Respiratory distress syndrome in pediatrics mbbs with proper understanding with photos and imaginations
Reading File
Finding Sources
Searching the Web
respiratory distress syndrome neonatal pediatric pathophysiology surfactant MBBS
Searching PubMed
"respiratory distress syndrome" newborn surfactant treatment
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Searching the Web
neonatal RDS chest X-ray ground glass reticulogranular appearance hyaline membrane disease image
Loading Image
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative textbooks and images. Let me compose the full, detailed MBBS-level answer.
Neonatal / Pediatric Respiratory Distress Syndrome (RDS)
Also called: Hyaline Membrane Disease (HMD) | Infantile RDS (IRDS) | Surfactant Deficiency Disorder
1. Introduction & Overview
Respiratory Distress Syndrome is the most common cause of respiratory distress in premature neonates, and one of the top causes of early neonatal mortality and long-term morbidity. It affects approximately 2% of all neonates - but the incidence rises sharply with decreasing gestational age:
- ~92% at 24-25 weeks gestation
- ~88% at 26-27 weeks
- ~76% at 28-29 weeks
- ~57% at 30-31 weeks
An estimated 30% of all neonatal disease results from RDS or its complications. - The Developing Human: Clinically Oriented Embryology
2. Fetal Lung Development - The Foundation
To understand RDS, you must understand when and how surfactant is made.
The fetal lung goes through these stages:
| Stage | Gestational Age | Key Event |
|---|---|---|
| Embryonic | 3-7 weeks | Lung bud forms from foregut |
| Pseudoglandular | 7-16 weeks | Airways branch, no gas exchange |
| Canalicular | 16-26 weeks | Blood-gas barrier begins to form |
| Saccular | 24-38 weeks | Terminal sacs form; Type II cells appear |
| Alveolar | 36 weeks - 2 years | True alveoli form; surfactant production matures |
Type II pneumocytes (alveolar epithelial cells) are the key cells. They begin appearing at ~22-24 weeks and produce surfactant, which is stored in lamellar bodies and secreted into the alveolar lining layer. Before ~34 weeks, surfactant production is often insufficient.
3. Surfactant - What It Is and What It Does
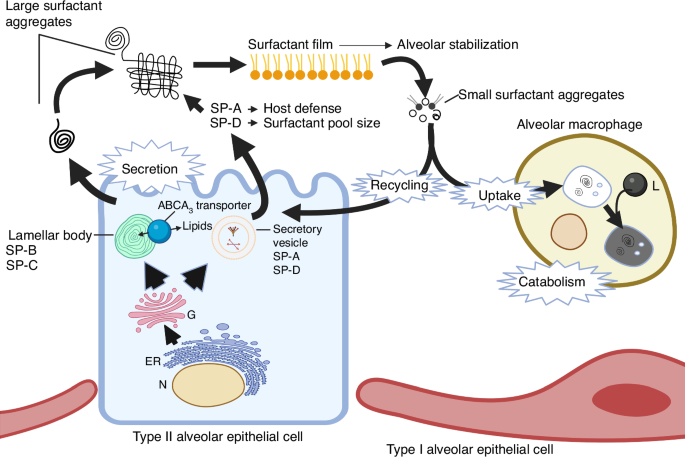
Surfactant is a complex mixture of:
- ~90% phospholipids - mainly dipalmitoyl phosphatidylcholine (DPPC), the workhorse molecule
- ~10% proteins - SP-A, SP-B, SP-C, SP-D
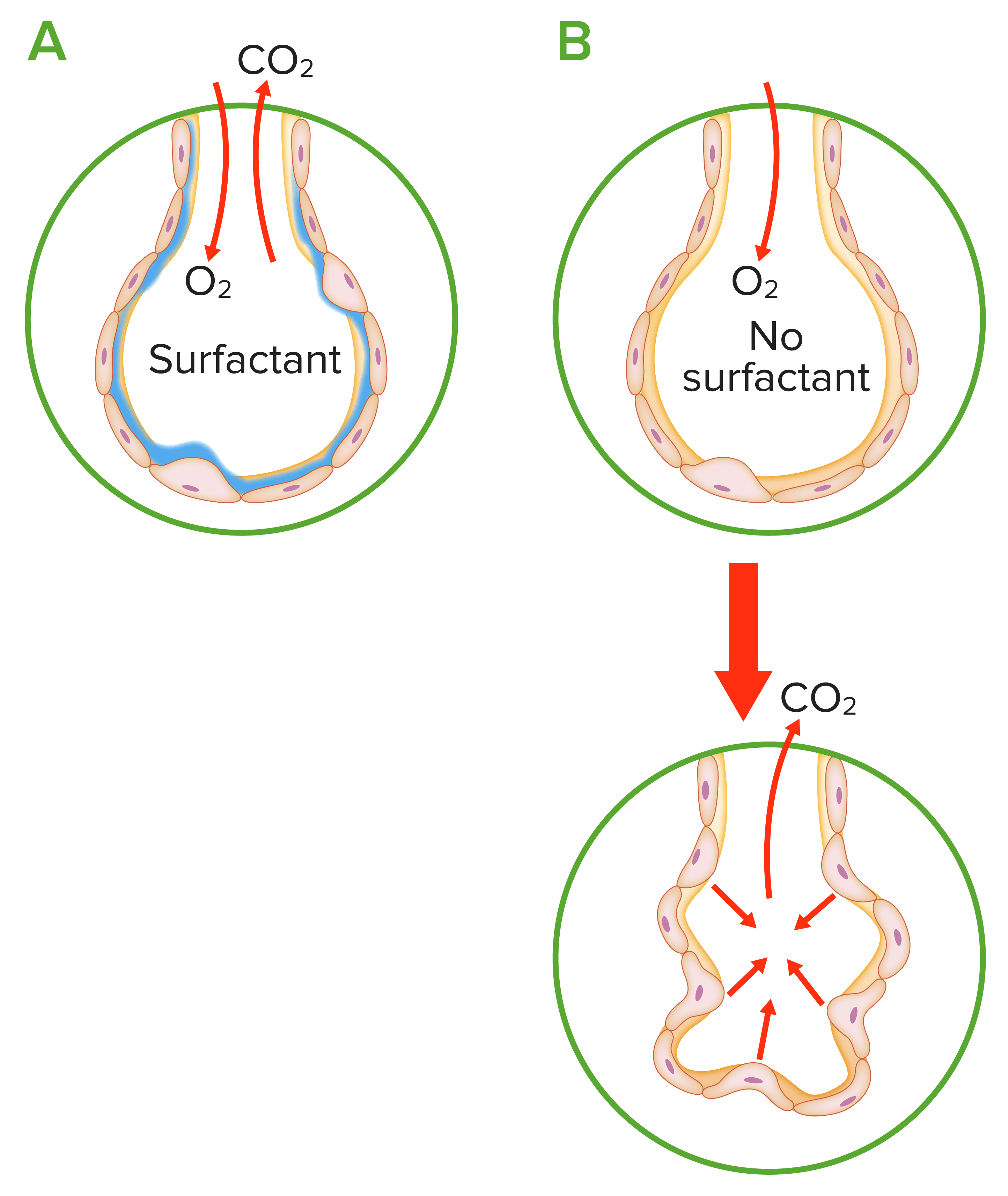
Function of surfactant - obeying Laplace's Law:
Surface tension (T) = Pressure (P) × radius (r) / 2
Without surfactant, the high surface tension at the air-liquid interface in small alveoli causes them to collapse on expiration (atelectasis). Surfactant coats the alveolar inner surface, dramatically reducing surface tension, especially at low lung volumes during exhalation - keeping alveoli open.
- SP-B and SP-C - small hydrophobic proteins that are essential for surface tension reduction; present in commercial surfactant preparations
- SP-A and SP-D - larger hydrophilic proteins involved in host defense and maintaining surfactant pool size
4. Pathophysiology of RDS
The Core Problem: Surfactant Deficiency
Follow this cascade:
Premature birth (< 34 weeks)
↓
Insufficient Type II pneumocytes → LOW SURFACTANT
↓
High alveolar surface tension
↓
Alveolar collapse (ATELECTASIS) at end-expiration
↓
Reduced functional residual capacity (FRC)
↓
V/Q mismatch → HYPOXIA + HYPERCAPNIA
↓
Pulmonary vasoconstriction → Pulmonary hypertension
↓
Right-to-left shunt (through PDA or foramen ovale)
↓
Worsened hypoxia → Acidosis
↓
Acidosis further damages Type II cells
↓
Even LESS surfactant produced → vicious cycle
The Hyaline Membrane
The name "hyaline membrane disease" comes from this: alveolar-capillary leak (from hypoxic injury) allows plasma proteins to flood the alveoli. Combined with epithelial cell debris, fibrin, red blood cells, and leukocytes, this forms an eosinophilic, glassy (hyaline) membrane lining the distal airspaces and terminal bronchioles. This membrane is visible on histology and macroscopically makes the lung look like liver tissue (hepatization).
Factors That Worsen Surfactant Deficiency
| Risk Factor | Mechanism |
|---|---|
| Prematurity | Immature Type II cells |
| Maternal diabetes | Insulin inhibits surfactant synthesis |
| Perinatal asphyxia | Damages Type II cells directly |
| Cesarean section without labor | Labor induces cortisol surge that matures surfactant |
| Male sex | Androgens slow lung maturation (boys affected more than girls) |
| Caucasian race | Genetic predisposition |
| SP-B gene deficiency | Rare genetic cause; often fatal |
| Congenital diaphragmatic hernia | Lung hypoplasia - fewer Type II cells |
| Sepsis / pneumonia | Inactivate existing surfactant |
5. Clinical Presentation
Symptoms typically appear within minutes to hours of birth (unlike TTN which may be milder and delayed slightly).
Classic Signs (TNRCG mnemonic):
- T - Tachypnea (respiratory rate > 60 breaths/min)
- N - Nasal flaring
- R - Retractions - subcostal, intercostal, sternal notch (use of accessory muscles)
- C - Cyanosis (central)
- G - Grunting (expiratory) - the HALLMARK sign
Why does the baby grunt?
The baby expires against a partially closed glottis - this is the infant's instinctive attempt to generate auto-PEEP (positive end-expiratory pressure) to prevent alveolar collapse. The grunt IS the baby trying to be its own CPAP machine!
Clinical Course
- Symptoms worsen over the first 48-72 hours
- Then gradually improve (natural surfactant production increases)
- With exogenous surfactant treatment, recovery is much faster
6. Radiology - Chest X-Ray
CXR Grade 1 (Mild)
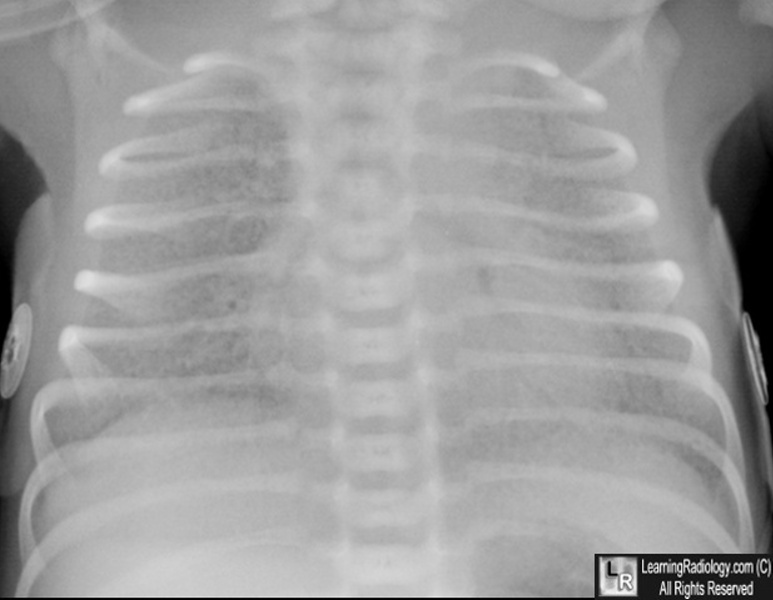
Mild granular opacification. Heart borders still visible. Low lung volumes.
CXR Grade 3-4 (Severe)
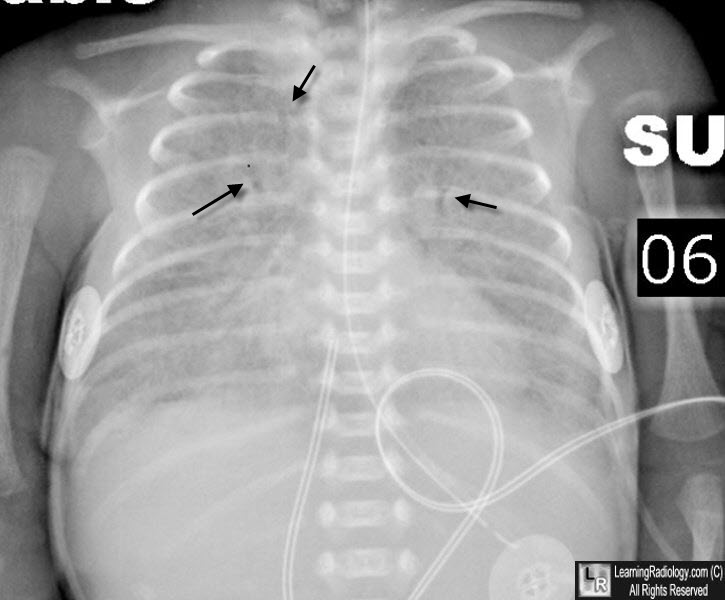
Severe RDS - diffuse reticulogranular (ground-glass) opacification, prominent air bronchograms (arrows), small lung volumes.
CXR Grading System (4 Grades)
| Grade | Appearance |
|---|---|
| Grade 1 | Mild ground-glass / granular opacification; clear cardiac borders |
| Grade 2 | Granular opacification + air bronchograms |
| Grade 3 | Increased consolidation; obscured heart and diaphragm borders |
| Grade 4 | Complete "white-out" (total opacification) of both lung fields |
Pathognomonic features:
- Ground-glass reticulogranular pattern - diffuse microatelectasis
- Air bronchograms - air-filled large airways visible against the opacified alveolar background
- Low lung volumes - small, hypoexpanded chest
- Note: Hyperinflation in a preterm infant without ventilation makes RDS highly unlikely
7. Diagnosis
RDS is a clinical + radiological diagnosis:
| Investigation | Finding in RDS |
|---|---|
| Chest X-ray | Reticulogranular pattern, air bronchograms, low volume |
| ABG | Hypoxemia (low PaO₂), Hypercapnia (high PaCO₂), Respiratory + metabolic acidosis |
| Lung ultrasound | Bilateral B-lines, "white lung" appearance (increasingly used) |
| Tracheal aspirate | Reduced surfactant activity (not routinely done) |
| Histopathology | Hyaline membranes, atelectasis with dilated terminal bronchioles |
Differential Diagnosis
| Condition | Key Distinction |
|---|---|
| Transient Tachypnea of Newborn (TTN) | Perihilar streaking (not ground glass); improves within 24h; term baby |
| Meconium Aspiration Syndrome | Hyperinflated lungs; patchy irregular opacities; post-term baby |
| Congenital pneumonia | Asymmetric opacities; risk factors (maternal fever, PROM) |
| Congenital heart disease | Cardiomegaly; no typical reticulogranular pattern |
| Pneumothorax | Hyperlucent hemithorax; mediastinal shift |
8. Management
Antenatal Prevention (the most impactful intervention!)
Antenatal Corticosteroids (ANS):
- Betamethasone (preferred): 12 mg IM × 2 doses, 24 hours apart
- OR Dexamethasone: 6 mg IM × 4 doses, 12 hours apart
- Given to mothers at risk of preterm delivery between 24-34 weeks gestation
- Extended to 34-37 weeks (late preterm) if delivery risk is present
- Also recommended for elective cesarean at term (reduces respiratory morbidity)
- Mechanism: Corticosteroids stimulate surfactant production by maturing Type II pneumocytes and increasing SP-B and SP-C gene expression
- A single rescue course is recommended if >7 days since first course and delivery still threatened
- Recent evidence (2025 meta-analysis, PMID 40418984): beneficial even for late preterm births
Postnatal Management - Step-by-Step
Step 1 - Immediate Stabilization:
- Warm, neutral thermal environment (incubator or radiant warmer)
- Pulse oximetry monitoring; target SpO₂ 90-95% (avoid both hypoxia AND hyperoxia)
- PaO₂ target: 50-80 mmHg
- Screen for sepsis (blood culture, CBC); start empirical antibiotics × 48h until cultures clear
Step 2 - Respiratory Support (escalate as needed):
Mild RDS → Supplemental O₂ (nasal cannula/hood)
↓
Moderate RDS → CPAP (nasal) ← Start here for most preterm infants
↓
Severe RDS → Intubation + Mechanical Ventilation
- Bubble CPAP (4-6 cm H₂O via nasal prongs) - keeps alveoli open, reduces work of breathing, reduces intubation need
- Gentle ventilation strategies are preferred to minimize barotrauma/volutrauma - the INSURE technique (INtubate, SURfactant, Extubate) aims to minimize ventilation time
Step 3 - Surfactant Replacement Therapy (SRT) - the cornerstone of treatment:
-
Delivered intratracheally via endotracheal tube
-
Works immediately - increases lung compliance, reduces oxygen and pressure requirements
-
Animal-derived surfactants (containing SP-B and SP-C) are the standard:
- Beractant (Survanta) - bovine
- Poractant alfa (Curosurf) - porcine (most widely used)
- Calfactant (Infasurf) - calf lung
-
Three strategies:
- Prophylactic - given before first breath to all at-risk infants (< 27-28 weeks)
- Early rescue - given within 2 hours of clinical diagnosis
- Late rescue - given when FiO₂ > 0.3-0.4 and X-ray confirms RDS
-
Latest evidence (2024-2025 network meta-analysis, PMID 39736686 and 41430414): Poractant alfa + budesonide shows additional benefit in extremely preterm infants ≤28 weeks, reducing BPD rates
-
Less invasive surfactant administration (LISA/MIST): surfactant given via thin catheter while baby breathes spontaneously on CPAP - avoids intubation, increasingly preferred
9. Complications
Acute Complications:
| Complication | Mechanism |
|---|---|
| Pneumothorax / Air leak | Alveolar rupture from barotrauma or volutrauma |
| Pulmonary hemorrhage | Capillary injury from hypoxia |
| Patent Ductus Arteriosus (PDA) | Hypoxia keeps ductus open; PDA causes pulmonary overflow |
| Intraventricular Hemorrhage (IVH) | Hemodynamic instability, hypoxia |
| Necrotizing Enterocolitis (NEC) | Bowel ischemia in hypoxic preterm infant |
| Pulmonary hypertension | Hypoxic vasoconstriction → R→L shunting |
Chronic / Long-term Complication:
Bronchopulmonary Dysplasia (BPD) - the most important long-term complication:
- Defined as oxygen dependency at 28 days of life (or 36 weeks corrected gestational age)
- Caused by: oxygen toxicity, barotrauma/volutrauma from mechanical ventilation, inflammation, infection
- Histology: simplified large alveoli, impaired capillary development, variable interstitial fibrosis
- Management: gradual weaning of O₂ and ventilatory support, pulmonary vasodilators (sildenafil, bosentan, nitric oxide) if pulmonary hypertension develops
10. Visual Summary

11. Quick Memory Mnemonics for MBBS
Risk Factors - "PDMCMG":
- Prematurity
- Diabetes (maternal)
- Male sex
- Caesarean (without labor)
- Multiple gestation (twins)
- Genetic (SP-B deficiency)
Signs - "TNCGR" (The Newborn Can't Get air Right):
- Tachypnea
- Nasal flaring
- Cyanosis
- Grunting (expiratory)
- Retractions
Management - "ASST":
- Antenatal steroids (prevention)
- Supplemental oxygen / SpO₂ targets
- Surfactant replacement
- Thermal environment + supportive care
12. Recent Evidence Update (2024-2026)
| Study | Finding |
|---|---|
| Meta-analysis, 2024 (PMID 39736686) | Poractant alfa (porcine) shows superior outcomes vs. beractant in network meta-analysis of surfactant delivery strategies |
| Meta-analysis, 2025 (PMID 40418984) | Antenatal corticosteroids benefit confirmed even for late preterm births (34-37 wks) |
| Systematic review, 2025 (PMID 41430414) | Surfactant + budesonide reduces BPD rates in infants ≤28 weeks gestation |
Key Take-Home Points for Exams
- RDS = surfactant deficiency in preterm infants - Type II pneumocytes not mature enough
- Hallmark sign = expiratory grunting (auto-PEEP mechanism)
- CXR = ground-glass reticulogranular pattern + air bronchograms + low lung volumes
- Pathology = hyaline membranes (eosinophilic) lining alveolar ducts on histology
- Prevention = antenatal betamethasone (24-34 weeks, given to mother)
- Treatment = CPAP + exogenous surfactant (intratracheal)
- Key complication = BPD (chronic lung disease of prematurity)
- RDS worsens over 48-72h then improves - surfactant accelerates this recovery
Sources: Creasy & Resnik's Maternal-Fetal Medicine, Fishman's Pulmonary Diseases and Disorders, The Developing Human: Clinically Oriented Embryology, Langman's Medical Embryology, StatPearls (NIH), LearningRadiology.com; supplemented with 2024-2025 PubMed meta-analyses (PMIDs: 39736686, 40418984, 41430414).
This is a shared conversation. Sign in to Orris to start your own chat.