Glioma
Reading File
Finding Sources
Searching PubMed
glioma classification treatment
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Excellent - I have comprehensive content from Harrison's 22E and Bailey & Love. Let me now compile the full answer.
Glioma
Gliomas are the most common malignant primary brain tumors, arising from glial cells. The 2021 WHO Classification fundamentally restructured their categorization by separating them into adult-type and pediatric-type diffuse gliomas, based on molecular genetic differences rather than histology alone.
1. Classification (2021 WHO CNS Tumor Classification)
Adult-Type Diffuse Gliomas
| Tumor Type | Key Molecular Alterations |
|---|---|
| Astrocytoma, IDH-mutant | IDH1, IDH2 (1p/19q intact) |
| Oligodendroglioma, IDH-mutant, 1p/19q-codeleted | IDH1/IDH2 + 1p/19q co-deletion |
| Glioblastoma, IDH wild-type | Chr 7 gain, Chr 10 loss; TERT, EGFR |
Pediatric-Type Diffuse Gliomas (can occur in adults)
| Tumor Type | Key Molecular Alterations |
|---|---|
| Diffuse midline glioma, H3 K27-altered | H3 K27M, EGFR, EZHIP |
| Diffuse hemispheric glioma, H3 G34-mutant | H3.3 G34R/V |
| Diffuse pediatric high-grade glioma, H3/IDH wild-type | EGFR, PDGFRA, MYCN |
| Diffuse low-grade glioma, MAPK pathway-altered | BRAF V600E/fusion, FGFR mutations |
The three key adult groups are defined by: IDH mutation status first, then 1p/19q co-deletion. Both carry significant prognostic impact.
2. Epidemiology & Clinical Presentation
- Low-grade glioma (WHO Grade II): Peak incidence in the 4th decade; commonly presents with seizures initially
- High-grade gliomas (WHO Grade III-IV): Present de novo in the 5th-6th decades, or by malignant transformation of low-grade tumors
- Glioblastoma (GBM, IDH wild-type): Most common glial tumor; peak in 5th-6th decade; presents with headache, focal neurological deficits, cognitive change, or seizures
- Rare presentation: Gliomatosis cerebri pattern - diffuse brain infiltration without focal mass, with cognitive symptoms; now categorized by biopsy pathology rather than as a separate entity
Hereditary syndromes predisposing to glioma include: NF1, NF2, Li-Fraumeni, Turcot, VHL, Lynch syndrome, TSC, and others.
3. Imaging
MRI with and without gadolinium is the preferred modality.
- Low-grade: T2/FLAIR hyperintense, typically non-enhancing
- High-grade/GBM: Ring-enhancing lesion with central necrosis and surrounding edema, mass effect
- CT with contrast also used (see below - heterogeneous frontoparietal lesion with midline shift)
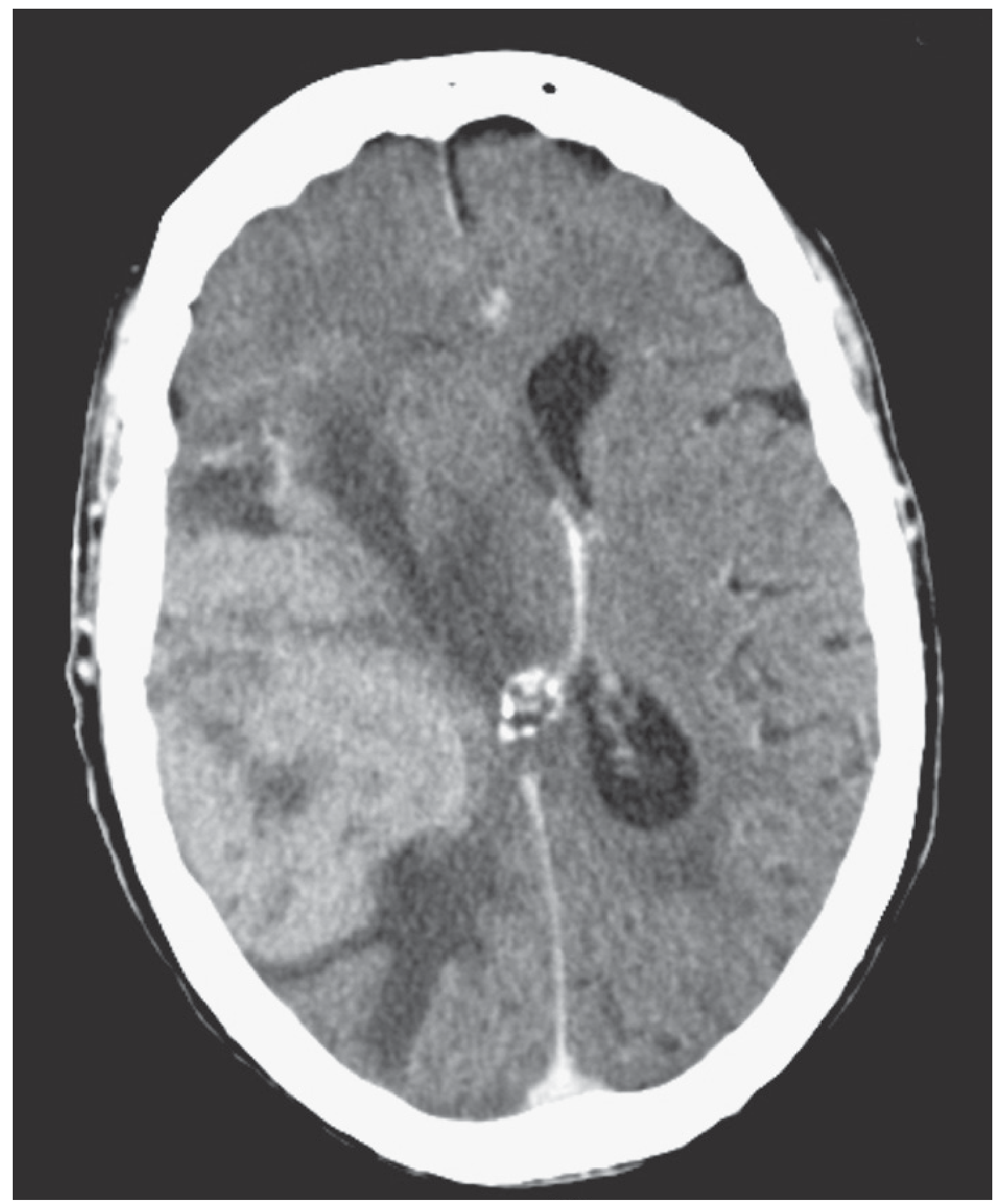
CT with contrast: heterogeneous right frontoparietal GBM with mass effect and midline shift - Bailey & Love's Surgery, Fig 48.22
Diffusion-weighted MRI is valuable to exclude brain abscess (which shows prominent restricted diffusion). CT chest/abdomen/pelvis is done to exclude extracranial primary (since metastasis is the main differential).
Pathological specimen showing the characteristic hemorrhagic, necrotic appearance of GBM:

Pathological specimen of glioblastoma multiforme - Bailey & Love's Surgery, Fig 48.23
4. Management
Initial Measures
- High-dose corticosteroids (dexamethasone) to alleviate mass effect
- Anti-epileptics for seizures or when anticipated (temporal location)
Surgery
- Surgical resection is the primary treatment: reduces disease burden and provides tissue for histological and molecular diagnosis
- Awake craniotomy when tumor is near eloquent cortex (speech areas), allowing intraoperative speech mapping
- Complete excision is impossible for most gliomas (except Grade I pilocytic astrocytoma in children) due to diffuse infiltration into surrounding brain
- Stereotactic biopsy when resection is not feasible
Adjuvant Therapy
Glioblastoma (IDH wild-type):
- Standard of care: Stupp protocol - concurrent temozolomide + radiotherapy (60 Gy in 30 fractions) followed by adjuvant temozolomide for 6 cycles
- MGMT promoter methylation is the key predictive biomarker for temozolomide benefit
- Bevacizumab (anti-VEGF) approved for recurrent GBM; improves progression-free survival
- Tumour Treating Fields (TTFields) - low-intensity alternating electric fields - added to maintenance temozolomide for newly diagnosed GBM (FDA approved 2015)
IDH-mutant low/intermediate-grade gliomas:
- Treatment depends on molecular subtype and risk stratification
- Radiotherapy + PCV chemotherapy (procarbazine, lomustine, vincristine) or temozolomide following resection
- Vorasidenib (IDH1/2 inhibitor) - a landmark 2023 New England Journal of Medicine trial showed benefit in IDH-mutant low-grade glioma and it received FDA approval in 2024 for this indication
Recurrence
- Re-irradiation, repeat surgery, and systemic therapy options at recurrence
- Clinical trials are strongly encouraged
5. Prognosis
| Tumor | Median Survival |
|---|---|
| GBM (IDH wild-type) | ~15 months (with Stupp protocol) |
| Anaplastic astrocytoma (IDH-mutant) | 3-5 years |
| Oligodendroglioma (IDH-mutant, 1p/19q-codeleted) | 10-15+ years |
| Low-grade astrocytoma (IDH-mutant) | 5-10 years |
Favorable prognostic factors: IDH mutation, 1p/19q co-deletion, MGMT methylation, younger age, good performance status, maximal surgical resection.
6. Pediatric Gliomas
- Pilocytic astrocytoma (WHO Grade I): Most common pediatric brain tumor; cerebellar location; often curable with complete resection; not infiltrative
- Optic pathway gliomas: Common in NF1; often managed conservatively or with chemotherapy
- Diffuse intrinsic pontine glioma (DIPG) / Diffuse midline glioma H3 K27-altered: Highly malignant; brainstem location precludes surgery; median survival ~12 months; H3 K27M mutation is diagnostic
- Pediatric low-grade gliomas often harbor BRAF alterations (BRAF V600E or BRAF-KIAA1549 fusion)
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Ch. 95 - Diffuse Glioma
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 48 - Glioma
- Recent evidence: A 2025 umbrella review (Yang et al., Ann Med PMID 40598793) comparing glioma treatment strategies, and vorasidenib approval (Mellinghoff IK et al., NEJM 2023 - referenced in Harrison's 22E)
This is a shared conversation. Sign in to Orris to start your own chat.