Thyroid detail information, pathophysiology, symptoms, diagnosis treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Searching PubMed
thyroid disorders diagnosis treatment
Reading File
Loading Image
Here is a comprehensive overview of the thyroid gland — its anatomy, physiology, pathophysiology, clinical disorders, diagnosis, and treatment — drawn from Schwartz's Principles of Surgery, Robbins & Kumar Basic Pathology, and Costanzo Physiology.
The Thyroid Gland — Complete Overview
1. Anatomy & Embryology
The thyroid arises as an outpouching of the primitive foregut around week 3 of gestation, originating at the base of the tongue (foramen cecum). It descends via the thyroglossal duct, which normally obliterates by week 8. Failure of this obliteration results in thyroglossal duct cysts — the most common congenital cervical anomaly.
Gross Anatomy
- Two lobes connected by an isthmus, situated anterior to the larynx and trachea
- Each lobe weighs ~20 g in adults
- Blood supply: superior thyroid artery (from external carotid) and inferior thyroid artery (from thyrocervical trunk)
- Key surgical landmark: the recurrent laryngeal nerve (RLN) lies in close proximity and is at risk during thyroid surgery
Histology
- Divided into lobules, each containing 20–40 follicles
- Follicles are lined by cuboidal epithelial cells (follicular cells) that synthesize thyroglobulin (Tg), stored as colloid
- Parafollicular C cells (neuroectodermal origin) secrete calcitonin and are located in the upper poles
— Schwartz's Principles of Surgery, pp. 1625–1629; Robbins & Kumar Basic Pathology, p. 729
2. Physiology — Hormone Synthesis & Regulation
The HPT Axis
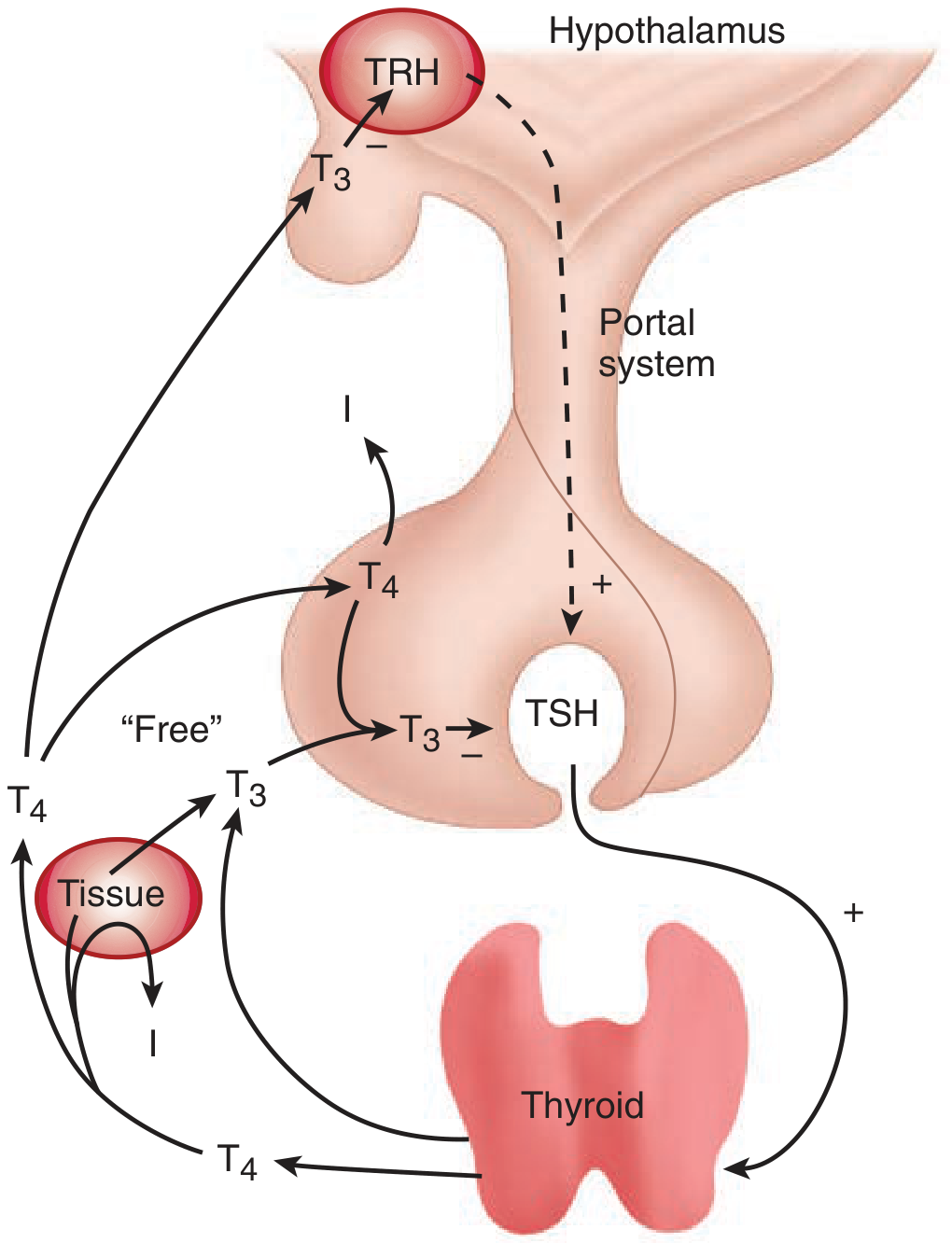
Figure: The hypothalamic-pituitary-thyroid (HPT) axis. TRH stimulates TSH, which drives T4/T3 synthesis. Free T3 provides negative feedback at both the hypothalamus and pituitary.
Steps in hormone synthesis:
- Iodide uptake: Active transport of I⁻ into follicular cells via Na⁺/I⁻ symporter
- Oxidation: Iodide → iodine (by thyroid peroxidase, TPO)
- Organification: Iodination of thyroglobulin to form MIT (monoiodotyrosine) and DIT (diiodotyrosine)
- Coupling: MIT + DIT → T3; DIT + DIT → T4 (catalyzed by TPO)
- Storage: As colloid within follicular lumen
- Secretion: TSH stimulates endocytosis of colloid → proteolysis releases T4 and T3
TSH regulation:
- TRH (hypothalamus) → stimulates TSH secretion
- Free T3 → negative feedback on both hypothalamus and anterior pituitary
- TSH binds follicular cell receptors → adenylyl cyclase/cAMP cascade → drives all steps of synthesis
Actions of Thyroid Hormones (T3 > T4 potency)
T4 is peripherally deiodinated to the active T3 by 5'-iodinase. T3 then enters the nucleus and binds thyroid hormone receptor (TR), stimulating gene transcription of:
| System | Effect |
|---|---|
| Metabolic (BMR) | ↑ O₂ consumption, ↑ Na⁺-K⁺ ATPase, ↑ heat production |
| Cardiovascular | ↑ Heart rate, ↑ stroke volume, ↑ cardiac output; induces β₁-adrenergic receptors & myosin |
| Nervous System | Essential for CNS maturation in fetus; normal adult mood/cognition |
| Skeletal | Synergizes with GH for bone growth |
| Metabolism | ↑ Gluconeogenesis, lipolysis, protein catabolism overall (catabolic effect) |
| Cholesterol | ↑ Synthesis AND ↑ degradation (net lowering effect) |
— Costanzo Physiology, pp. 427–428; Schwartz's Principles of Surgery, p. 1629
3. Thyroid Disorders — Pathophysiology, Symptoms, Diagnosis, Treatment
A. HYPERTHYROIDISM (Thyrotoxicosis)
Pathophysiology:
Elevated circulating thyroid hormones → hypermetabolic state + autonomic nervous system overactivity.
Three most common causes:
| Cause | Frequency |
|---|---|
| Graves disease (autoimmune TSH-R stimulating antibodies) | ~85% |
| Toxic multinodular goiter | Uncommon |
| Toxic adenoma | Uncommon |
| Other causes: thyroiditis (transient), TSH-secreting pituitary adenoma (rare) |
Symptoms & Signs:
| System | Manifestations |
|---|---|
| Constitutional | Weight loss despite ↑ appetite, heat intolerance, excessive sweating, warm/flushed skin |
| Cardiovascular | Palpitations, tachycardia, atrial fibrillation, wide pulse pressure |
| GI | Diarrhea, hypermotility, malabsorption |
| Neuromuscular | Anxiety, tremor, irritability, proximal muscle weakness (~50%) |
| Ocular | Lid lag, wide staring gaze (Dalrymple's sign); proptosis/exophthalmos in Graves disease |
| Female | Amenorrhea, infertility, miscarriages |
Graves-specific features:
- Ophthalmopathy: Proptosis, periorbital edema, chemosis, diplopia (in ~50%) caused by TSH-R antibodies targeting orbital fibroblasts
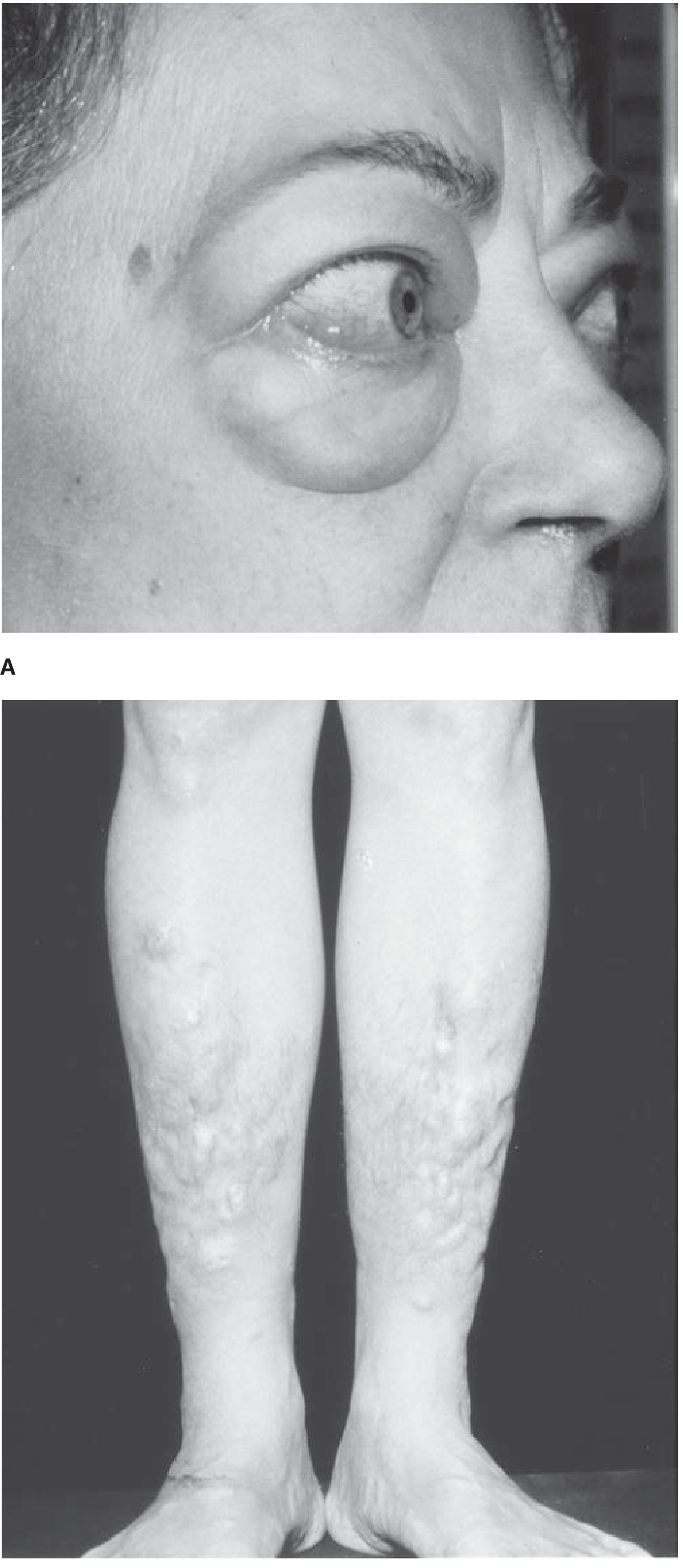
Figure: (A) Graves ophthalmopathy with exophthalmos and periorbital edema. (B) Pretibial myxedema — deposition of glycosaminoglycans on the pretibial skin and dorsum of feet.
- Dermopathy (pretibial myxedema): 1–2% of cases
- Thyroid acropachy: Rare subperiosteal bone formation in metacarpals
Thyroid Storm: Abrupt severe hyperthyroidism (fever, extreme tachycardia, agitation). Medical emergency — triggered by surgery, infection, or stress; significant mortality if untreated.
Diagnosis:
- ↓ TSH (most sensitive screen) with ↑ free T4 and/or ↑ free T3
- Thyroid-stimulating immunoglobulins (TSI) — positive in Graves disease
- Radioactive iodine uptake (RAIU): Diffusely increased in Graves; focal in toxic adenoma; decreased in thyroiditis
- Normal TSH range: 0.5–5 μU/mL
Treatment:
| Modality | Details |
|---|---|
| Antithyroid drugs | Methimazole (first-line), PTU (pregnancy/thyroid storm) — inhibit TPO |
| β-blockers | Propranolol — adjunct for symptomatic control (palpitations, tremor) |
| Radioactive iodine (¹³¹I) | Destroys thyroid tissue; first-line in many non-pregnant adults |
| Surgery | Total/near-total thyroidectomy — for large goiters, compression, failed medical Rx, pregnancy preference |
— Robbins & Kumar Basic Pathology, pp. 729–730; Schwartz's Principles of Surgery, pp. 1634–1642
B. HYPOTHYROIDISM
Pathophysiology:
Deficient thyroid hormone production, classified as:
- Primary (intrinsic thyroid failure — most common)
- Secondary/Central (pituitary or hypothalamic failure — rare)
Causes of Primary Hypothyroidism:
| Cause | Mechanism |
|---|---|
| Hashimoto thyroiditis | Autoimmune destruction |
| Iodine deficiency | ↓ Hormone synthesis (commonest cause worldwide — ~2 billion affected) |
| Post-surgery / Radiation | Loss of thyroid tissue |
| Drugs: lithium, amiodarone, iodides | Interference with synthesis |
| Congenital dysgenesis or enzyme defects | Absent/defective gland |
Symptoms (Myxedema in adults):
| System | Features |
|---|---|
| General | Fatigue, weight gain, cold intolerance, decreased sweating |
| Skin | Cool, pale, dry skin; non-pitting edema (myxedema — from glycosaminoglycan accumulation) |
| Cardiovascular | Bradycardia, reduced cardiac output, ↑ LDL/cholesterol, risk of atherosclerosis |
| CNS | Mental sluggishness, depression, memory impairment, slow reflexes |
| GI | Constipation |
| Voice/Face | Deep voice, coarsened facial features, macroglossia |
Congenital hypothyroidism (Cretinism):
- Iodine deficiency in utero → impaired skeletal and CNS development, severe mental disability, short stature, protruding tongue
Diagnosis:
- ↑ TSH (primary) — most sensitive test
- ↓ free T4
- Positive anti-TPO and anti-thyroglobulin antibodies in Hashimoto's
Treatment:
- Levothyroxine (T4) — standard replacement therapy; dose titrated to normalize TSH
- Monitor TSH every 6–12 months once stable
- Dose adjustments needed in pregnancy, aging, malabsorption
— Robbins & Kumar Basic Pathology, pp. 730–731; Schwartz's Principles of Surgery, p. 1638
C. THYROIDITIS
| Type | Pathogenesis | Clinical Features | Treatment |
|---|---|---|---|
| Hashimoto's (Chronic Lymphocytic) | Autoimmune — CD4+ T cells activate CD8+ cytotoxic T cells against thyroid antigens; anti-TPO + anti-Tg antibodies | Painless diffuse goiter, progressive hypothyroidism; middle-aged women; associated with B-cell NHL | Levothyroxine replacement |
| Subacute Granulomatous (de Quervain's) | Post-viral; self-limited | Painful, tender enlarged thyroid; fever; ESR >100; triphasic: hyper → eu → hypo → recovery | NSAIDs/aspirin; steroids for severe cases; β-blockers; self-resolves |
| Painless (Silent/Postpartum) | Autoimmune; postpartum variant at ~6 weeks | Painless goiter; transient hyperthyroidism then hypothyroidism | β-blockers + T4 replacement; usually self-limited |
| Riedel's | IgG4-related disease; extensive fibrosis | Hard, fixed ("woody") thyroid mass; compressive symptoms; usually euthyroid | Surgery for compressive symptoms; glucocorticoids |
— Robbins & Kumar Basic Pathology, p. 731; Schwartz's Principles of Surgery, pp. 1634–1638
D. GOITER
Pathogenesis:
- Most commonly due to iodine deficiency → ↓ T4/T3 → ↑ TSH → follicular cell hypertrophy/hyperplasia → diffuse goiter → over time, recurrent cycles produce multinodular goiter
- Endemic goiter: >10% of population affected in iodine-deficient regions
- Sporadic goiter: Young women; dietary goitrogens (cabbage, cauliflower), dyshormonogenesis
Clinical features:
- Neck enlargement (can be massive)
- Compressive symptoms: dysphagia, dyspnea, stridor, hoarseness
- Usually euthyroid but may develop hypothyroidism or autonomously hyperfunctioning nodules
E. THYROID NODULES & CANCER
Evaluation — Bethesda Classification for FNA Cytology:
| Category | Risk of Malignancy | Management |
|---|---|---|
| Nondiagnostic | 1–4% | Repeat FNA under ultrasound |
| Benign | <3% | Follow-up |
| AUS/FLUS | 5–15% | Repeat FNA or clinical follow-up |
| Follicular Neoplasm | 15–35% | Lobectomy |
| Suspicious for Malignancy | 60–75% | Lobectomy or total thyroidectomy |
| Malignant | 97–99% | Total thyroidectomy |
Thyroid Cancer Types:
| Type | Features |
|---|---|
| Papillary (~80%) | Psammoma bodies, "Orphan Annie" nuclei; excellent prognosis; spreads to lymph nodes |
| Follicular (~15%) | Spreads hematogenously; follicular adenoma vs. carcinoma distinguished only by capsular/vascular invasion |
| Medullary (~3–5%) | From C cells; produces calcitonin; associated with MEN2A/2B |
| Anaplastic (<2%) | Elderly; extremely aggressive; near-universal mortality within months |
Treatment:
- Lobectomy or total thyroidectomy depending on cancer type and risk stratification
- ¹³¹I ablation for papillary/follicular cancer post-operatively (to destroy residual tissue)
- TSH suppressive therapy with levothyroxine
- Thyroglobulin monitoring for recurrence after total thyroidectomy
- Small papillary cancers (<1 cm) — active surveillance is an accepted option
4. Diagnostic Summary
| Test | Interpretation |
|---|---|
| TSH (0.5–5 μU/mL) | Best initial screen; ↓ in hyperthyroidism, ↑ in primary hypothyroidism |
| Free T4 (normal ~1.0–1.8 ng/dL) | ↑ in hyperthyroidism, ↓ in hypothyroidism |
| Free T3 | Useful when T3 toxicosis suspected |
| Anti-TPO / Anti-Tg antibodies | Positive in Hashimoto's; also in Graves |
| TSI (Thyroid-stimulating immunoglobulins) | Specific for Graves disease |
| RAIU scan | Diffuse uptake = Graves; focal = toxic adenoma; low = thyroiditis |
| Thyroid ultrasound | First-line imaging for nodules |
| FNA biopsy | Gold standard for nodule cytology — Bethesda classification guides management |
| Calcitonin | Elevated in medullary thyroid carcinoma |
| Thyroglobulin (Tg) | Tumor marker for differentiated thyroid cancer follow-up post-thyroidectomy |
Sources:
- Schwartz's Principles of Surgery, 11th Ed., pp. 1625–1660
- Robbins & Kumar Basic Pathology, pp. 729–737
- Costanzo Physiology, 7th Ed., pp. 427–430
- Peng B et al. (2024). Effects of supplements on Hashimoto's thyroiditis: systematic review and network meta-analysis. Front Endocrinol [PMID: 39698034]
Jaundice,types , pathophysiology, symptoms sign diagnosis and treatment in detail
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.