Homeopathy
Searching the Web
homeopathy scientific evidence 2024 2025
Searching PubMed
homeopathy placebo systematic review
Here is a thorough overview of homeopathy, covering its history, principles, and the scientific evidence.
What Is Homeopathy?
Homeopathy was developed in 1796 by German physician Samuel Hahnemann. It rests on two foundational ideas:
- "Like cures like" (similia similibus curentur) - A substance that produces symptoms in a healthy person can treat similar symptoms in a sick person. For example, onion (which causes watery eyes) would be used to treat hay fever.
- "Law of infinitesimals" - The more a substance is diluted, the more potent it becomes. Standard remedies are diluted on a "C" scale: 1C = 1 part in 100, 30C = 1 part in 10^60. At 12C and above, not a single molecule of the original substance is statistically likely to remain. Proponents claim water retains a "memory" of the substance.
Preparations are made by serial dilution with vigorous shaking ("succussion") between steps.
What the Evidence Shows
The Scientific Consensus
The overwhelming scientific and regulatory consensus is that homeopathy does not work beyond placebo:
- Australia (NHMRC, 2015, reviewed 2024): After reviewing over 1,800 studies, the National Health and Medical Research Council found "no good quality evidence to support the claim that homeopathy is effective in treating health conditions." The 2024 Australian Natural Therapies Review reaffirmed this conclusion.
- UK (House of Commons Science and Technology Committee, 2010): Concluded homeopathy is no more effective than placebo and should not receive NHS funding.
- U.S. FDA & FTC: Both agencies have issued statements that homeopathic products lack credible scientific evidence of efficacy.
Systematic Reviews on PubMed
Key meta-analyses and systematic reviews (including Hamre et al., 2023 - PMID 37805577) consistently find that when trial quality is higher (better blinding, larger samples, pre-registration), the effect sizes for homeopathy shrink toward zero - a hallmark of placebo responses rather than true drug effects. The Mathie et al. series (2018-2019) in the journal Homeopathy attempted to find a signal in well-designed trials and found mostly low-quality evidence with inconclusive results.
Why Positive Studies Exist (But Don't Hold Up)
- Publication bias - Positive results are more likely to be published.
- Small sample sizes - Many studies are underpowered.
- Poor blinding - Patients or practitioners can often tell which group they're in.
- Regression to the mean - People seek treatment when symptoms are at their worst; they naturally improve.
The Physics and Chemistry Problem
The core issue is that homeopathy's mechanism is not just unproven - it is implausible under known physics and chemistry:
- Avogadro's number (6.022 × 10²³) sets a hard limit: at dilutions beyond ~12C, no molecules of the original substance remain.
- The "water memory" hypothesis has never been demonstrated under controlled conditions. Water forms hydrogen bonds that last picoseconds, not long enough to carry biological information.
- If water did memorize dissolved substances, it would "remember" every contaminant it has ever contacted.
Homeopathy vs. Herbal Medicine
A common confusion: homeopathy is not herbal medicine. Herbal medicine uses active plant compounds at detectable concentrations. Many herbal remedies have real pharmacological effects. Homeopathic remedies are diluted to the point of containing nothing but water or a lactose pill.
Regulatory and Safety Status
- Homeopathic products are generally considered safe because they contain no active substance - but this also means no therapeutic effect.
- Risk comes from delaying real treatment: people with serious conditions (cancer, infections, diabetes) who use homeopathy instead of evidence-based care face real harm.
- In the U.S., the FDA has increased regulatory scrutiny since 2017, particularly for products marketed for children.
Bottom Line
Homeopathy is a pre-scientific system with no plausible mechanism, and the highest-quality clinical evidence consistently shows no effect beyond placebo. It remains popular in some countries (France, Germany, India) due to cultural tradition and the therapeutic benefit of the lengthy, empathetic consultations practitioners typically provide - but that benefit comes from the consultation, not the remedy.
Psoriasis
Reading File
Finding Sources
Searching PubMed
psoriasis treatment biologics
Searching the Web
psoriasis pathophysiology treatment guidelines 2025
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
Finding Sources
I now have thorough content from multiple authoritative sources. Let me compile the comprehensive response.
Psoriasis
Overview
Psoriasis is a common, chronic, immune-mediated inflammatory skin disease affecting approximately 1-2% of the population worldwide. It is characterized by discrete plaques with adherent silvery-white (micaceous) scales occurring at sites of predilection, particularly extensor surfaces. It is now understood as a systemic disease - not merely a skin condition - with significant associated comorbidities.
- Fitzpatrick's Dermatology, p. 227
- Andrews' Diseases of the Skin, Ch. 10
Pathophysiology
The central mechanism involves dysregulation of the IL-23/Th17 axis:
- Dermal dendritic cells produce TNF-α and IL-23 in response to triggers (trauma, infection, stress, drugs).
- IL-23 drives differentiation and survival of Th17 cells, which produce IL-17A, IL-17F, and IL-22.
- IL-17 acts on keratinocytes, causing hyperproliferation, abnormal differentiation, and secretion of antimicrobial peptides (defensins), chemokines, and inflammatory mediators.
- This creates a self-amplifying loop: keratinocytes secrete IL-8 and GRO-α, which recruit neutrophils (forming Munro's microabscesses in the stratum corneum) and more T cells (epidermotropism).
The epidermis thickens dramatically - basal keratinocyte transit time drops from ~28 days to ~3-4 days, producing the characteristic parakeratotic, silvery scale. Capillary loops extend into the superficial dermis, explaining the Auspitz sign (pinpoint bleeding when scale is removed).
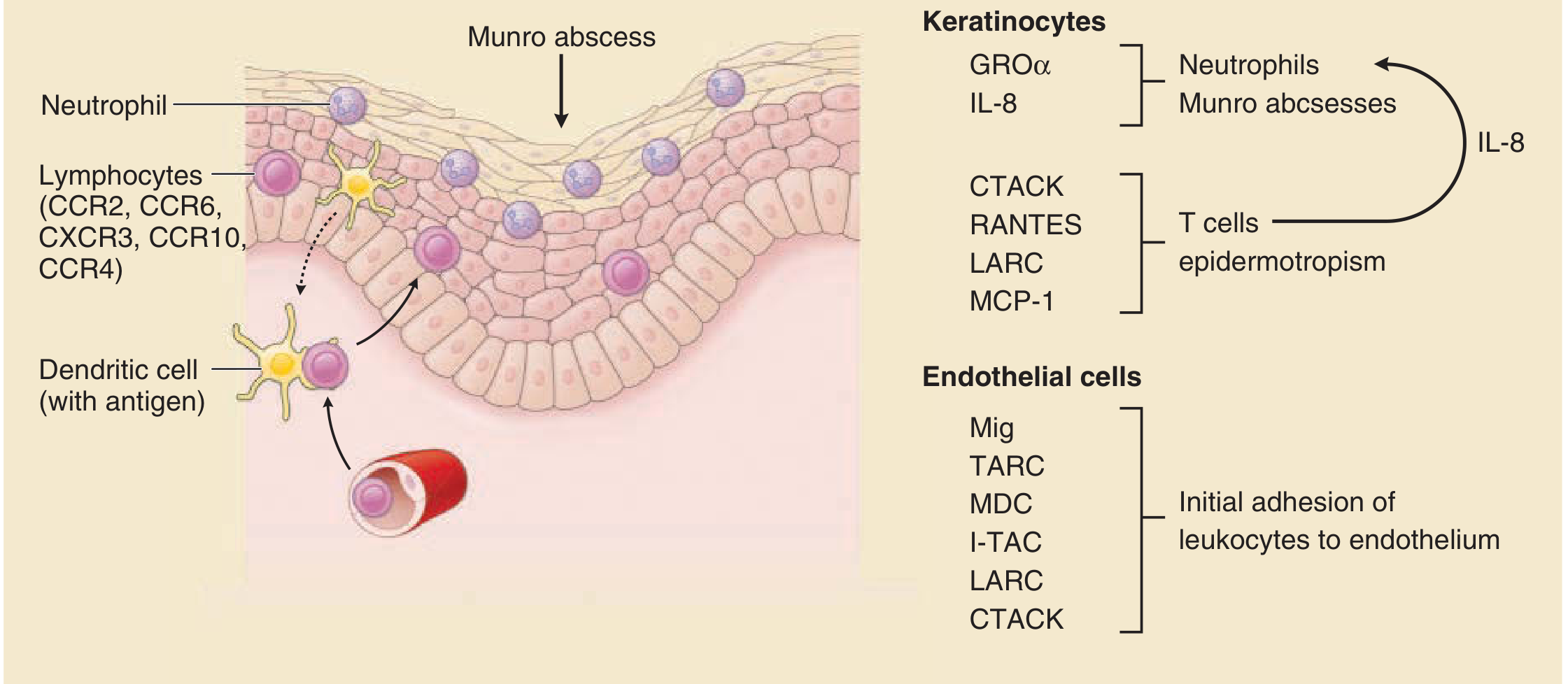
Chemokine actions in psoriasis (Fitzpatrick's Dermatology, Fig. 12-11)
Genetics
- Strong genetic component: risk ~16% with one parent affected, up to ~50% with both parents affected.
- Key susceptibility loci: HLA-Cw6 (strongest association), IL23A, IL12B, IL17RA, PSORS1 locus on chromosome 6p.
- Two bimodal age peaks of onset: 16-22 years (type I, HLA-linked, more severe) and 57-60 years (type II, less familial).
Clinical Types
| Type | Features |
|---|---|
| Plaque (vulgaris) | 80-90% of cases; well-demarcated, erythematous plaques with silvery scale; elbows, knees, scalp, lumbosacral |
| Guttate | Small (2-5 mm) "water drop" lesions; triggered by streptococcal pharyngitis; mostly <30 yrs |
| Inverse | Smooth, erythematous plaques in skin folds (axilla, groin, inframammary, intergluteal); minimal scale; often mimics candida |
| Pustular | Sterile pustules; can be localized (palmoplantar) or generalized (von Zumbusch) - a medical emergency |
| Erythrodermic | Widespread erythema + scale involving >90% BSA; unstable, life-threatening |
| Scalp | Plaques on scalp; can extend beyond hairline |
| Palmoplantar | Thick plaques on palms and soles; highly debilitating |
| Nail | Pitting, onycholysis, "oil spots," subungual hyperkeratosis |
| Psoriatic arthritis | Affects ~30% of patients; joints of hands, feet, knees; can be destructive |
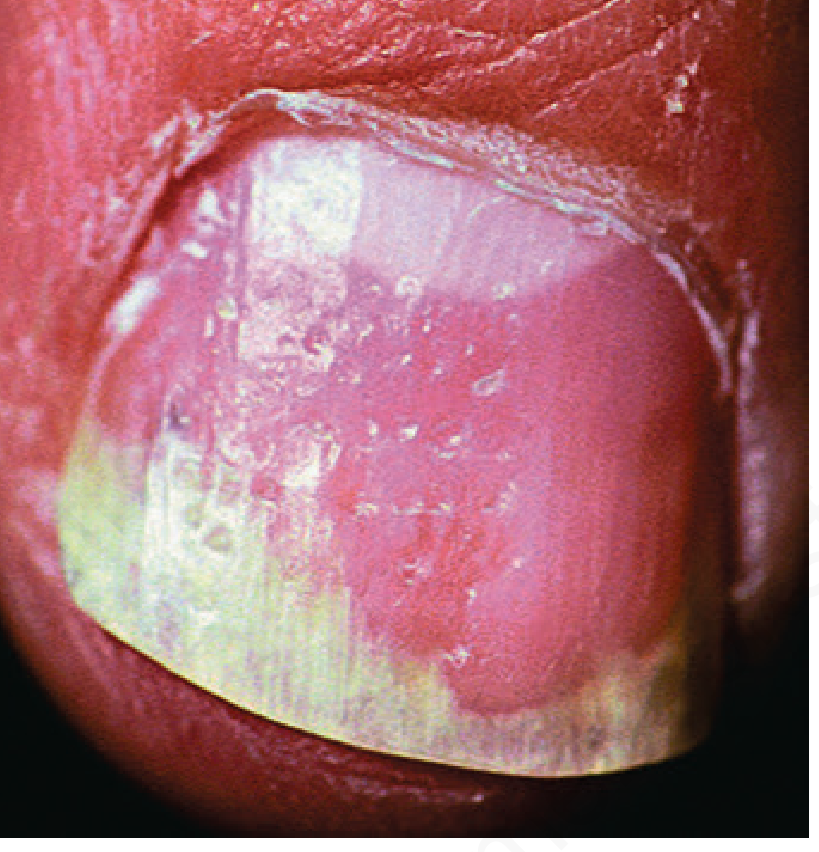
Nail pitting and distal onycholysis - Andrews' Diseases of the Skin, Fig. 10.6
Important: Never treat psoriasis with systemic corticosteroids - withdrawal can precipitate life-threatening generalized pustular psoriasis.
Triggers
- Koebner phenomenon (trauma to skin)
- Streptococcal infections (especially guttate)
- Medications: lithium, beta-blockers, antimalarials, NSAIDs, systemic steroid withdrawal
- HIV infection
- Stress, alcohol, smoking
- Obesity
Diagnosis
Usually clinical. Key features:
- Auspitz sign: pinpoint bleeding on scale removal
- Koebner phenomenon: lesions at trauma sites
- Woronoff ring: pale halo around resolving plaques
Biopsy if atypical (shows acanthosis, parakeratosis, Munro microabscesses, dilated dermal capillaries, loss of granular layer).
Comorbidities
Psoriasis is now recognized as a systemic inflammatory disease associated with:
- Psoriatic arthritis (~30%)
- Cardiovascular disease (increased MI risk, especially in severe psoriasis)
- Metabolic syndrome (obesity, hypertension, dyslipidemia, diabetes)
- Inflammatory bowel disease (Crohn's, UC)
- Depression and anxiety
- Non-alcoholic fatty liver disease
Treatment
Severity Assessment
- Mild: <10% BSA, limited impact on QoL → topical therapy
- Moderate-Severe: ≥10% BSA, or involvement of face/hands/genitals/nails, or psoriatic arthritis, or failed topical therapy → phototherapy or systemic agents
Step 1 - Topical Therapy (mild disease)
| Agent | Notes |
|---|---|
| Potent topical corticosteroids (e.g. clobetasol) | First-line; 68-89% achieve clearance (SOR: A) |
| Vitamin D analogues (calcipotriol/calcipotriene) | Comparable efficacy to clobetasol; combined with steroid = best results |
| Tazarotene (topical retinoid) | Effective; can cause irritation |
| Tacrolimus 0.1% | For facial and inverse psoriasis (avoids steroid side effects) |
| Coal tar | Older agent; antiproliferative |
| Salicylic acid | Keratolytic; helps remove scale |
Step 2 - Phototherapy (moderate disease)
- Narrowband UVB (NB-UVB): Safer and more effective than broadband UVB; first-line phototherapy (SOR: A)
- Broadband UVB: One situation where it may outperform NB-UVB: guttate psoriasis requiring erythemogenic doses
- PUVA (psoralen + UVA): Highly effective but higher risk of skin cancer and cataracts; reserved for refractory cases
Step 3 - Conventional Systemic Agents
| Drug | Dose | Notes |
|---|---|---|
| Methotrexate | 5-15 mg/week | Effective for skin + joints; hepatotoxic - monitor LFTs; contraindicated in pregnancy |
| Cyclosporine | ~3-5 mg/kg/day | Rapid onset; nephrotoxic; short-term use only (≤1-2 years) |
| Acitretin (oral retinoid) | 25-50 mg/day | Best for pustular/palmoplantar psoriasis; teratogenic (avoid 3 yrs post-use) |
| Fumaric acid esters | - | First-line in Germany; GI side effects |
| Apremilast (PDE4 inhibitor) | 30 mg BID | Oral; modest efficacy; useful when biologics contraindicated |
Step 4 - Biologics (moderate-severe disease)
Biologics have transformed psoriasis management. Targets and agents:
Anti-TNF-α:
- Etanercept (Enbrel) - SubQ; good for psoriatic arthritis
- Adalimumab (Humira) - SubQ; skin + joints
- Infliximab (Remicade) - IV; fastest onset; very effective
Anti-IL-12/23 (p40 subunit):
- Ustekinumab (Stelara) - SubQ; dosing every 12 weeks after induction
Anti-IL-17:
- Secukinumab (Cosentyx) - Highest PASI 90 rates in early trials
- Ixekizumab (Taltz) - Very high skin clearance rates
- Bimekizumab (targets IL-17A and IL-17F) - Newer, very high efficacy
Anti-IL-23 (p19 subunit - most selective):
- Guselkumab, Risankizumab, Tildrakizumab - Every 8-12 weeks; excellent sustained clearance rates
Newer oral agents:
- Deucravacitinib (TYK2 inhibitor) - Oral; targets the IL-23/IL-17 pathway upstream; approved 2022; favorable safety profile vs. JAK inhibitors
The 2023 Cochrane network meta-analysis (PMID 37436070) comparing all systemic treatments found bimekizumab and ixekizumab consistently ranked highest for achieving PASI 90 responses. The 2023/2025 EuroGuiDerm guidelines provide decision grids for choosing between agents based on comorbidities (IBD, cardiac disease, pregnancy, TB, etc.).
The 2024 EULAR guidelines (PMID 38499325) updated recommendations specifically for psoriatic arthritis.
Special Situations
- Psoriatic arthritis: Prefer anti-TNF or anti-IL-17 agents (have joint + skin data); IL-23 inhibitors also effective for joints
- IBD comorbidity: Avoid anti-IL-17 (can worsen IBD); prefer anti-TNF (infliximab) or ustekinumab
- Pregnancy: Cyclosporine preferred if systemic needed; all biologics generally avoided; acitretin absolutely contraindicated
- Latent TB: Screen all patients before biologics; prefer agents with better TB safety profile
Prognosis
Psoriasis is a lifelong, relapsing-remitting condition. It cannot currently be cured, but modern biologics allow sustained skin clearance (PASI 90 or 100) in the majority of patients. Quality of life, cardiovascular risk, and metabolic comorbidities must all be actively managed.
Sources: Fitzpatrick's Dermatology in General Medicine (9th ed.); Andrews' Diseases of the Skin (13th ed.); Textbook of Family Medicine (9th ed.); Cochrane review PMID 37436070; EULAR 2023 guidelines PMID 38499325; EuroGuiDerm 2025.
This is a shared conversation. Sign in to Orris to start your own chat.