Ulcer long case examination and viva
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content I need to build a thorough, exam-ready ulcer long case guide. Let me compile this into a comprehensive answer.
Ulcer - Long Case Examination & Viva Guide
(Based on S Das Manual on Clinical Surgery, Bailey & Love, and Harrison's)
DEFINITION
An ulcer is a break in the continuity of the covering epithelium (skin or mucous membrane), following either molecular death of surface epithelium or its traumatic removal.
PART 1 - HISTORY TAKING
1. Mode of Onset
- Traumatic onset: ulcer usually heals if traumatic agent is removed (e.g., dental ulcer of tongue). Chronicity if trauma persists or lies over a joint.
- Spontaneous onset: following rupture of matted tuberculous lymph nodes, gumma, or malignant growth. Varicose/ischaemic ulcers arise spontaneously. Marjolin's ulcer develops in a burn scar.
2. Duration
- Acute ulcer = shorter duration
- Chronic ulcer = persists for months or years
- Ask about incubation period when relevant: Hunterian chancre (syphilis) = 3-4 weeks; Chancroid (soft sore) = 3-4 days
3. Pain
- Acutely inflamed ulcers: exquisitely painful
- Syphilitic/trophic ulcers: painless (tabes dorsalis, transverse myelitis, peripheral neuritis)
- Tuberculous ulcers: slightly painful
- Malignant ulcers (epithelioma, BCC): absolutely painless initially; only become painful when infiltrating pain-fibre-rich structures
- Varicose ulcers: may or may not be painful
4. Discharge
- Character, amount, smell
- Scanty serous: healing ulcer
- Purulent: spreading or inflamed ulcer
- Sero-sanguineous: tuberculous or malignant ulcer
- Greenish: B. pyocyanea (Pseudomonas) infection
- Always take a bacteriological swab
5. Progress
- Getting better, worse, or static?
- Has the patient had treatment before? What type?
6. Associated symptoms
- Fever, weight loss, night sweats (TB, malignancy)
- Claudication, rest pain (ischaemic ulcer)
- Leg swelling, heaviness (varicose ulcer)
- Tingling, numbness, weakness (neuropathic ulcer)
- Urethral discharge, genital lesion, rash (syphilitic ulcer)
7. Past history
- Diabetes mellitus, hypertension, peripheral vascular disease
- TB, syphilis, leprosy
- Prior burns, trauma, radiation
- Drug history
8. Social history
- Occupation, travel history (tropical ulcer, yaws), sexual history (STI)
PART 2 - PHYSICAL EXAMINATION
A. GENERAL EXAMINATION
Do not focus only on the ulcer. A proper general examination is mandatory.
- Nutritional status: anaemia (pale conjunctiva), cachexia - suggest malignancy or TB
- Jaundice: hepatic metastases
- Lymphadenopathy: all regional and distant nodes
- Diabetes signs: xanthelasma, diabetic retinopathy (fundoscopy)
- Cardiovascular: peripheral pulses for ischaemic ulcer
- Neurological: sensory deficit, motor deficit for neuropathic ulcer
- Chest: TB focus, metastatic deposits
B. LOCAL EXAMINATION OF THE ULCER
On INSPECTION - examine each anatomical part systematically:
| Part | What to Note | Significance |
|---|---|---|
| Site | Anatomical location; pressure points, gaiter area, genitalia | Guides aetiology |
| Size | cm x cm | Extent of disease |
| Shape | Round, oval, irregular | Helps in typing |
| Number | Single or multiple | TB/syphilis often multiple |
| Edge | See below - 6 types | Most important diagnostic feature |
| Floor | What covers it | Healing status |
| Discharge | Character (see above) | Inflammation, infection type |
| Surrounding skin | Glossy, red, oedematous; eczematous/pigmented; scarred | Varicose, acute, TB |
The 6 TYPES OF EDGE (MOST IMPORTANT FOR VIVA):
- Sloping/shelving edge - found in healing ulcers; one side shows new epithelium growing over
- Punched-out edge - edges are vertical, like a hole punched in skin; seen in trophic/neuropathic ulcers (also syphilitic gumma)
- Undermined edge - edge overhangs the floor; seen in tuberculous ulcers and pressure sores
- Rolled/everted edge - edges rolled outward exposing floor; seen in squamous cell carcinoma (epithelioma)
- Raised/heaped-up edge - raised, everted, irregular proliferative edge; seen in basal cell carcinoma (rodent ulcer)
- Indurated/hard edge - indurated edge; seen in carcinoma (SCC or adenocarcinoma) and hard chancre (primary syphilis)
Floor of the Ulcer:
- Red granulation tissue = healthy, healing ulcer
- Pale, smooth granulation = slowly healing
- Wash-leather slough (wet chamois leather appearance) = pathognomonic of gummatous ulcer (tertiary syphilis)
- Penetrating to bone = trophic ulcer
- Black mass = malignant melanoma
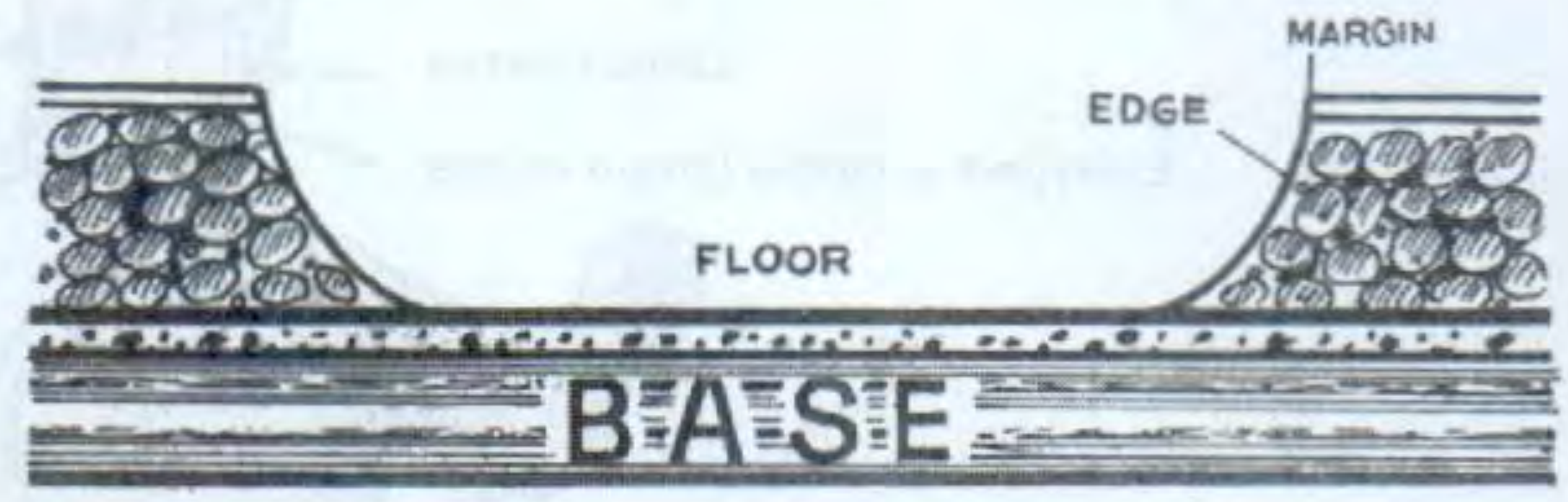
Anatomical parts of an ulcer: MARGIN = junction of normal skin with ulcer boundary; EDGE = area between margin and floor; FLOOR = exposed surface; BASE = tissue deep to the floor
On PALPATION - examine each part:
| Parameter | Findings | Significance |
|---|---|---|
| Tenderness | Exquisite = acute inflammation; slight = TB/syphilis; none = neoplastic; variable = varicose | Guides type |
| Edge & Margin | Induration = chronic or malignant | Induration pathognomonic of carcinoma |
| Floor | Note depth, what it lies on | Bone involvement in trophic |
| Base | Hard, soft, indurated | Hard = carcinoma or syphilitic chancre |
| Temperature | Warm = inflamed/ischaemic; cool = venous stasis | |
| Mobility | Fixed to underlying structures | Malignant infiltration |
| Regional lymph nodes | Tender, hard, matted, mobile | Infection vs. malignancy |
Lymph node findings by diagnosis:
- TB: enlarged, non-tender, matted (characteristic)
- Syphilitic chancre: enlarged, mobile, firm, discrete, non-tender, no suppuration
- Carcinoma: hard, may be fixed, irregular
- Acute infection: tender, soft (suppurated)
GENERAL (WHOLE LIMB) EXAMINATION:
- Look for varicose veins in the upper limb/leg - varicose ulcer
- Arterial pulses (femoral, popliteal, PT, DP) - ischaemic ulcer; always examine both limbs (Buerger's is bilateral)
- Neurological examination - sensory (light touch, proprioception, vibration), motor - trophic ulcer
- Atherosclerosis elsewhere - bruits, fundoscopy changes
- Skin over whole limb - pigmentation, lipodermatosclerosis, atrophie blanche (venous)
PART 3 - SPECIAL INVESTIGATIONS
| Investigation | When/Why |
|---|---|
| FBC, ESR | Always; lymphocytosis + high ESR = TB; anaemia in malignancy |
| Blood sugar | Exclude DM in all chronic ulcers |
| VDRL/TPHA (WR, Kahn) | Exclude syphilis |
| Urine sugar | Exclude DM |
| Bacteriology swab + C&S | Inflamed/spreading ulcers; antibiotic sensitivity |
| Dark-field microscopy | Serous discharge of hard chancre - demonstrate T. pallidum |
| AFB smear + guinea pig inoculation | Tuberculous ulcer discharge |
| Mantoux test | TB - positive in children, used to exclude in adults |
| Chest X-ray | TB (primary focus); malignant (lung metastases) |
| Biopsy (from edge) | Malignant ulcer - always from edge including surrounding healthy skin; for histology and staging |
| X-ray bone/joint | Near bone; gumma causes new bone formation and "sabre tibia" |
| Arteriography | Ischaemic/arterial ulcer |
| Ascending phlebography | DVT in venous ulcer |
| Radioactive fibrinogen (125I) | Detecting DVT (90% accuracy) |
| Doppler/duplex | Venous and arterial insufficiency |
| Ankle-Brachial Index (ABI) | ≤0.9 = arterial insufficiency; <0.5 = critical ischaemia |
PART 4 - TYPES OF ULCERS (DIFFERENTIAL DIAGNOSIS)
1. Healing (Simple) Ulcer
- Sloping edge, red granulation tissue floor, serous discharge
- Progressing toward healing; no induration
2. Tuberculous Ulcer
- Site: neck, axilla, groin (from ruptured caseous lymph nodes)
- Edge: thin, reddish-blue, undermined (pathognomonic)
- Floor: pale granulation tissue
- Discharge: scanty, sero-sanguineous
- Base: slight induration
- Lymph nodes: enlarged, non-tender, matted
- Pain: slightly painful
3. Syphilitic Ulcers
- (i) Hard chancre (primary) - external genitalia, coronal sulcus; painless, indurated base (feels like a button); lymph nodes: mobile, firm, discrete, non-tender, no suppuration
- (ii) Gummatous ulcer (tertiary) - leg/scalp; punched-out edge; wash-leather slough on floor; painless
- (iii) Secondary syphilis - "snail-track ulcers" in mouth (mucous patches coalescencing)
4. Varicose (Venous) Ulcer
- Site: gaiter area (medial malleolus region of leg)
- Edge: sloping
- Surrounding skin: eczematous, pigmented, lipodermatosclerosis
- Varicose veins present
- Pain: variable; often aching, relieved by elevation
- ABI normal (>0.9)
5. Ischaemic/Arterial Ulcer
- Site: tips of toes, heel, pressure points
- Edge: punched-out
- Surrounding skin: cold, pale/cyanosed, atrophic, hairless
- Pain: severe, worse at night and with elevation; claudication history
- Pulses: absent or reduced
- ABI <0.9; <0.5 = critical ischaemia
- Causes: atherosclerosis, Buerger's disease, Raynaud's
6. Trophic/Neuropathic Ulcer (Perforating Ulcer)
- Site: pressure points on the sole (1st and 5th MTH, heel); areas of anaesthesia
- Edge: punched-out; callous surrounding skin
- Floor: may reach bone
- Pain: painless (anaesthesia)
- Associated: neurological signs (loss of vibration, proprioception, reflexes)
- Causes: DM peripheral neuropathy, tabes dorsalis, leprosy, transverse myelitis, syringomyelia
7. Malignant Ulcer (Epitheliomatous/SCC)
- Edge: everted/rolled; hard indurated base
- Floor: irregular, bleeds easily
- Discharge: sero-sanguineous, offensive
- Pain: initially painless
- Lymph nodes: hard, irregular, may be fixed
- Marjolin's ulcer: SCC in burn scar; slow-growing, little metastasis
- Requires biopsy from edge
8. Basal Cell Carcinoma (Rodent Ulcer)
- Site: sun-exposed areas (face, especially near eye, nose, ear)
- Edge: raised, pearly, "rolled" with telangiectasia
- Never metastasises (locally destructive only)
- Slow-growing; victims are old people with outdoor exposure
9. Tropical Ulcer
- Cause: Vincent's organisms (Bacteroides fusiformis) from trauma/insect bite
- Site: lower limb
- Edge: undermined, raised
- Discharge: copious sero-sanguineous; very painful acutely
- Can become chronic, may undergo squamous cell carcinoma change
10. Chancroid (Soft Sore)
- Cause: Haemophilus ducreyi; incubation 3-4 days
- Multiple, painful, soft ulcers on genitalia
- Contrast with syphilitic chancre (painless, hard, single, incubation 3-4 weeks)
PART 5 - VIVA QUESTIONS & MODEL ANSWERS
Q: Define an ulcer.
A: A break in the continuity of the covering epithelium - skin or mucous membrane - due to molecular death or traumatic removal of surface epithelium.
Q: What are the anatomical parts of an ulcer?
A: Margin (boundary between normal skin and ulcer), Edge (area between margin and floor), Floor (the exposed base surface), and Base (tissue lying deep to the floor).
Q: What is the most important diagnostic feature of an ulcer?
A: The edge - its character is most informative for diagnosis.
Q: Name the 6 types of edges.
A: (1) Sloping/shelving - healing ulcer; (2) Punched-out - trophic/gummatous; (3) Undermined - tuberculous; (4) Everted/rolled - SCC (epithelioma); (5) Raised/heaped - BCC (rodent ulcer); (6) Indurated - carcinoma.
Q: What is the pathognomonic feature of a gummatous ulcer?
A: Wash-leather slough (wet chamois leather appearance) on the floor.
Q: Differentiate hard chancre from soft sore (chancroid).
| Feature | Hard Chancre (Syphilis) | Soft Sore (Chancroid) |
|---|---|---|
| Cause | T. pallidum | H. ducreyi |
| Incubation | 3-4 weeks | 3-4 days |
| Pain | Painless | Very painful |
| Edge/base | Indurated, button-like | Soft, undermined |
| Lymph nodes | Firm, non-tender, no suppuration | Tender, may suppurate (bubo) |
| Number | Usually single | Multiple |
Q: What is Marjolin's ulcer?
A: A squamous cell carcinoma developing in the scar of a chronic burn wound or chronic ulcer (e.g., scar from lupus vulgaris). It is slow-growing with little tendency to metastasise. Characterised by an everted edge and indurated base.
Q: What are the causes of a painless ulcer?
A: Syphilitic ulcers, trophic/neuropathic ulcers (tabes dorsalis, leprosy, DM neuropathy), malignant ulcers (initially), and BCC (rodent ulcer).
Q: Why is biopsy taken from the edge (not the centre) of an ulcer?
A: Activity is maximum at the edge and margin; the centre often contains necrotic tissue. The edge biopsy includes a portion of surrounding healthy tissue, providing maximum diagnostic yield for histology and invasion assessment.
Q: What investigation helps diagnose deep vein thrombosis in venous ulcer?
A: Radioactive fibrinogen test using 125I-labelled fibrinogen (90% accuracy), ascending functional phlebography, and duplex ultrasonography.
Q: What is the ABI threshold for arterial ulcer?
A: ABI ≤0.9 indicates arterial insufficiency. ABI <0.5 indicates critical limb ischaemia. Compression bandaging is contraindicated if ABI <0.8.
Q: What are causes of non-healing of an ulcer?
A: (Causes of chronicity)
- Persisting aetiological factor (poor arterial supply, uncontrolled DM, continued trauma, venous hypertension)
- Secondary infection
- Malignant change
- Nutritional deficiency
- Ischaemia
- Foreign body
- Specific infection (TB, syphilis, actinomycosis) not being treated
- Steroid use
Q: What is a trophic ulcer?
A: Also called a perforating/neuropathic ulcer. It occurs over pressure points in anaesthetic areas due to loss of protective pain sensation. The floor may penetrate to bone. Causes include diabetes, tabes dorsalis, leprosy, syringomyelia, and peripheral neuropathy.
PART 6 - TREATMENT PRINCIPLES
General Principles:
- Treat the cause (most important step)
- Control DM (blood sugar optimisation)
- Improve venous drainage (elevation, compression)
- Restore arterial supply (revascularisation)
- Treat TB/syphilis with appropriate chemotherapy
- Remove offending trauma/foreign body
- Local wound care (ulcer care):
- Wound debridement: remove slough and necrotic tissue
- Dressings: moist wound healing (hydrocolloid, alginate, foam)
- Bacteriology-guided antibiotics if infected
- Maggot therapy for debridement of necrotic tissue
- Surgical options:
- Skin grafting (split-thickness graft) once ulcer bed is clean with healthy granulation tissue
- Excision + grafting for malignant ulcers
- Varicose vein surgery/stripping for venous ulcers
- Arterial bypass/angioplasty for ischaemic ulcers
- Amputation in critical ischaemia unresponsive to revascularisation
SUMMARY MNEMONICS
For Edge types - "Should Punch Under Every Real Incision":
- Sloping - healing
- Punched-out - trophic/gumma
- Undermined - TB
- Everted - SCC
- Raised (heaped) - BCC
- Indurated - carcinoma
For Painless ulcers - "STM":
- Syphilitic
- Trophic
- Malignant (early)
For TB ulcer - "Undermined, Matted, Pale, Serosanguineous" - UMaPS
Sources: S Das Manual on Clinical Surgery 13th Ed, Chapter 4 (Ulcer); Bailey & Love's Short Practice of Surgery 28th Ed; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.