Acute onset painless vision loss detailed information
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute painless vision loss" AND diagnosis
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"vision loss" AND "retinal artery occlusion" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full detailed response.
Acute Onset Painless Vision Loss - Detailed Guide
Acute onset painless vision loss is a true ocular and neurological emergency. The key working principle is that sudden painless vision loss = vascular event until proven otherwise. Pain essentially rules in acute angle-closure glaucoma; its absence points to the causes below.
1. Classification Framework
| Category | Laterality | Mechanism |
|---|---|---|
| Central Retinal Artery Occlusion (CRAO) | Monocular | Arterial occlusion - ischemia |
| Branch Retinal Artery Occlusion (BRAO) | Monocular | Partial arterial occlusion |
| Central Retinal Vein Occlusion (CRVO) | Monocular | Venous stasis/thrombosis |
| Ischemic Optic Neuropathy (AION/PION) | Monocular | Optic nerve ischemia |
| Retinal Detachment | Monocular | Tractional/rhegmatogenous |
| Vitreous Hemorrhage | Monocular | Intraocular bleeding |
| Amaurosis Fugax | Monocular, transient | TIA of retina |
| Occipital/Cortical Infarct | Binocular (homonymous) | Posterior circulation stroke |
2. Central Retinal Artery Occlusion (CRAO)
Mechanism
Embolic, thrombotic, vasculitic, or vasospastic occlusion of the central retinal artery or its branches. The retina tolerates ischemia poorly - partial recovery is possible only if circulation is restored within 4 hours (primate studies); irreversible infarction likely by 6 hours.
Types
- Non-arteritic permanent - most common (~2/3 of cases); equivalent to ischemic stroke of the retina
- Non-arteritic transient - vasospasm-mediated; resembles a retinal TIA
- Arteritic - due to giant cell arteritis (GCA); the only type where pain may be present (headache/jaw claudication from GCA, not the eye itself)
Risk Factors
- Age 50-70 years
- Vascular risk factors (HTN, DM, hyperlipidemia, smoking)
- Collagen vascular disease / vasculitis
- Cardiac valvular abnormality (embolic source)
- Sickle cell disease
- Increased orbital pressure (acute glaucoma, retrobulbar hemorrhage)
- In <50 years: hypercoagulable states
Clinical Features
- Sudden, profound, painless monocular vision loss
- VA severely reduced (may be no light perception if GCA or ophthalmic artery occlusion)
- RAPD profound - sometimes a complete amaurotic pupil
- Fundoscopy:
- Pale, grey-white retinal edema in all quadrants
- Cherry-red spot at fovea - the intact choroidal circulation shines through the thin foveola against the surrounding pale ischemic retina
- Attenuated arteries with "cattle trucking" / "box-car" segmentation of blood column
- Emboli visible in ~20% (especially at bifurcation points)
- If a cilioretinal artery is present, a sector of normal-colored macula is preserved
- Over days-weeks: cloudiness and cherry-red spot disappear; arteries remain attenuated; late signs: optic atrophy, vascular sheathing, inner retinal atrophy
CRAO Fundus - Cherry-Red Spot:
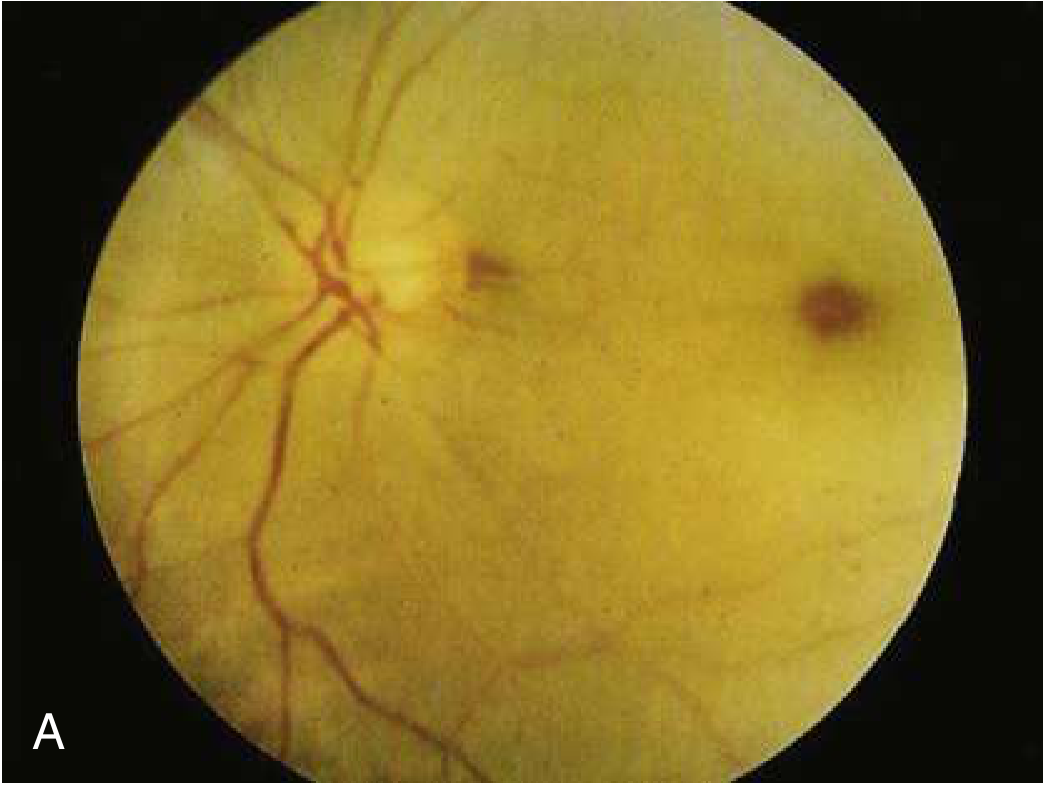
Fig. A: Acute CRAO - pale retinal whitening with a cherry-red spot. B: Later stage with less prominent cherry-red spot.
Prognosis
Poor - in two-thirds, final VA is worse than 6/120. Only one-fifth achieve 6/12 or better. Spontaneous resolution in only 1-8%.
Management (time window <6 hours)
The following can be attempted; evidence for benefit is limited:
- Ocular massage - using a three-mirror contact lens (or through closed eyelids by the patient). Positive pressure 10-15 seconds, then release, for 3-5 minutes. Aim: mechanically collapse artery lumen, cause flow changes, dislodge embolus.
- Anterior chamber paracentesis - 27-gauge needle, withdraw 0.1-0.2 mL of aqueous humor; reduces IOP and may dislodge embolus. Pre-treat with povidone-iodine 5% + topical antibiotic.
- IV thrombolysis - if <4.5 hours from onset; intra-arterial thrombolysis if <6 hours. No large RCT exists; heterogeneous evidence. Use is tailored to individual circumstances in consultation with ophthalmology.
- Hypercoagulable workup - mandated in patients <50 years.
- Cerebrovascular workup - strong association between retinal artery occlusion and subsequent ischemic stroke; expedited workup for cerebrovascular disease is recommended.
There are no established national guidelines; significant practice heterogeneity exists at academic centres - [Rosen's Emergency Medicine, p.902].
3. Branch Retinal Artery Occlusion (BRAO)
-
Symptoms: Sudden, profound painless altitudinal or sectoral visual field loss. Can go unnoticed if central vision is spared.
-
RAPD often present.
-
Fundus: Cloudy white "ground glass" retinal oedema corresponding to the ischemic area; one or more emboli visible at bifurcation points; "cattle trucking" in affected artery.
-
FA: Delayed arterial filling, hypofluorescence of involved segment.
-
Management similar to CRAO. Review at 3 months for fundus appearance and visual fields.
-
Kanski's Clinical Ophthalmology 10th Edition, p.552
4. Central Retinal Vein Occlusion (CRVO)
Mechanism
Thrombosis of the central retinal vein causes venous stasis, retinal edema, and hemorrhage. Unlike CRAO, this is a venous not arterial event.
Risk Factors
Hypertension, diabetes mellitus, hyperlipidemia, glaucoma, hypercoagulable states, vasculitides, thyroid disease (compressive), orbital tumors.
Types
- Non-ischemic CRVO: Dilatation and edema only; VA >20/200 in >80% of cases.
- Ischemic CRVO: Sudden onset painless vision loss; VA <20/200 in >90%; associated with severe complications.
Clinical Features
- Vision loss ranges from vague blurring to rapid, painless, monocular loss
- Fundoscopy: Dilated tortuous veins, diffuse retinal hemorrhages in all quadrants ("blood-and-thunder fundus"), disc edema
- Contralateral fundus is normal - this distinguishes CRVO from papilledema
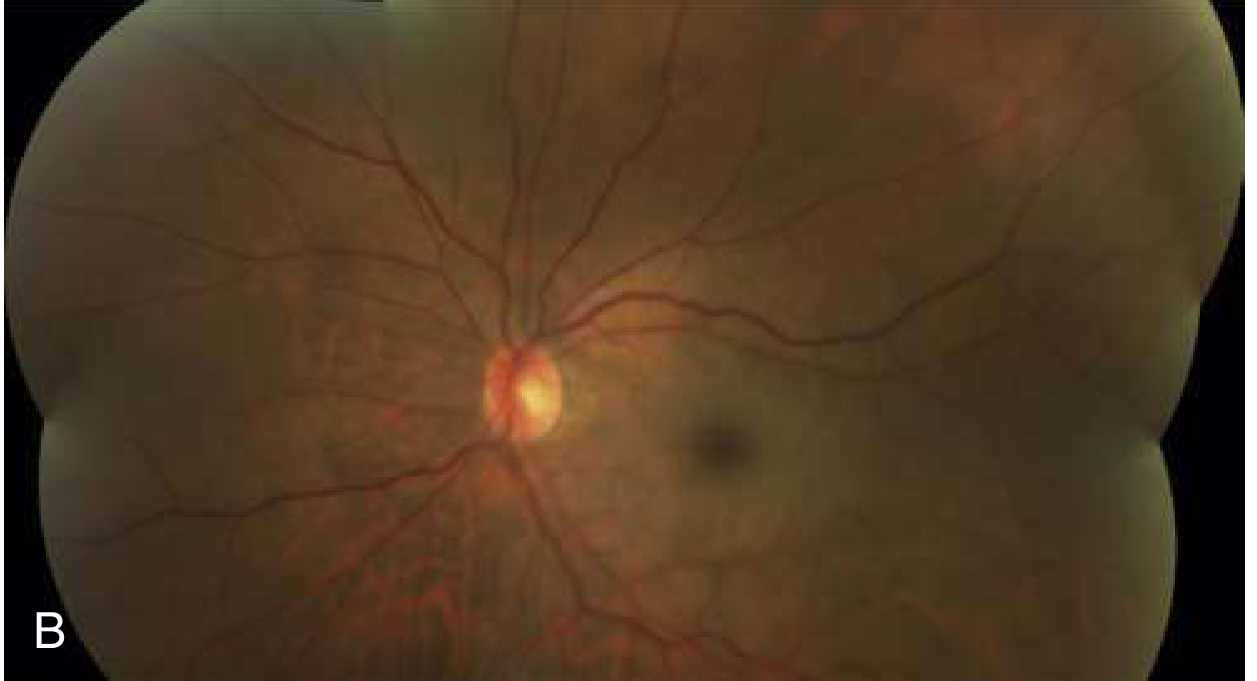
CRVO - "Blood and Thunder" Fundus:

Massive flame hemorrhages in all quadrants, tortuous dilated veins, disc edema - classic "blood and thunder" appearance.
Complications
- Neovascular glaucoma (ischemic CRVO)
- Macular edema
Management
-
Treat underlying etiology (HTN, DM, etc.)
-
Ophthalmology consult for macular edema management
-
Anti-VEGF therapy (intravitreal ranibizumab, bevacizumab)
-
Intravitreal corticosteroids
-
Retinal photocoagulation / cyclocryotherapy
-
Low-molecular-weight heparin shows promise
-
Tintinalli's Emergency Medicine; Rosen's Emergency Medicine, p.902
5. Ischemic Optic Neuropathy (ION)
Classification
| Type | Abbreviation | Cause |
|---|---|---|
| Arteritic anterior ION | A-AION | Giant cell arteritis (GCA) |
| Non-arteritic anterior ION | NA-AION | Vascular/small vessel disease |
| Posterior ION | PION | Posterior optic nerve ischemia |
A-AION (Arteritic - GCA-related)
Most serious form. Untreated, vision loss becomes bilateral in at least 50% of cases within days to weeks.
- Age typically >70 years (extremely rare <50 years)
- Associated symptoms: headache, scalp tenderness, jaw claudication, polymyalgia rheumatica, fever, malaise, weight loss
- Note: In up to 25%, acute vision loss is the only symptom - no classic GCA features
- Vision loss unilateral (46%), sequential (37%), or simultaneously bilateral (17%)
- Vision is severely reduced - hand motion or worse in ~25%
- Optic disc: Chalky-white edematous appearance with disc hemorrhages
- Concurrent cotton-wool spots on fundus are highly suggestive of A-AION
- Fluorescein angiography: Choroidal hypoperfusion (distinguishes from NA-AION)
Lab/Investigations:
- Elevated ESR (typically 70-110 mm/h in biopsy-proven cases)
- Elevated CRP (combination increases diagnostic sensitivity)
- CT angiography: 71% sensitive, 85.7% specific
- MRI: 94% sensitive, 78% specific
- Temporal artery biopsy confirms diagnosis (giant cells + endovascular inflammation)
Treatment - EMERGENCY:
- Do not wait for biopsy before starting steroids - biopsy remains valid up to 1 week after steroid initiation
- IV methylprednisolone 500 mg - 1 g daily x 3 days (admit for IV)
- Then transition to oral prednisolone
- IV steroids: 34% chance of visual improvement; reduces fellow eye involvement
- Prognosis for visual recovery in the affected eye is poor despite treatment
- Tocilizumab for steroid-resistant or steroid-intolerant patients
NA-AION (Non-arteritic)
- Most common cause of unilateral optic nerve edema in adults >50 years
- Classic risk factors: DM, HTN, obstructive sleep apnea, nocturnal hypotension
- Structural risk factor: congenitally crowded optic nerve head ("disc at risk") - small cup-to-disc ratio; swelling within scleral canal causes compartment syndrome → further ischemia
- Visual field: Altitudinal defects (respecting the horizontal midline)
- Disc: Pale, swollen with nerve fiber hemorrhages
- Moderate visual loss (less severe than A-AION)
- Spontaneous improvement in ~1/3 of patients
- No proven treatment - steroids (systemic + intravitreal) and anti-VEGF tried without success
AION - disc comparison (normal vs edematous):
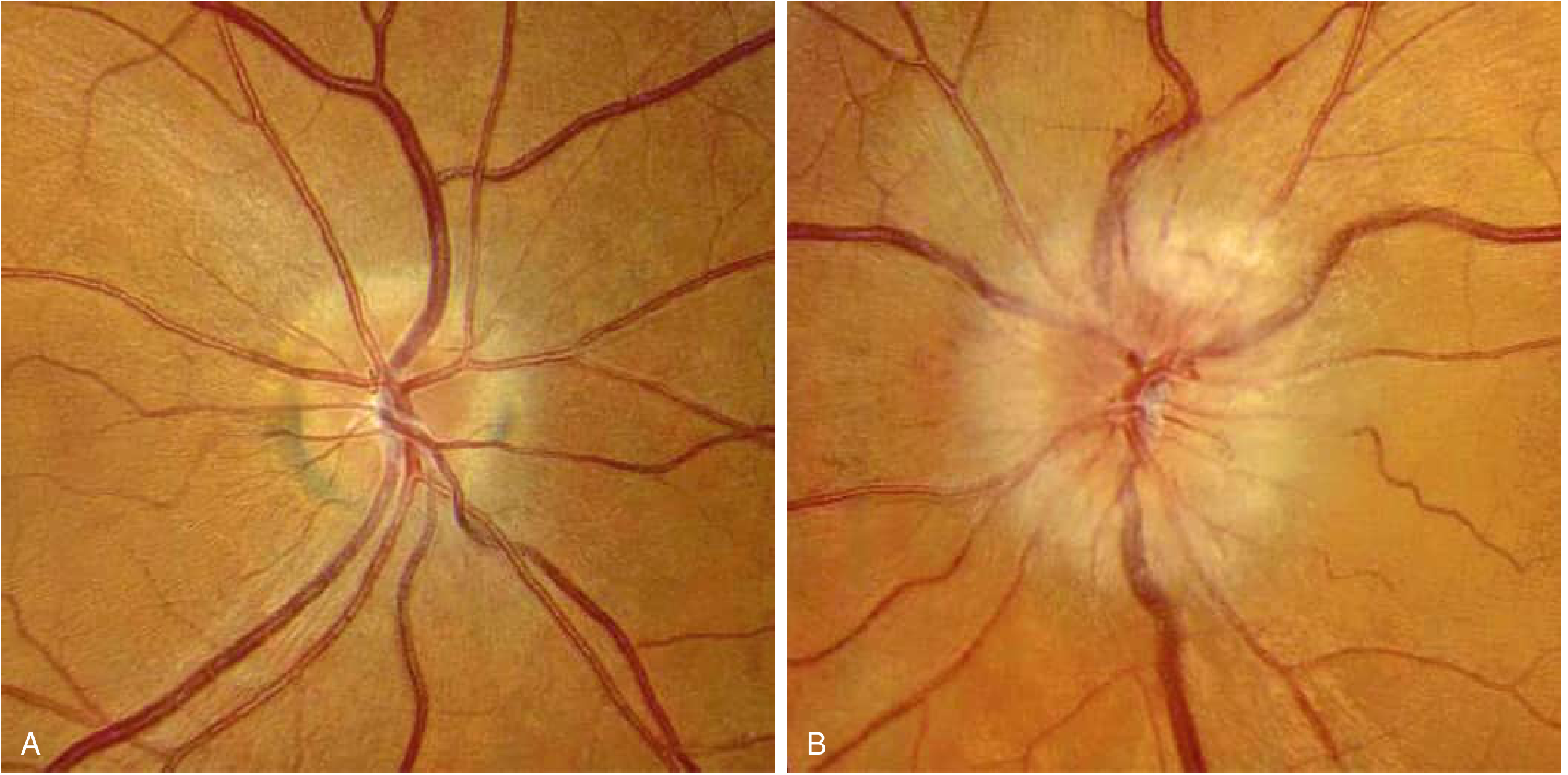
Left: normal disc, Right: pale chalky-white edematous disc in AION. Note the small cup-to-disc ratio in the "fellow eye at risk."
- Bradley and Daroff's Neurology in Clinical Practice; Rosen's Emergency Medicine, p.902
6. Retinal Detachment
-
Symptoms: Flashing lights (photopsia) and floaters preceding the vision loss; then a dark veil or curtain progressing across the visual field; decreased peripheral then central acuity
-
Monocular (binocular flashes/floaters = ophthalmic migraine)
-
Fundoscopy (dilated): Large detachment appears as a pale, billowing "parachute" - most tears are peripheral and not visible on direct fundoscopy
-
Requires dilated indirect ophthalmoscopy by ophthalmologist within 24 hours
-
Ocular ultrasound can confirm in the ED; must be verified by the ophthalmologist
-
Tintinalli's Emergency Medicine
7. Amaurosis Fugax (Transient Monocular Vision Loss)
- Transient monocular vision loss (minutes, resolves completely) - the "TIA of the retina"
- Caused by embolic or vasospastic episode in the ophthalmic/retinal circulation
- Carries significant risk of subsequent permanent vision loss or ischemic stroke
- Reported in: 2% of CRAO, 14% of BRAO, 5% of CRVO, 3% in NA-AION, 32% in GCA with ocular involvement
- Requires urgent vascular workup (carotid imaging, echo, ECG, lipids, coagulation screen)
8. Cortical/Occipital Causes (Binocular)
- Posterior circulation stroke (basilar artery territory) → sudden bilateral total blindness
- Occipital lobe infarct → sudden homonymous hemianopia (patient may report it as monocular loss on one side)
- Key differentiator: bilateral visual loss with a pupillary reflex intact (cortical blindness preserves pupil reflex as the afferent arc is intact through the midbrain, not the cortex)
9. Diagnostic Approach
History
- Monocular vs. binocular? - critical first question
- Onset, duration, progression
- Associated symptoms: pain, headache, jaw claudication, floaters, flashes, preceding TIA episodes
- Vascular risk factors, GCA symptoms
Examination
| Finding | Implication |
|---|---|
| RAPD (afferent pupillary defect) | Unilateral optic nerve/retinal disease |
| Cherry-red spot | CRAO |
| "Blood and thunder" fundus | CRVO |
| Chalky-white disc edema | A-AION (GCA) |
| Pale swollen disc, altitudinal field loss | NA-AION |
| Pale "parachute" billowing retina | Retinal detachment |
| Normal fundus | Cortical cause, PION, functional |
Investigations
- Urgent: Fundoscopy (dilated), visual acuity, visual fields, pupil responses
- Bloods: ESR, CRP (if GCA suspected); FBC, glucose, lipid profile
- If <50 years: Hypercoagulable screen (protein C, S, antithrombin III, antiphospholipid antibodies, Factor V Leiden, homocysteine)
- Imaging: CT/MRI brain (if cortical cause or uncertain diagnosis); carotid Doppler/CTA for embolic source
- Cardiac workup: Echo, ECG (embolic source)
- Temporal artery biopsy if GCA suspected
10. Disposition Summary
All patients with sudden monocular vision loss require emergent ophthalmologic evaluation. Most are admitted for further workup and management. Specific dispositions:
| Condition | Urgency | Action |
|---|---|---|
| CRAO | Within 4-6 hours | Ophthalmology + neurology; consider thrombolysis; stroke workup |
| CRVO | Same-day | Ophthalmology |
| A-AION (GCA) | Immediate - hours | Admit; IV methylprednisolone; temporal artery biopsy within 1 week |
| NA-AION | Same-day | Ophthalmology; vascular risk factor management |
| Retinal Detachment | Within 24 hours | Retina specialist; surgical repair |
| Cortical | Immediate | Neurology; stroke code if <4.5h |
Key Differentiating Points (High-Yield Summary)
| Feature | CRAO | CRVO | AION | Retinal Detachment |
|---|---|---|---|---|
| Pain | No (yes if GCA) | No | No (headache in GCA) | No |
| Laterality | Monocular | Monocular | Monocular | Monocular |
| RAPD | Profound | Moderate | Present | Variable |
| Cherry-red spot | Yes | No | No | No |
| Disc edema | No | Yes (CRVO) | Yes | No |
| Retinal hemorrhages | Rare | Diffuse ("blood-thunder") | Cotton-wool spots | No |
| Key fundus sign | Pale retina + cherry-red | Tortuous veins + hemorrhages | White edematous disc | Billowing grey retina |
| Systemic association | Stroke/emboli | HTN/DM/glaucoma | GCA/vascular risk | Myopia/aging/trauma |
Sources:
- Rosen's Emergency Medicine, Concepts and Clinical Practice, Chapter 57 (p. 900-903)
- Kanski's Clinical Ophthalmology, 10th Edition, Chapter 13 (pp. 552-554)
- Tintinalli's Emergency Medicine, Chapter 241 (pp. 1596-1598)
- Bradley and Daroff's Neurology in Clinical Practice, Chapter 16 (p. 260)
- Recent review: Bénard-Séguin et al., Handbook of Clinical Neurology 2026 - Acute retinal artery occlusions (PMID 42217977)
This is a shared conversation. Sign in to Orris to start your own chat.