Explain me cephalosporins from basic to clinics drug of choice
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Katzung and Goodman & Gilman. Let me compile the complete, detailed answer.
Cephalosporins: From Basic Science to Clinical Drug of Choice
1. HISTORICAL OVERVIEW
Cephalosporins were first isolated in 1945 from the fungus Cephalosporium acremonium by Brotzu, who noticed the seawater near a Sardinian sewage outlet had antibacterial activity. The core compound, 7-aminocephalosporanic acid (7-ACA), forms the scaffold on which all modern cephalosporins are built. They are now the most widely prescribed class of antibiotics globally.
2. BASIC CHEMISTRY
All cephalosporins share a bicyclic nucleus: a beta-lactam ring (4-membered) fused to a dihydrothiazine ring (6-membered) - this is called the 7-aminocephalosporanic acid (7-ACA) nucleus. This differs from penicillins, which have a 5-membered thiazolidine ring (forming 6-aminopenicillanic acid, 6-APA).
Two key modification sites determine activity:
- R1 side chain at position 7 (C-7) - determines antibacterial spectrum and beta-lactamase stability
- R2 side chain at position 3 (C-3) - influences pharmacokinetics and metabolic stability
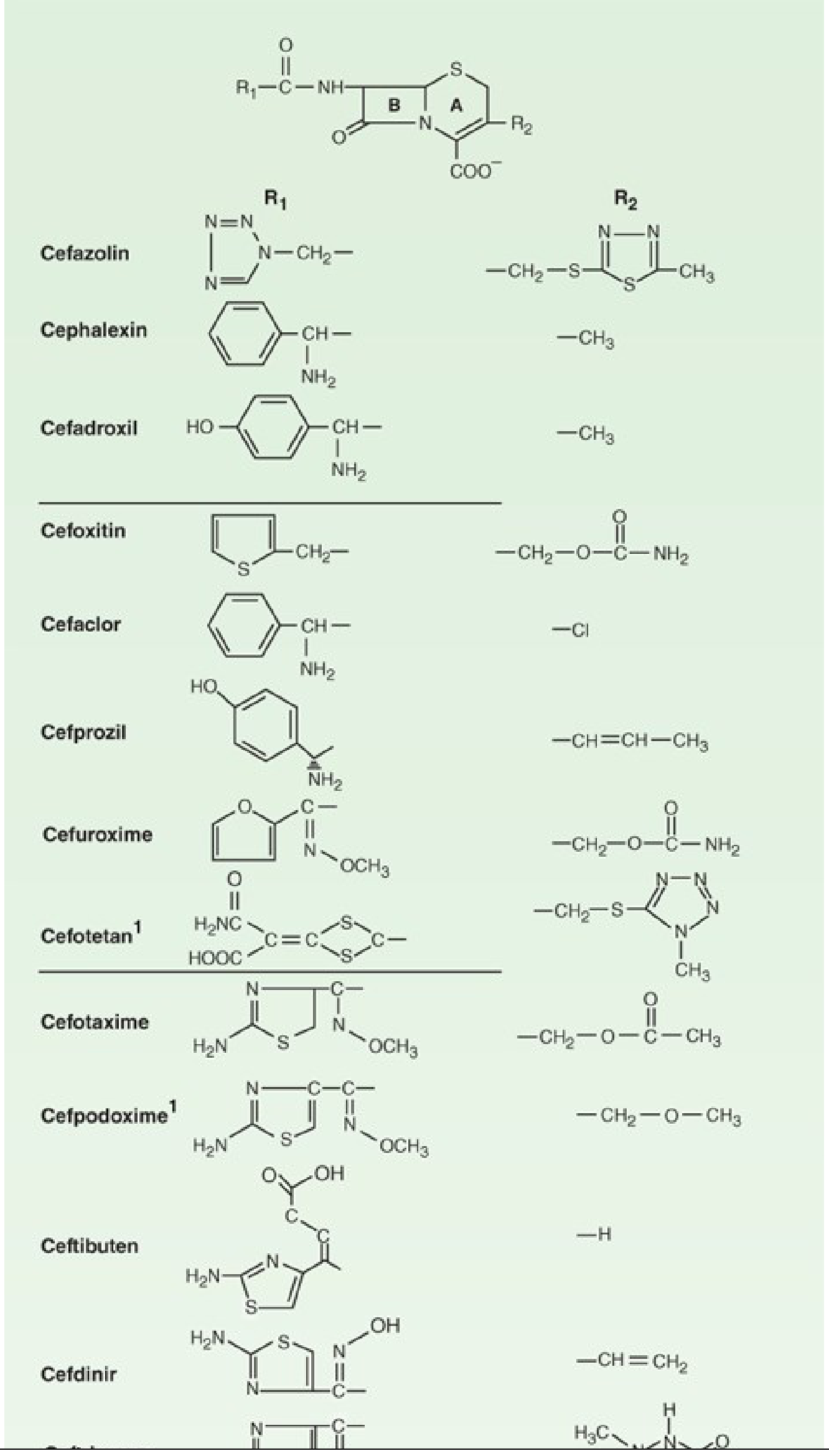
(Katzung, Figure 43-6: R1 and R2 substituents on the 7-ACA nucleus)
3. MECHANISM OF ACTION
Cephalosporins are bactericidal and work by inhibiting bacterial cell wall synthesis:
- Binding to Penicillin-Binding Proteins (PBPs) - transpeptidases and carboxypeptidases on the bacterial inner membrane
- Inhibition of cross-linking of peptidoglycan chains (transpeptidation step) - the final step in cell wall synthesis
- Cell wall weakening leads to osmotic lysis and bacterial death
- Activation of autolysins contributes to bacterial killing
They are time-dependent antibiotics - efficacy correlates with the %T > MIC (percentage of dosing interval that free drug concentration exceeds the MIC), not peak concentration.
4. MECHANISMS OF RESISTANCE
| Mechanism | Detail |
|---|---|
| Beta-lactamase production | Most common - enzymes hydrolyze the beta-lactam ring (e.g., ESBLs, AmpC, KPCs, MBLs) |
| Altered PBPs | MRSA expresses PBP2a (encoded by mecA gene) with very low affinity for most cephalosporins |
| Reduced outer membrane permeability | Loss of porins (OmpF, OmpC) in gram-negatives limits entry |
| Efflux pumps | Active pumping out of the drug (e.g., MexAB-OprM in P. aeruginosa) |
| AmpC induction | In Enterobacter, Citrobacter, Serratia - inducible chromosomal AmpC derepression occurs with 2nd/3rd gen exposure |
Important: "ESCAPPM" or "SPICE" organisms (Serratia, Pseudomonas, indole-positive Proteus, Citrobacter, Enterobacter) harbor inducible AmpC beta-lactamases. Even if in vitro susceptibility is shown to 2nd/3rd-gen cephalosporins, clinical failure can occur - these should be avoided or used with caution in serious infections.
5. GENERATIONS OF CEPHALOSPORINS
The generational classification reflects an expanding gram-negative spectrum with each generation while gram-positive coverage (except for 5th gen) relatively decreases.
Key Rule:
With each generation, gram-negative coverage expands, gram-positive activity relatively decreases, and beta-lactamase stability increases.
FIRST GENERATION
Agents: Cefazolin (IV/IM), Cephalexin (oral), Cefadroxil (oral)
Spectrum:
- Excellent gram-positive: Streptococci, MSSA (methicillin-sensitive S. aureus)
- Limited gram-negative: E. coli, K. pneumoniae, P. mirabilis (the "3 E-K-P" organisms)
- No activity: MRSA, enterococci, Pseudomonas, Bacteroides fragilis
Pharmacokinetics:
- Cephalexin oral: peak serum ~15-20 mcg/mL after 500 mg; given 250-500 mg four times daily
- Cefazolin IV: peak ~185 mcg/mL after 1g infusion; dosed 0.5-2 g IV every 8 hours
- Renal excretion (dose adjust in renal failure); cefazolin does NOT penetrate the CNS
Drug of Choice / Clinical Uses:
| Indication | Drug |
|---|---|
| Surgical prophylaxis | Cefazolin (DOC for most clean/clean-contaminated surgeries) |
| Skin/soft tissue infections (MSSA, strep) | Cephalexin (oral), Cefazolin (IV) |
| MSSA bacteremia/sepsis | Cefazolin (preferred over antistaphylococcal PCN due to tolerability) |
| UTI (susceptible E. coli/Klebsiella) | Cephalexin oral |
| Mild penicillin allergy (non-immediate) | Cefazolin can be substituted |
SECOND GENERATION
Agents: Cefuroxime (oral/IV), Cefoxitin (IV), Cefotetan (IV), Cefaclor (oral), Cefprozil (oral)
Spectrum: Extended gram-negative vs. 1st gen, retained gram-positive activity
- Cefuroxime: adds H. influenzae, Moraxella catarrhalis, Neisseria coverage; useful for community-acquired pneumonia
- Cefoxitin/Cefotetan (cephamycins): extended anaerobic activity including B. fragilis; used in mixed aerobic-anaerobic infections
- Still no activity against Pseudomonas, enterococci, MRSA
Pharmacokinetics:
- Cefuroxime IV: serum levels 75-125 mcg/mL after 1g; oral dose 250-500 mg twice daily
- Cefoxitin: short half-life, given every 6-8 hours
Drug of Choice / Clinical Uses:
| Indication | Drug |
|---|---|
| Surgical prophylaxis (colorectal/gynecologic) | Cefoxitin or Cefotetan (anaerobic coverage needed) |
| Community-acquired pneumonia (mild, outpatient) | Cefuroxime axetil |
| Sinusitis, otitis media, bronchitis (H. influenzae) | Cefuroxime axetil |
| Pelvic inflammatory disease (with doxycycline) | Cefoxitin IV |
| Intra-abdominal infections (mild-moderate) | Cefoxitin/Cefotetan |
| Lyme disease (early disseminated) | Cefuroxime axetil |
THIRD GENERATION
Agents:
- Parenteral: Ceftriaxone, Cefotaxime, Ceftazidime, Cefoperazone
- Oral: Cefixime, Cefdinir, Cefpodoxime, Ceftibuten
Spectrum:
- Markedly enhanced gram-negative coverage (most Enterobacterales)
- Ceftriaxone/Cefotaxime: excellent streptococcal activity (best among 3rd gen)
- Ceftazidime: unique activity against Pseudomonas aeruginosa (but weaker gram-positive)
- All: penetrate CSF adequately for meningitis
- Activity reduced vs. ESBL-producing organisms
Pharmacokinetics:
- Ceftriaxone: half-life 7-8 hours - once-daily dosing possible; excreted via biliary tract (no dose adjustment for renal failure)
- Cefotaxime: half-life ~1 hour; metabolized to desacetylcefotaxime; given every 4-8 hours
- Cefixime oral: half-life 3-4 hours; 400 mg once daily
Drug of Choice / Clinical Uses:
| Indication | Drug |
|---|---|
| Bacterial meningitis (empiric, >1 month) | Ceftriaxone or Cefotaxime + Vancomycin (for resistant pneumococcus) |
| Gonorrhea (uncomplicated urogenital) | Ceftriaxone 500 mg IM single dose (now 500 mg due to rising resistance) |
| Community-acquired pneumonia (moderate-severe, hospitalized) | Ceftriaxone + macrolide or fluoroquinolone |
| Typhoid fever | Ceftriaxone IV (DOC in severe disease) |
| Lyme neuroborreliosis | Ceftriaxone IV |
| Pyelonephritis/severe UTI | Ceftriaxone or Cefotaxime |
| Meningococcemia/disseminated gonococcal infection | Ceftriaxone |
| Pseudomonal infections | Ceftazidime IV |
| H. influenzae meningitis | Ceftriaxone or Cefotaxime |
| Outpatient UTI / otitis media (oral) | Cefdinir, Cefpodoxime, Cefixime |
| Empiric sepsis (community-acquired) | Ceftriaxone |
Caution: Do not use 3rd-gen cephalosporins for Enterobacter, Citrobacter, Serratia serious infections - AmpC derepression causes treatment failure even when the isolate appears susceptible in vitro. - Katzung, p. 1251
Neonates: Avoid ceftriaxone - biliary displacement of bilirubin can cause kernicterus. Use cefotaxime instead. - Goodman & Gilman, p. 967
FOURTH GENERATION
Agent: Cefepime (IV/IM only)
Spectrum: Combines best of 1st and 3rd gen:
- Good gram-positive: MSSA, S. pneumoniae (including PCN-non-susceptible strains)
- Broad gram-negative: Pseudomonas aeruginosa + Enterobacterales
- More resistant to chromosomal AmpC beta-lactamases than 3rd gen
- Penetrates CSF well
Pharmacokinetics: Half-life ~2 hours; renally cleared; dose adjust in renal failure
Drug of Choice / Clinical Uses:
| Indication | Drug |
|---|---|
| Febrile neutropenia (empiric) | Cefepime (monotherapy in non-high-risk) |
| Hospital-acquired pneumonia / VAP (Pseudomonas risk) | Cefepime |
| Enterobacter serious infections | Cefepime (preferred over 3rd-gen due to AmpC stability) |
| Nosocomial sepsis (non-MRSA) | Cefepime |
| Meningitis due to gram-negative enteric rods | Cefepime |
Cefepime is the only fourth-generation cephalosporin currently available in the USA. - Katzung, p. 1251
FIFTH GENERATION (ANTI-MRSA CEPHALOSPORINS)
Agents: Ceftaroline (IV, USA-approved), Ceftobiprole (IV, not USA-approved)
Mechanism of the added feature: Modified R1 side chain allows binding to PBP2a (the low-affinity PBP encoded by mecA that confers MRSA resistance) - this is unique among cephalosporins
Spectrum:
- MRSA (>95% of isolates inhibited) - the distinguishing feature
- Penicillin-resistant S. pneumoniae
- Gram-negative coverage similar to cefotaxime (NOT Pseudomonas)
- No activity against VRE or Acinetobacter
Drug of Choice / Clinical Uses:
| Indication | Drug |
|---|---|
| MRSA skin/soft tissue infections | Ceftaroline (alternative to vancomycin) |
| Community-acquired pneumonia (MRSA possible) | Ceftaroline |
| MRSA bacteremia (salvage) | Ceftaroline |
SIDEROPHORE CEPHALOSPORINS (Novel)
Agent: Cefiderocol
Mechanism: Uses the bacterial iron-uptake system ("Trojan horse" - siderophore-conjugated) to bypass outer membrane barriers; extremely broad gram-negative spectrum including carbapenem-resistant organisms (CROs)
Indication: Carbapenem-resistant gram-negative infections (last-resort agent)
6. SPECTRUM SUMMARY TABLE
| Generation | Key Gram (+) | Key Gram (-) | Notable Gaps | Prototype Drug |
|---|---|---|---|---|
| 1st | MSSA, Strep | E. coli, Klebsiella, P. mirabilis | Pseudomonas, MRSA, Bacteroides | Cefazolin |
| 2nd | MSSA, Strep | Above + H. influenzae, Moraxella | Pseudomonas, MRSA | Cefuroxime |
| 2nd (cephamycins) | Moderate | Enterobacterales | Pseudomonas, MRSA | Cefoxitin |
| 3rd | Strep (reduced staph) | Broad Enterobacterales | MRSA, Enterococcus | Ceftriaxone |
| 3rd (anti-pseudomonal) | Weaker | Enterobacterales + Pseudomonas | MRSA | Ceftazidime |
| 4th | MSSA, Strep (including PCN-R) | Broad + Pseudomonas + AmpC-stable | MRSA | Cefepime |
| 5th | MRSA, MSSA, Strep | Enterobacterales (not Pseudomonas) | Pseudomonas, VRE | Ceftaroline |
7. ADVERSE EFFECTS
| Adverse Effect | Details |
|---|---|
| Hypersensitivity | Most common concern; maculopapular rash, urticaria; anaphylaxis rare. Cross-reactivity with penicillins is ~1-2% (much less than the previously quoted 10%) - primarily determined by shared R1 side chains, not the beta-lactam core |
| GI disturbance | Diarrhea, especially cefoperazone (biliary excretion); C. difficile colitis risk |
| Coombs test positivity | Common with high doses; hemolysis rare |
| Biliary pseudolithiasis | Ceftriaxone - precipitates in bile due to high biliary excretion and calcium binding |
| Kernicterus risk | Ceftriaxone displaces bilirubin from albumin - contraindicated in neonates |
| Disulfiram-like reaction | Cephalosporins with methylthiotetrazole (MTT) ring: Cefotetan, Cefoperazone - avoid alcohol |
| Hypoprothrombinemia | MTT side chain drugs (cefazolin, cefotetan, cefoperazone) can prolong PT |
| Nephrotoxicity | Rare alone; potentiated by aminoglycosides or loop diuretics |
| Seizures | High-dose Cefepime, especially in renal impairment - neurotoxicity |
8. CROSS-REACTIVITY WITH PENICILLINS
The old teaching of 10% cross-reactivity is outdated. Modern data shows:
- Cross-reactivity is ~1-2% and is driven by shared R1 side chains between specific penicillins and cephalosporins, not the beta-lactam ring itself
- Patients with mild/distant penicillin reactions: low risk - cephalosporins generally safe
- Patients with severe immediate hypersensitivity (anaphylaxis) to penicillin: skin test first or use cautious graded challenge before giving a cephalosporin - Goodman & Gilman, p. 964
- Cephalosporins may be used in patients with PCN-induced maculopapular rashes but avoided in those with anaphylactic history - Katzung
9. QUICK CLINICAL CHEAT SHEET - DRUGS OF CHOICE
| Clinical Scenario | Cephalosporin of Choice |
|---|---|
| Surgical prophylaxis (most surgeries) | Cefazolin 1st gen |
| MSSA bacteremia | Cefazolin |
| Bacterial meningitis (empiric, community) | Ceftriaxone + Vancomycin |
| Gonorrhea (uncomplicated) | Ceftriaxone 500 mg IM |
| Community-acquired pneumonia (hospitalized) | Ceftriaxone + macrolide |
| Typhoid fever (severe) | Ceftriaxone |
| Lyme neuroborreliosis | Ceftriaxone |
| Febrile neutropenia | Cefepime |
| Pseudomonal infection | Ceftazidime or Cefepime |
| Nosocomial HAP/VAP (Pseudomonas risk) | Cefepime or Ceftazidime |
| MRSA skin/soft tissue infection | Ceftaroline |
| Pelvic inflammatory disease / intra-abdominal (anaerobic) | Cefoxitin (2nd gen cephamycin) |
| Colorectal surgery prophylaxis | Cefoxitin or Cefotetan |
| Pediatric meningitis | Cefotaxime (avoid ceftriaxone in neonates) |
| Carbapenem-resistant gram-negative | Cefiderocol |
10. RENAL DOSING NOTE
Nearly all cephalosporins require dose adjustment in renal failure except ceftriaxone (biliary excretion). Cefazolin, cefepime, and ceftazidime in particular accumulate in renal failure; cefepime accumulation is associated with neurotoxicity and seizures.
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed., Ch. 43, pp. 1247-1258; Goodman & Gilman's Pharmacological Basis of Therapeutics, pp. 901-975; Lippincott Illustrated Reviews Pharmacology, pp. 964-969
This is a shared conversation. Sign in to Orris to start your own chat.