Treatment of stage 4 stomach
Reading File
Finding Sources
Searching PubMed
"gastric cancer" AND "stage IV" AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Searching the Web
stage 4 gastric cancer treatment 2025 guidelines nivolumab zolbetuximab
Reading File
Searching the Web
metastatic gastric cancer first-line treatment NCCN 2025 CheckMate nivolumab
Here is a structured, evidence-based overview of the treatment of Stage IV (metastatic) gastric cancer (Stage IVB).
Stage IV Gastric Cancer - Treatment Overview
Stage IVB is defined by distant metastasis (M1). It is generally not curable, and treatment goals are palliative: to prolong survival, control symptoms, and maintain quality of life. With best supportive care alone, median survival is only about 5 months. Systemic therapy meaningfully extends this.
Staging Reminder (TNM)
- Stage IVA: T4b, any N, M0 (locally unresectable)
- Stage IVB: Any T, any N, M1 (distant metastasis - e.g., liver, peritoneum, lungs, distant lymph nodes)
- Washington Manual of Medical Therapeutics, p. 844
1. Biomarker Testing - Required Before Treatment
Before starting systemic therapy, tissue must be tested for:
| Biomarker | Test | Relevance |
|---|---|---|
| HER2 | IHC ± FISH | Targets trastuzumab use |
| PD-L1 | CPS (Combined Positive Score) | Guides ICI eligibility |
| MSI/MMR | PCR or IHC | MSI-H responds well to immunotherapy; does NOT respond to conventional chemo |
| EBV status | ISH | EBV+ tumors are highly immunotherapy-responsive |
| NTRK fusion | NGS | Eligible for TRK inhibitors |
| RET fusion | NGS | Eligible for selpercatinib |
| BRAF V600E | Molecular testing | Eligible for dabrafenib + trametinib |
- Sabiston Textbook of Surgery, p. 1809
2. First-Line Systemic Therapy
A) HER2-Negative Tumors
Standard backbone: Platinum (cisplatin or oxaliplatin) + fluoropyrimidine (5-FU or capecitabine)
- Common regimens: FOLFOX (5-FU, leucovorin, oxaliplatin), CAPOX (capecitabine + oxaliplatin), FLOT (docetaxel + oxaliplatin + leucovorin + 5-FU)
+ Immunotherapy (checkpoint inhibitor):
- Nivolumab (anti-PD-1) added to chemotherapy is FDA-approved for first-line treatment in patients with CPS ≥ 1 (CheckMate-649 trial showed improved OS)
- Pembrolizumab + chemotherapy is approved for HER2-negative metastatic gastric cancer (KEYNOTE-859 trial)
- ASCO guidelines recommend ICI + chemo for CPS ≥ 5; individualized approach for CPS 1-4; chemotherapy alone for CPS 0
B) HER2-Positive Tumors (IHC 3+ or IHC 2+/FISH+)
- Trastuzumab + platinum/fluoropyrimidine is standard of care (ToGA trial: median OS 13.8 months vs. 11 months with chemo alone)
- Adding nivolumab to trastuzumab + chemo is an emerging option
- Sabiston Textbook of Surgery, p. 1747
C) MSI-High / dMMR Tumors
- These tumors do not respond to conventional cytotoxic chemotherapy
- Checkpoint blockade (pembrolizumab, nivolumab) has high response rates
- MSI-H gastric cancer should be considered for upfront immunotherapy-based treatment
- Sabiston Textbook of Surgery, p. 1809
3. Second-Line and Beyond
| Agent | Mechanism | Indication |
|---|---|---|
| Ramucirumab (REGARD trial) | Anti-VEGFR monoclonal antibody | After failure of first-line platinum/fluoropyrimidine |
| Ramucirumab + paclitaxel | Anti-VEGFR + taxane | Second-line (RAINBOW trial) |
| Trastuzumab deruxtecan (T-DXd) | HER2-directed antibody-drug conjugate | HER2+ after prior trastuzumab - FDA approved (median OS 12.5 vs 8.4 months) |
| Irinotecan | Topoisomerase inhibitor | Second/third line |
| Docetaxel / paclitaxel | Taxane | Second/third line |
| Pembrolizumab (MSI-H) | Anti-PD-1 | Any line in MSI-H tumors |
- Sabiston Textbook of Surgery, p. 1747; Schwartz's Principles of Surgery, p. 58
4. Targeted Therapies for Rare Molecular Subsets
- NTRK fusion: Larotrectinib or entrectinib (tumor-agnostic FDA approval)
- RET fusion: Selpercatinib
- BRAF V600E: Dabrafenib + trametinib
- Sabiston Textbook of Surgery, p. 1589
5. Palliative / Supportive Measures
- Bleeding: Endoscopic coagulation; external beam radiation or angiographic embolization for refractory cases
- Gastric outlet obstruction: Endoscopic stenting (preferred) or surgical gastrojejunostomy; venting gastrostomy
- Palliative gastrectomy: Selectively for distal tumors to improve quality of life (total gastrectomy generally avoided as palliative due to high complication risk)
- Nutritional support: Jejunal feeding tube or gastrostomy if oral intake is inadequate
- Peritoneal disease (in ~50%): Staging laparoscopy for assessment; HIPEC is under investigation in trials
- Current Surgical Therapy 14e, p. 103-106
6. Conversion Surgery (Selected Patients)
A 2025 systematic review (PMID 40696068) found that conversion surgery (resection after good response to systemic therapy in initially unresectable Stage IV disease) is associated with improved outcomes versus continuing systemic therapy alone in carefully selected patients. This is a promising but not yet standard strategy.
Prognosis
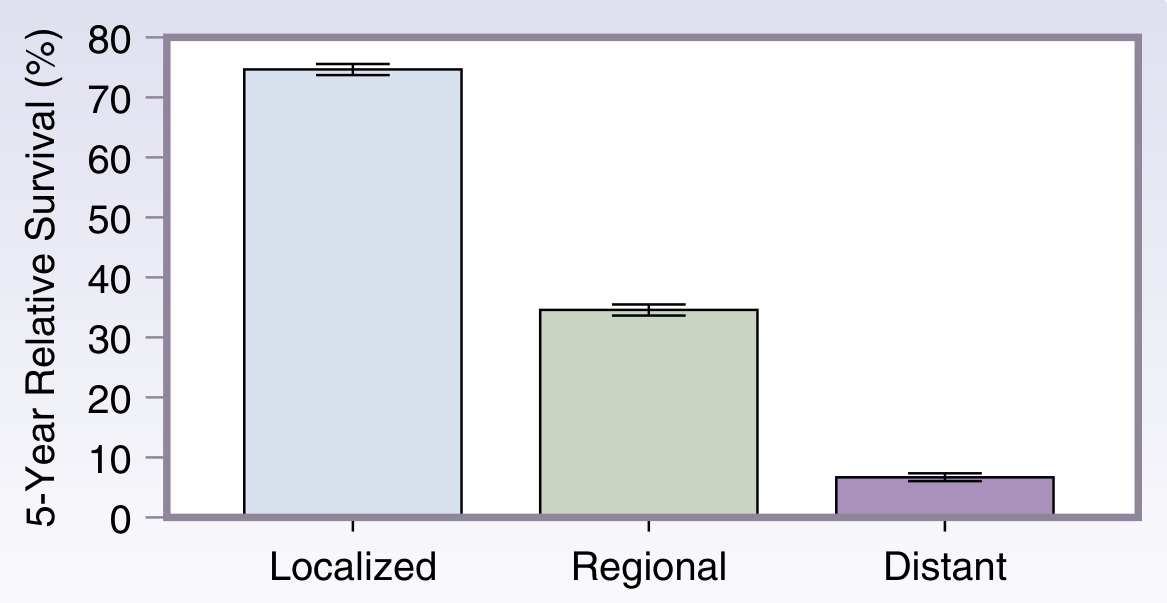
- Distant (Stage IV) 5-year survival: approximately 5-7%
- Localized disease: ~75% | Regional: ~35%
- Sabiston Textbook of Surgery (SEER data 2013-2019)
Summary Algorithm
Stage IVB Gastric Cancer
|
├── Test: HER2, PD-L1 (CPS), MSI/MMR, EBV, NTRK, RET, BRAF
|
├── HER2+ → Trastuzumab + Platinum/FP ± Nivolumab
|
├── MSI-H/dMMR → Pembrolizumab or Nivolumab (± chemo)
|
├── HER2-, PD-L1 CPS ≥5 → Nivolumab/Pembrolizumab + Platinum/FP
|
├── HER2-, CPS 0-4 → Platinum + Fluoropyrimidine ± ICI (individualized)
|
├── NTRK/RET/BRAF mutation → Targeted agent
|
└── All patients: Palliative/supportive care + nutritional support
Note: A 2025 systematic review (PMID 40696068) confirms conversion surgery may benefit select Stage IV patients who respond well to systemic therapy. Zolbetuximab (targeting Claudin 18.2) is also emerging as a new first-line option in Claudin18.2+ / HER2- tumors based on the SPOTLIGHT and GLOW trials - a 2025 meta-analysis (PMID 41203756) confirms Claudin18.2 as a significant prognostic and therapeutic target.
This is a shared conversation. Sign in to Orris to start your own chat.