Pure tone audiometry
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have everything needed for a thorough, well-illustrated answer. Let me compile it.
Pure Tone Audiometry (PTA)
Definition and Purpose
Pure-tone audiometry is the most widely used test for evaluating auditory sensitivity. It establishes hearing sensitivity thresholds at discrete frequencies across the range important for human communication. The threshold is defined (by ANSI/ASA S3.21-2004) as "the lowest sound pressure level at which responses occur in at least 50% of ascending trials." Results are plotted on a graphic chart called an audiogram. - Cummings Otolaryngology Head and Neck Surgery, p. 2566
The Audiogram
The audiogram is a graph with:
- X-axis (horizontal): Frequency in Hertz (Hz), from low (250 Hz) to high (8000 Hz), at octave intervals
- Y-axis (vertical): Hearing Level in decibels (dB HL), from -10 at top to 120 dB at bottom (worse hearing = lower on page)
The reference point (0 dB HL) is calibrated to the average threshold of normal young adults (ANSI S3.6-1969). - Cummings Otolaryngology, p. 2566
Audiogram Symbols
| Symbol | Meaning |
|---|---|
| O | Right ear, unmasked air conduction |
| X | Left ear, unmasked air conduction |
| △ | Right ear, masked air conduction |
| □ | Left ear, masked air conduction |
| < | Right ear, unmasked bone conduction |
| > | Left ear, unmasked bone conduction |
| [ | Right ear, masked bone conduction |
| ] | Left ear, masked bone conduction |
Right ear is conventionally plotted in red, left ear in blue. - K.J. Lee's Essential Otolaryngology, Table 14-6
Test Frequencies
- Standard octave frequencies tested: 250, 500, 1000, 2000, 4000, and 8000 Hz
- Inter-octave frequencies (750, 1500, 3000, 6000 Hz) are added when there is a 25 dB or greater difference between adjacent octave thresholds
- 3000 and 6000 Hz are routinely included for baseline audiograms in noise-exposed workers and patients on ototoxic medications - K.J. Lee's Essential Otolaryngology, p. 296
Air Conduction Testing
Air-conduction (AC) thresholds measure the function of the entire hearing system - external ear, middle ear, and inner ear. Tones are delivered through supra-aural headphones or insert earphones.
Hughson-Westlake ascending method:
- Present tone well above threshold, then decrease in 10-15 dB steps until inaudible
- Increase in 5 dB steps, decrease in 10 dB steps
- The threshold = level at which a response is obtained at least 3 times - Cummings Otolaryngology, p. 2566
Bone Conduction Testing
Bone-conduction (BC) testing delivers sound via a bone oscillator placed on the mastoid process, bypassing the outer and middle ear and stimulating the cochlea directly. It therefore reflects inner ear (sensorineural) function.
- Comparison of AC and BC thresholds determines the type of hearing loss
- The difference between AC and BC thresholds is the air-bone gap (ABG), reflecting the conductive component - K.J. Lee's Essential Otolaryngology, p. 297
Types of Hearing Loss
1. Conductive Hearing Loss
- AC thresholds elevated, BC thresholds normal
- Air-bone gap present (≥ 10 dB)
- Pathology: outer or middle ear (e.g., otitis media, otosclerosis, perforated TM)
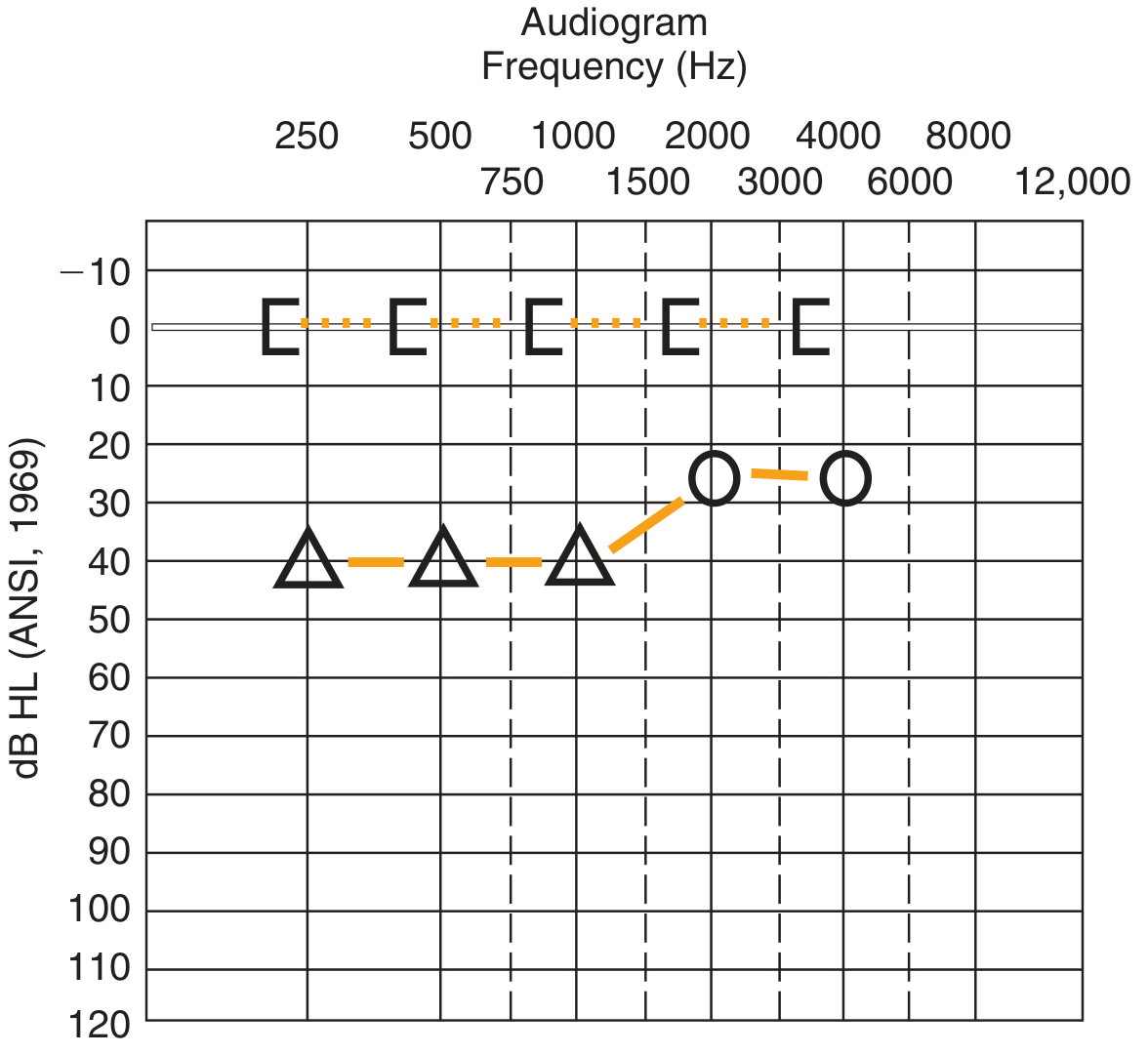
Air-bone gap: bone conduction thresholds (bracket symbols) at 0 dB HL, air conduction (circles and triangles) at 25-40 dB HL.
2. Sensorineural Hearing Loss (SNHL)
- AC and BC thresholds equally elevated - no air-bone gap
- Pathology: cochlea (sensory) or auditory nerve/central pathway (neural)
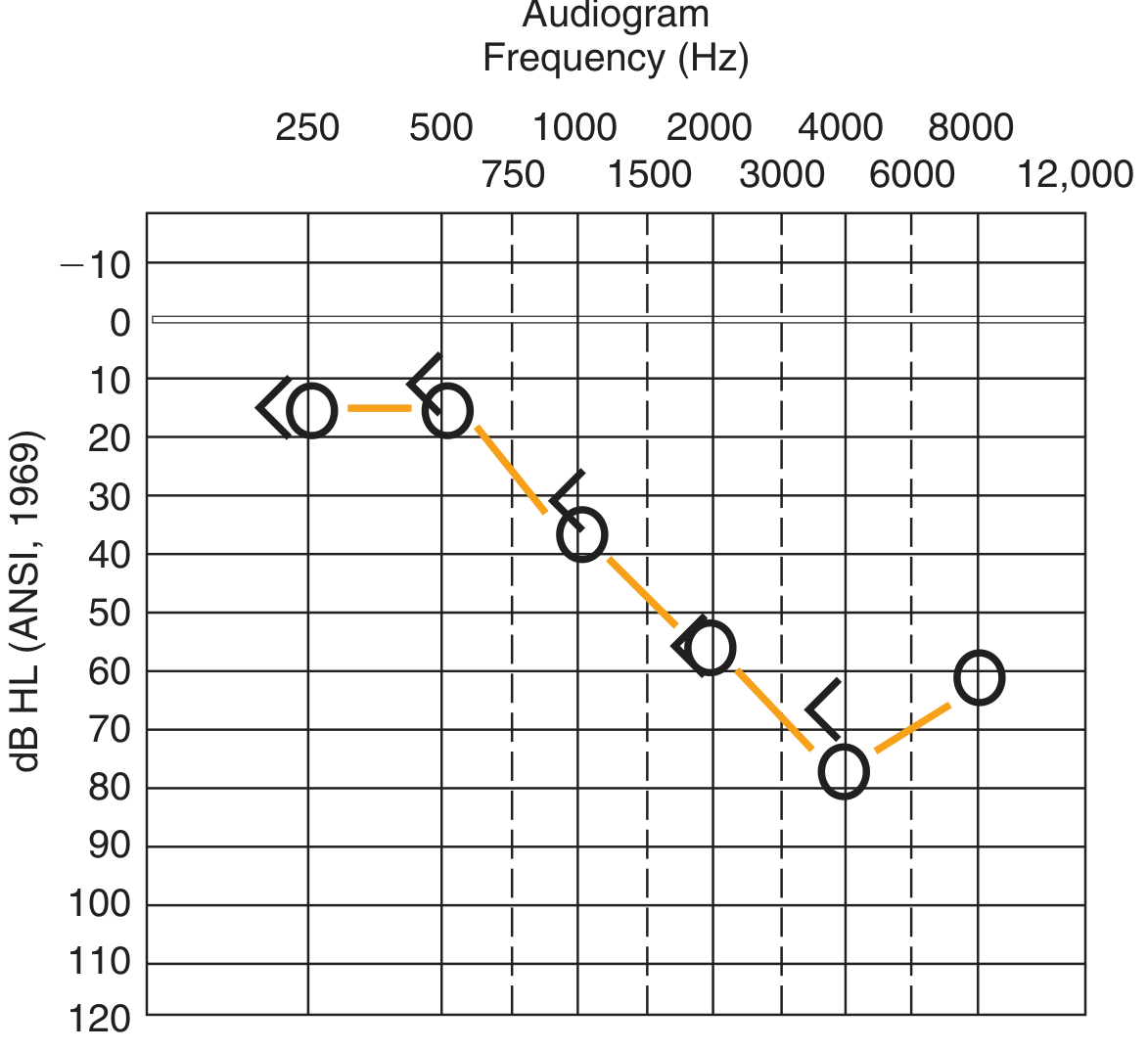
SNHL: Both AC (circles) and BC (left-arrow symbols) thresholds are elevated and closely parallel - no air-bone gap.
3. Mixed Hearing Loss
- Both AC and BC thresholds elevated, but AC worse than BC (air-bone gap present on top of SNHL baseline)
- Example: otosclerosis with cochlear damage
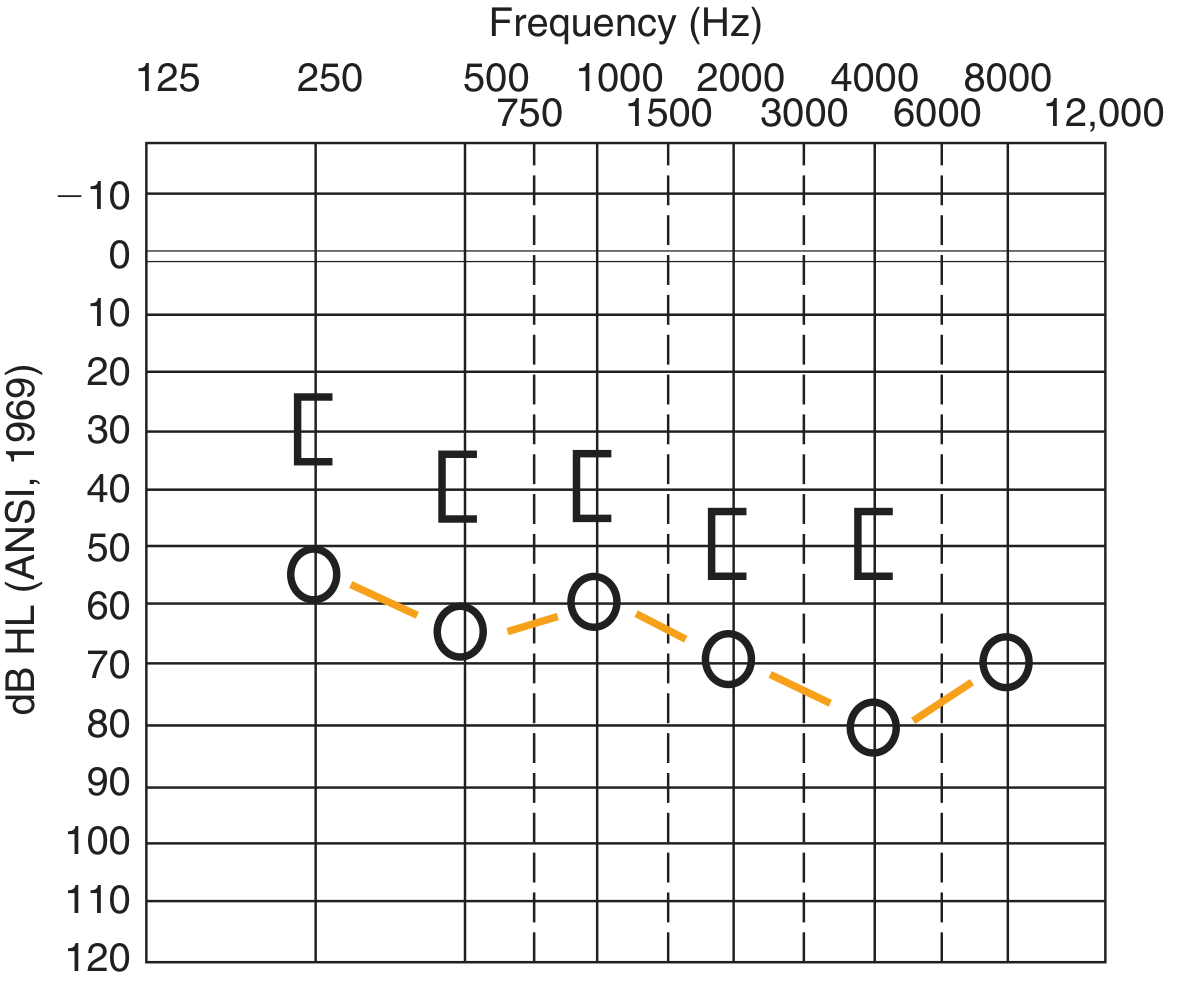
Mixed loss: BC thresholds elevated (SNHL component), AC thresholds even more elevated (conductive component on top).
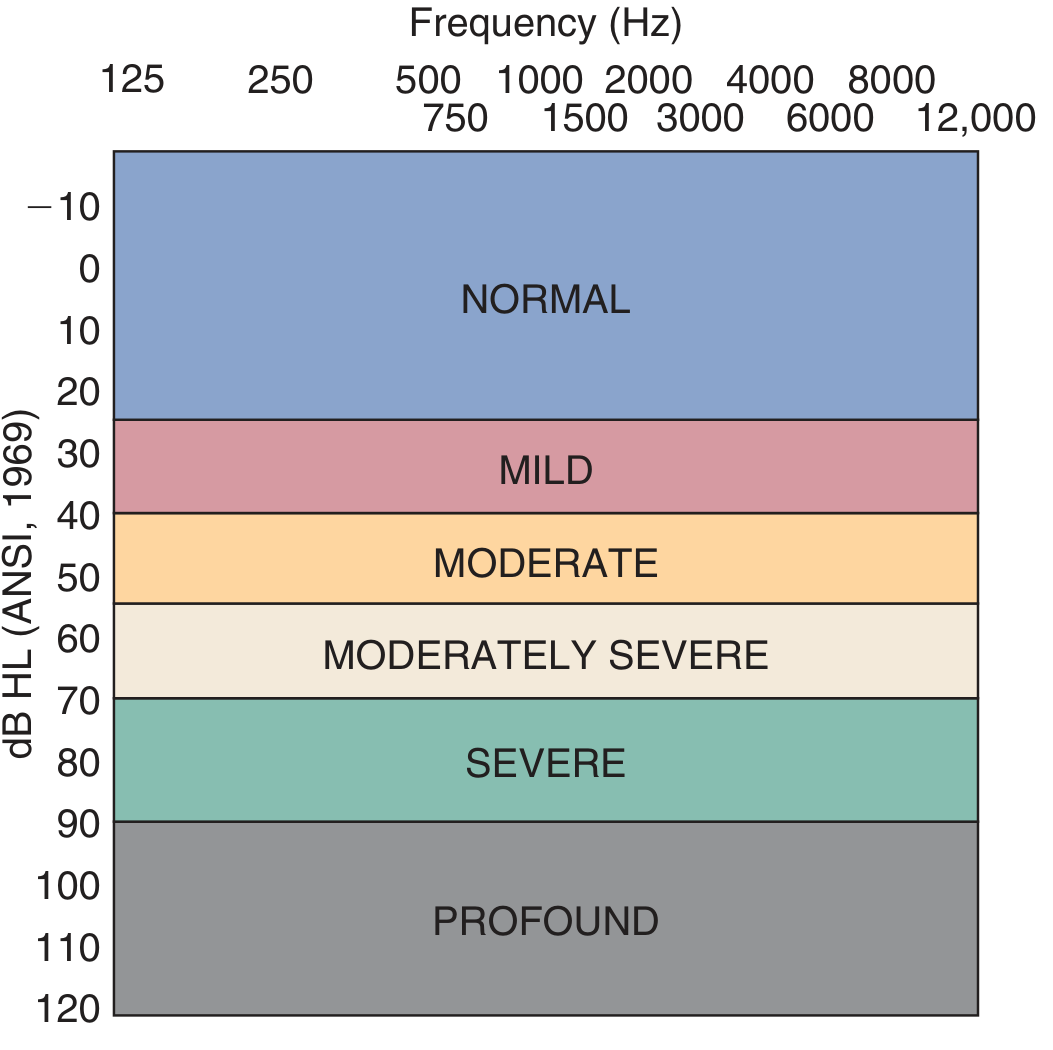
Degrees of Hearing Loss
| Degree | Threshold Range |
|---|---|
| Normal | ≤ 25 dB HL (adults); ≤ 15 dB HL (children) |
| Minimal | 15-25 dB HL |
| Mild | 25-40 dB HL |
| Moderate | 40-55 dB HL |
| Moderately severe | 55-70 dB HL |
| Severe | 70-90 dB HL |
| Profound | > 90 dB HL |
Note: 99% of normal-hearing individuals have thresholds between -15 and +15 dB HL. - Shambaugh Surgery of the Ear, p. 4587
Pure-Tone Average (PTA)
The PTA is calculated as the average threshold at 500, 1000, and 2000 Hz (the speech frequencies). It correlates closely with the Speech Detection Threshold (SDT) and is used to cross-check Speech Reception Threshold (SRT). An agreement within 6-10 dB between PTA and SRT validates the audiogram. - Cummings Otolaryngology, p. 2567
Masking
Why mask? Sound can travel through the skull from the test ear to the non-test ear (crossover), causing the non-test ear to respond - a "shadow curve." Masking introduces narrow-band noise into the non-test ear to prevent this.
When to mask:
- Air conduction: Mask when AC stimulus to test ear exceeds BC threshold of non-test ear by ≥ 40 dB (supra-aural headphones) or ≥ 70 dB (insert earphones)
- Bone conduction: Mask whenever there is an air-bone gap > 10 dB in the test ear (since interaural attenuation for BC is only 0-10 dB, meaning BC almost always requires masking when an ABG exists)
Interaural attenuation:
- Supra-aural headphones: 40-65 dB (frequency dependent)
- Insert earphones: 70-90 dB (preferred for minimizing crossover)
- Bone conduction: 0-10 dB - K.J. Lee's Essential Otolaryngology, p. 297
The preferred masker for pure-tone testing is narrow-band noise centered at the test frequency.
Audiogram Configurations
The shape of the audiogram provides diagnostic clues:
| Configuration | Description | Common Causes |
|---|---|---|
| Flat | Similar loss at all frequencies | Conductive loss, some SNHL |
| Sloping / High-frequency | Better low, worse high | Noise-induced, presbycusis, SNHL |
| Rising / Low-frequency | Worse low, better high | Meniere's disease (early), endolymphatic hydrops |
| Notched | Notch at 4000 Hz, recovery at 8000 Hz | Noise-induced hearing loss (classic 4 kHz notch) |
| Saucer-shaped | Mid-frequency dip (cookie-bite) | Hereditary SNHL |
| Falling | Progressive drop across frequencies | Various cochlear pathologies |
- K.J. Lee's Essential Otolaryngology, p. 299-300
Reliability Factors (for Valid Testing)
A reliable PTA requires:
- Sound-treated booth (quiet enough to measure 0 dB HL thresholds)
- Calibrated audiometer (full calibration annually)
- Trained examiner (preferably a licensed audiologist)
- Clear, age-appropriate instructions
- Otoscopic inspection before testing
- Correct earphone/bone oscillator placement
- Patient comfort
- K.J. Lee's Essential Otolaryngology, p. 296
Testing in Children
| Age Group | Method |
|---|---|
| 0-6 months | Behavioral Observation Audiometry (BOA) - observe responses to sound-field signals |
| 6 months - 2 years | Visual Reinforcement Audiometry (VRA) - head-turn to sound conditioned with visual reward |
| 2-5 years | Conditioned Play Audiometry (CPA) - behavioral response conditioned with play task (e.g., toss block into box) |
| > 5 years | Standard PTA - conventional audiometry |
- Shambaugh Surgery of the Ear, p. 4589
Interpretation in Clinical Context
PTA alone identifies the degree and type of hearing loss but says little about etiology. Comprehensive audiological evaluation combines:
- PTA (sensitivity thresholds)
- Speech audiometry (SRT, Word Recognition Score)
- Tympanometry (middle ear pressure, compliance)
- Acoustic reflex testing
- Otoacoustic emissions (OAE) - marker of outer hair cell function
- Auditory Brainstem Response (ABR) - for retrocochlear lesions or infant testing
Pure-tone results should always be interpreted in conjunction with these complementary tests. - K.J. Lee's Essential Otolaryngology, p. 300
This is a shared conversation. Sign in to Orris to start your own chat.