Practical file - Trauma management surgery
Asking for Preferences
I wanted a topic, trauma management, in which the first topic is CPR, because I have to make an assignment on it. So please give the material according to that.
Reading File
Finding Sources
Finding Sources
Searching the Web
CPR cardiopulmonary resuscitation trauma management 2024 guidelines steps
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material. Let me compile the full assignment.
Trauma Management - Practical Assignment
Topic 1: Cardiopulmonary Resuscitation (CPR)
1. Introduction
Trauma is one of the leading causes of death worldwide, and cardiopulmonary arrest is one of its most catastrophic consequences. Cardiopulmonary Resuscitation (CPR) is a life-saving emergency procedure that combines chest compressions with rescue breathing to manually preserve brain function and cardiac output until spontaneous circulation is restored or advanced care is available.
CPR should be considered any time an individual cannot adequately oxygenate or perfuse vital organs - not only following cardiac or respiratory arrest. In the trauma setting, early and effective CPR can bridge the gap between injury and definitive surgical management.
2. Definition
CPR (Cardiopulmonary Resuscitation) is an emergency procedure performed on a person who has suffered cardiac arrest (cessation of effective heart pumping) and/or respiratory arrest (cessation of breathing). It involves the combined use of:
- External chest compressions - to maintain artificial circulation
- Rescue breathing (mouth-to-mouth or bag-valve-mask) - to maintain oxygenation
3. Indications for CPR
CPR should be initiated when a patient presents with:
- Unresponsiveness
- Absent or agonal (gasping) breathing
- Absent carotid pulse (check for no more than 10 seconds)
- Cardiac arrest from any cause (trauma, myocardial infarction, drowning, electrocution, etc.)
In traumatic cardiac arrest, CPR is appropriate when the patient had signs of life immediately before arrest, or when the cause is potentially reversible (tension pneumothorax, cardiac tamponade, hypovolemia).
4. The Chain of Survival
The American Heart Association (AHA) identifies five critical links:
| Link | Action |
|---|---|
| 1 | Early recognition and activation of emergency response |
| 2 | Early high-quality CPR |
| 3 | Early defibrillation |
| 4 | Advanced resuscitation (ACLS) |
| 5 | Post-cardiac arrest care |
5. CPR Sequence - CAB Protocol (AHA 2020 Guidelines)
The sequence was changed from the older ABC (Airway - Breathing - Compressions) to CAB (Compressions - Airway - Breathing) in the 2010 AHA guidelines and reaffirmed in 2020. This is because during cardiac arrest, oxygen delivery to the heart and brain is limited by blood flow rather than arterial oxygen content - hence compressions take priority.
Step-by-Step CPR Protocol
Step 1 - Scene Safety
Ensure the environment is safe for both the rescuer and the victim before approaching.
Step 2 - Check Responsiveness
Tap the patient's shoulders firmly and shout "Are you okay?" Check for no longer than 10 seconds.
Step 3 - Activate Emergency Response
Call for help, activate the emergency response system (call 108/emergency number), and send someone to retrieve an AED (Automated External Defibrillator).
Step 4 - Check for Breathing and Pulse (simultaneously, <10 seconds)
- Look for chest rise
- Check carotid pulse
- Absence of both = initiate CPR immediately
6. Chest Compressions (C - Circulation)
Technique:
- Position: Patient flat/supine on a firm surface
- Hand placement: Heel of one hand on the lower half of the sternum (center of the chest), second hand on top, fingers interlaced
- Compression depth: At least 5 cm (2 inches) in adults; avoid exceeding 6 cm (2.4 inches)
- Rate: 100-120 compressions per minute
- Full chest recoil: Allow complete recoil between compressions (do not lean on the chest)
- Minimize interruptions: Keep interruptions to less than 10 seconds
Compression-to-Ventilation Ratio:
- Without advanced airway: 30 compressions : 2 breaths (30:2)
- With advanced airway (ETT): Continuous compressions at 100-120/min + 8-10 breaths/min (asynchronous)
- Rotate compressors every 2 minutes to avoid fatigue
- One cycle = 30 compressions + 2 breaths; 5 cycles = approximately 2 minutes
7. Airway Management (A - Airway)
The airway is most commonly obstructed by posterior displacement of the tongue or epiglottis.
Techniques:
1. Head-Tilt Chin-Lift (first-line, if no cervical spine injury suspected)
- Place one palm on the forehead to tilt the head back
- Lift the chin upward with two fingers of the opposite hand
2. Jaw Thrust (preferred when cervical spine injury is suspected - common in trauma)
- Place both hands on either side of the patient's head
- Grasp the angles of the jaw and lift forward
- This opens the airway without neck extension
In trauma patients, always assume a cervical spine injury until proven otherwise. Use the jaw thrust in preference to head-tilt chin-lift.
8. Breathing / Rescue Breaths (B - Breathing)
- Deliver 2 rescue breaths after every 30 compressions (if no advanced airway)
- Each breath should last 1 second and produce visible chest rise
- Avoid excessive ventilation (hyperventilation decreases venous return and cardiac output)
- Use a bag-valve-mask (BVM) with supplemental O2 when available
- Confirm ETT placement with waveform capnography (gold standard)
Targets during CPR:
| Parameter | Target |
|---|---|
| PETCO2 (end-tidal CO2) | >10 mmHg |
| Arterial diastolic BP | >20 mmHg |
| Central venous O2 saturation (ScvO2) | >30% |
9. Defibrillation (D - Defibrillation)
Attach the AED/defibrillator as soon as it is available.
Shockable vs Non-Shockable Rhythms:
| Shockable | Non-Shockable |
|---|---|
| Ventricular Fibrillation (VF) | Pulseless Electrical Activity (PEA) |
| Pulseless Ventricular Tachycardia (pVT) | Asystole |
- Biphasic shock: Device-specific dose (typically 120-200 J); if unknown, use 200 J
- Resume CPR immediately after shock delivery
- Minimize the pre-shock pause (time from last compression to shock delivery)
CPR Algorithm (ACLS):
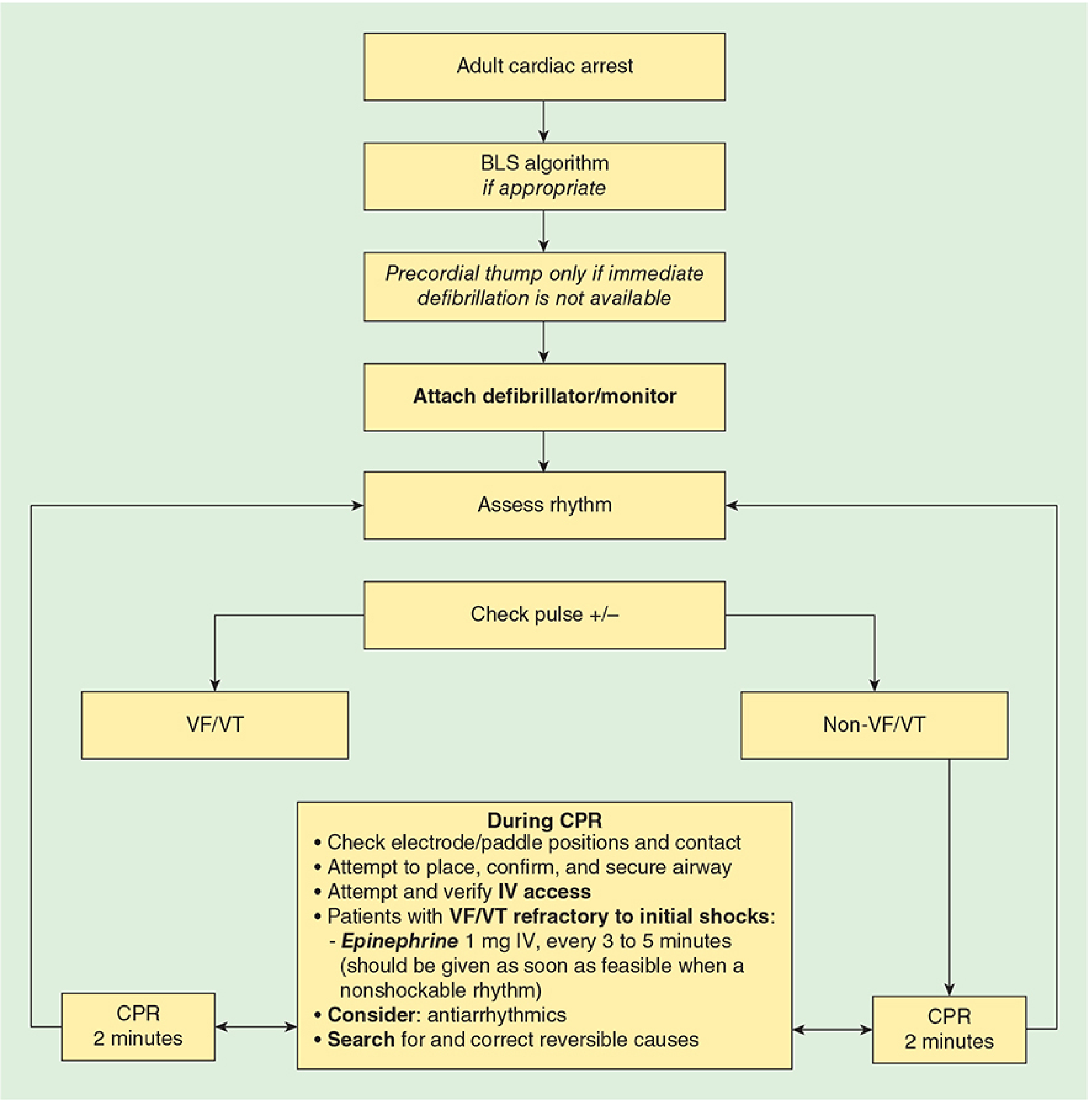
10. Pharmacotherapy During CPR
Key Drugs (AHA 2020):
| Drug | Dose | Indication |
|---|---|---|
| Epinephrine (Adrenaline) | 1 mg IV/IO every 3-5 min | All cardiac arrest rhythms (give as soon as feasible in non-shockable) |
| Amiodarone | 300 mg IV/IO (first dose); 150 mg (second dose) | VF/pVT refractory to shocks |
| Lidocaine | 1-1.5 mg/kg IV (first dose); 0.5-0.75 mg/kg (repeat, max 3 doses/3 mg/kg) | Alternative to amiodarone |
| Magnesium Sulfate | 1-2 g IV/IO loading dose | Torsades de Pointes |
Note: Vasopressin alone or combined with epinephrine offers no advantage over standard-dose epinephrine and has been removed from the AHA algorithm.
11. Reversible Causes - The "H's and T's"
During CPR, always search for and treat reversible causes:
| H's | T's |
|---|---|
| Hypovolemia | Tamponade (cardiac) |
| Hypoxia | Tension pneumothorax |
| Hydrogen ion (acidosis) | Thrombosis (pulmonary embolism) |
| Hypo/Hyperkalemia | Thrombosis (coronary - MI) |
| Hypoglycemia | Toxins/drugs |
| Hypothermia | Trauma |
In trauma, the most common reversible causes are: hypovolemia (hemorrhage), tension pneumothorax, cardiac tamponade, and hypoxia - all of which must be identified and corrected during resuscitation.
12. CPR in Trauma - Special Considerations
Traumatic cardiac arrest has unique features that differ from medical cardiac arrest:
- Hemorrhagic shock is the most common cause - aggressive hemorrhage control (tourniquets, direct pressure) must accompany CPR
- Tension pneumothorax - requires immediate needle decompression (2nd intercostal space, mid-clavicular line)
- Cardiac tamponade - requires emergency pericardiocentesis or resuscitative thoracotomy
- Airway obstruction - secured with jaw thrust first; definitive airway (ETT) as soon as possible
- Cervical spine protection must be maintained throughout
Resuscitative Thoracotomy:
In penetrating trauma with witnessed arrest, emergency department thoracotomy may be indicated to:
- Relieve tamponade
- Control intrathoracic hemorrhage
- Perform open cardiac massage
When to Withhold/Terminate CPR in Trauma:
- Obviously unsurvivable injury (decapitation, hemicorporectomy, rigor mortis)
- Blunt trauma arrest with no signs of life on EMS arrival and no organized rhythm
- Resuscitation limited to 30 minutes if the traumatic event was unwitnessed and prolonged hypoxia is assumed
13. Post-Resuscitation Care (Return of Spontaneous Circulation - ROSC)
Once ROSC is achieved:
| Intervention | Goal |
|---|---|
| 12-lead ECG | Identify STEMI for cath lab activation |
| Targeted temperature management (TTM) | 32-36°C for 24 hours (comatose patients) |
| Oxygen titration | SpO2 94-98% (avoid hyperoxia) |
| CO2 management | PaCO2 35-45 mmHg (avoid hyperventilation) |
| Blood pressure support | MAP >65 mmHg |
| CT scan | Identify treatable injuries |
14. Basic Life Support (BLS) vs Advanced Cardiac Life Support (ACLS)
| Feature | BLS | ACLS |
|---|---|---|
| Training level | Layperson / first responder | Healthcare professionals |
| Equipment | Minimal (hands, BVM, AED) | Full equipment, drugs, ETT |
| Chest compressions | Yes (30:2) | Yes (continuous with ETT) |
| Defibrillation | AED | Manual defibrillator |
| Drugs | No | Yes (epinephrine, amiodarone) |
| Airway | Head-tilt/jaw-thrust, BVM | ETT, LMA, surgical airway |
15. Pediatric CPR - Key Differences
| Parameter | Adult | Child (1-8 yrs) | Infant (<1 yr) |
|---|---|---|---|
| Compression depth | 5-6 cm | 5 cm (1/3 chest) | 4 cm (1/3 chest) |
| Compression rate | 100-120/min | 100-120/min | 100-120/min |
| Ratio (1 rescuer) | 30:2 | 30:2 | 30:2 |
| Ratio (2 rescuers) | 30:2 | 15:2 | 15:2 |
| Hand technique | 2 hands | 1-2 hands | 2 fingers / 2-thumb |
| Initial breaths | No (CAB) | 5 rescue breaths first (ABC) | 5 rescue breaths first (ABC) |
| Defibrillation | 200 J biphasic | 2 J/kg (max 4 J/kg) | 2 J/kg |
16. Summary
| Key Point | Value |
|---|---|
| Compression rate | 100-120 per minute |
| Compression depth (adult) | At least 5 cm (not >6 cm) |
| C:V ratio (no advanced airway) | 30:2 |
| Pulse check duration | <10 seconds |
| Compression interruption limit | <10 seconds |
| First drug (all rhythms) | Epinephrine 1 mg IV/IO every 3-5 min |
| AED shock (unknown dose) | 200 J biphasic |
| Sequence (AHA 2020) | CAB (not ABC) |
References
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition - Chapter 55: CPR (AHA 2020 Guidelines), pp. 2378-2385
- The Washington Manual of Medical Therapeutics - ACLS Pulseless Arrest Algorithm, p. 1130
- Bailey and Love's Short Practice of Surgery, 28th Edition - Chapter 26: The Management of Trauma, pp. 365-370
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Primary Survey & CPR
- AHA 2020 Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S366-S468
- AHA 2025 Guidelines for CPR and Emergency Cardiovascular Care (latest update)
This covers all the major content areas you need for a comprehensive CPR assignment within trauma management. The key themes to emphasize are: the CAB sequence, high-quality compressions (rate + depth + recoil), the H's and T's, and trauma-specific modifications (jaw thrust for c-spine, treating tension pneumothorax and tamponade alongside CPR). Let me know if you want me to expand any section, add diagrams, or format this as a Word document or PDF for submission.
This is a shared conversation. Sign in to Orris to start your own chat.