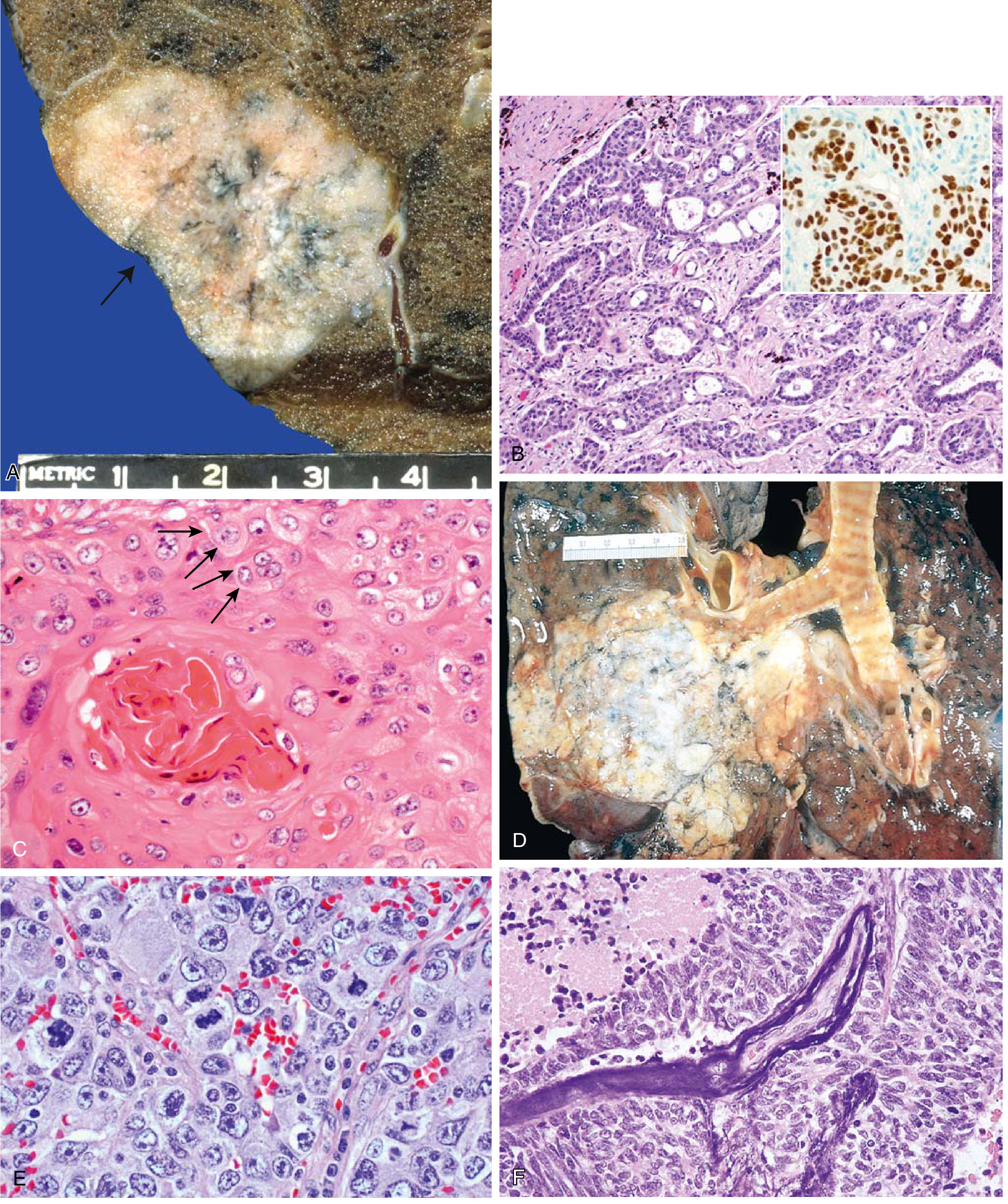
Fig. 11.44 - Robbins & Kumar Basic Pathology
| Panel | What to see | Key Feature |
|---|---|---|
| A | Gross: Lung adenocarcinoma (peripheral) | Central scarring with anthracotic pigments, pleural puckering (arrow) |
| B | Micro: Gland-forming adenocarcinoma | Acinar glands; inset = TTF-1 positive (brown nuclear staining) |
| C | Micro: Well-differentiated SCC | Keratin pearls + intercellular bridges (arrows) |
| D | Gross: SCC as central (hilar) mass | Gray-white tumor invading lung parenchyma centrally |
| E | Micro: Large cell carcinoma | Sheets of large cells - no glands, no squamous differentiation |
| F | Micro: Small cell carcinoma | Small deeply basophilic cells + necrosis; Azzopardi effect = blue DNA encrusting vessel walls |
IMAGE 2: Pathology of Lung Carcinomas - Robbins, Cotran & Kumar (Pathologic Basis of Disease)
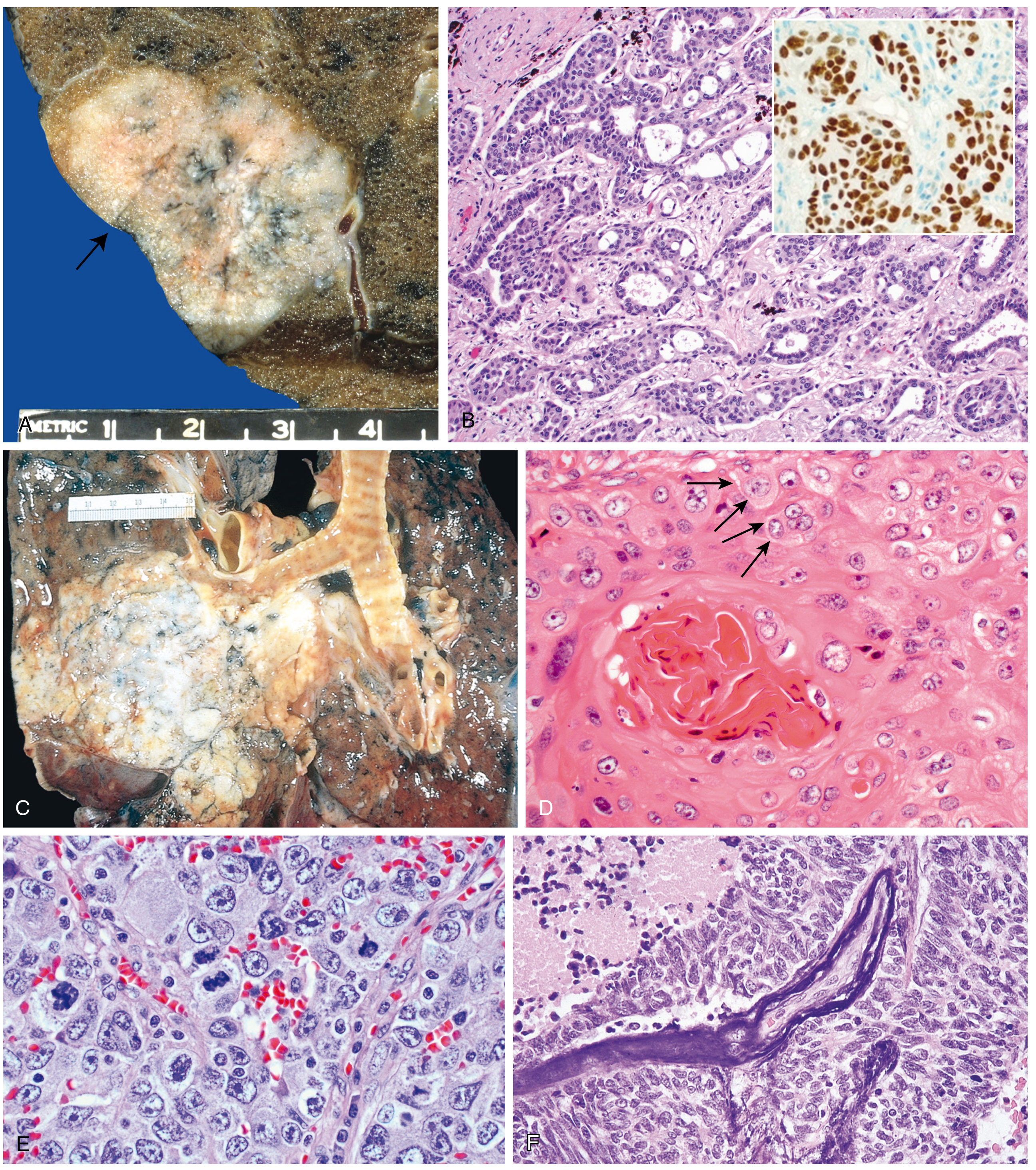
Fig. 15.34 - Robbins, Cotran & Kumar Pathologic Basis of Disease
| Panel | What to see | Key Feature |
|---|---|---|
| A | Gross: Peripheral lung adenocarcinoma | Subpleural scar + anthracotic pigment (arrow) |
| B | Micro: Gland-forming adenocarcinoma | Inset: TTF-1 IHC - hallmark of pulmonary adenocarcinoma |
| C | Gross: SCC as central hilar mass | Bilateral tumor obliterating bronchi at carina |
| D | Micro: Well-differentiated SCC | Keratin pearl (concentric pink whorls) + intercellular bridges (arrows) |
| E | Micro: Large cell carcinoma | Sheets of pleomorphic large cells, no specific differentiation |
| F | Micro: Squamous cell carcinoma | Keratinized cells / squamous architecture |
NEET MCQ tip: TTF-1 positivity = adenocarcinoma (also positive in small cell carcinoma). p40/p63 positivity = squamous cell carcinoma.
IMAGE 3: Precursor Lesions of Lung Cancer (Robbins, Cotran & Kumar)
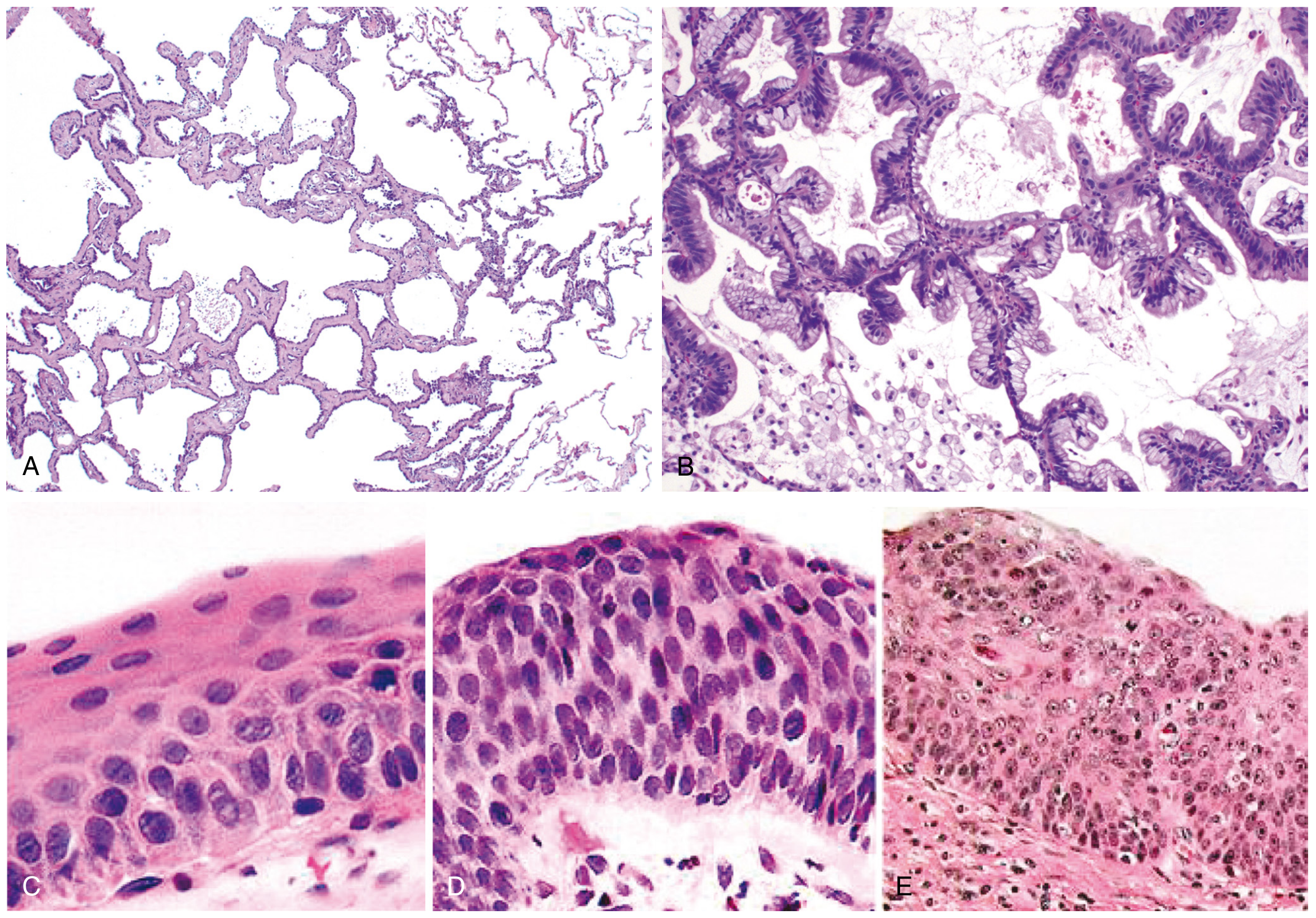
Fig. 15.33 - Precursor lesions
| Panel | Lesion | What to see |
|---|---|---|
| A | Atypical adenomatous hyperplasia (AAH) | Mild septal thickening; slightly enlarged atypical pneumocytes lining alveoli (≤5 mm) |
| B | Adenocarcinoma in situ (AIS) - mucinous type | Tall columnar mucinous cells growing along alveolar septations - classic lepidic pattern |
| C | Squamous metaplasia / basal cell hyperplasia | Bronchial epithelium replaced by squamous cells - earliest change |
| D | Squamous dysplasia | Disordered squamous epithelium - loss of polarity, hyperchromasia, pleomorphism |
| E | Squamous cell carcinoma in situ (CIS) | Full-thickness dysplasia; basement membrane intact - immediately precedes invasion |
Sequence to memorize: Normal → AAH → AIS (lepidic, ≤3cm, no invasion) → Minimally invasive → Invasive adenocarcinoma Normal → Metaplasia → Dysplasia → CIS → Invasive SCC
IMAGE 4: Sputum Cytology - Squamous Cell Carcinoma
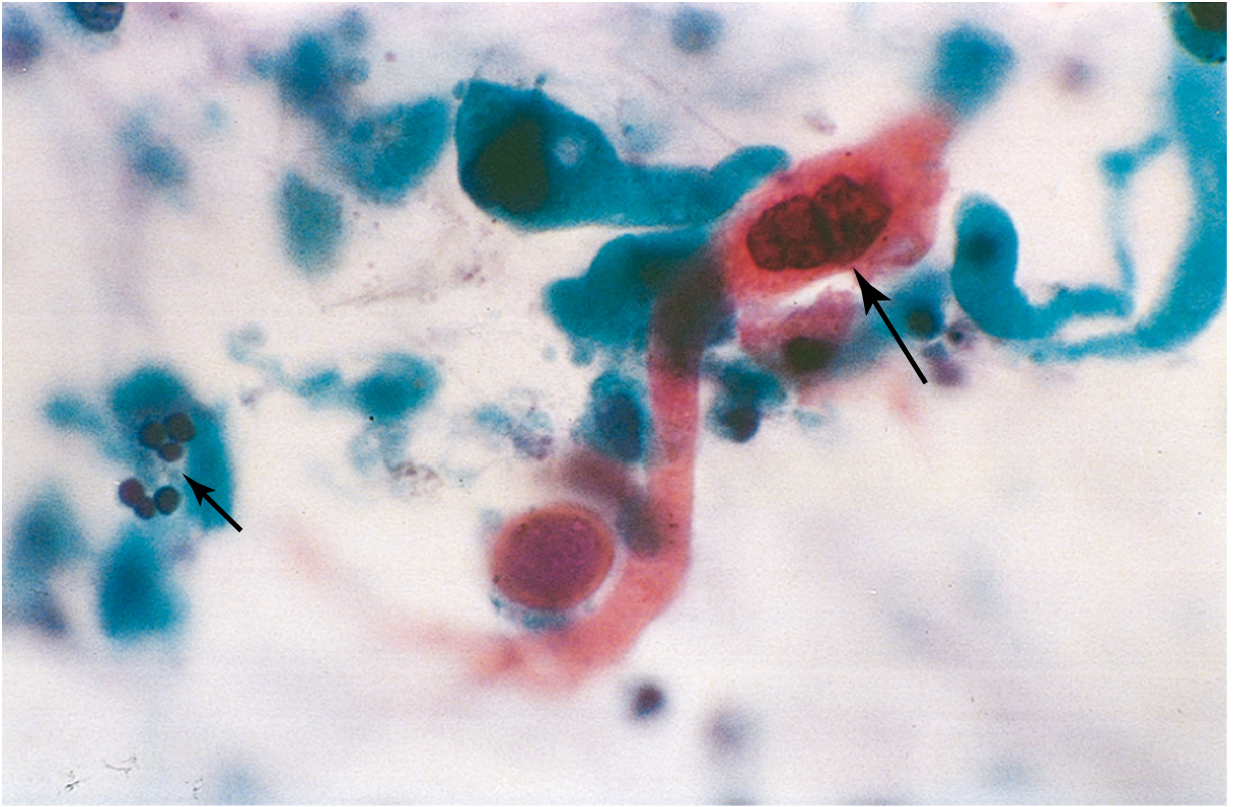
Fig. 15.35 - Cytologic diagnosis of lung cancer
- Large arrow: Orange-staining, keratinized squamous carcinoma cell with hyperchromatic nucleus - the diagnostic cell in sputum
- Small arrow: Normal neutrophils for size comparison
- The tumor cell is dramatically larger with a markedly abnormal nucleus
- Orange staining = keratin (Papanicolaou stain)
NEET tip: Sputum cytology is most useful for central tumors (SCC, SCLC) - cells shed into the bronchial lumen. Peripheral adenocarcinoma = CT-guided biopsy preferred.
Key Histologic Identifiers - Quick Reference
| Feature on Histology | Tumor |
|---|---|
| Keratin pearls + intercellular bridges | Squamous cell carcinoma |
| Gland formation + TTF-1+ | Adenocarcinoma |
| Lepidic growth along alveolar walls | Adenocarcinoma in situ |
| Small cells, scant cytoplasm, salt-and-pepper chromatin, crush artifact, Azzopardi effect | Small cell carcinoma |
| Large cells, no differentiation (diagnosis of exclusion) | Large cell carcinoma |
| Neuroendocrine nests, "salt-and-pepper" chromatin, no mitoses | Carcinoid tumor |
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.