Rhino manometry 10 marks for ms ent exam
Reading File
Finding Sources
Finding Sources
Searching the Web
rhinomanometry ENT exam 10 marks nasal airway resistance measurement
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from both major textbooks to write a thorough 10-mark MS ENT exam answer. Let me compile the complete answer.
Rhinomanometry
(Scott-Brown's Otorhinolaryngology, p. 1039-1040; Cummings Otolaryngology, p. 767)
Definition
Rhinomanometry is the simultaneous measurement of nasal airflow and trans-nasal pressure from which nasal airway resistance (NAR) can be calculated. It is a functional, objective test of nasal patency. The term "rhinomanometry" reflects that the technique uses manometers (differential pressure transducers) to measure pressure across the nasal airway.
Principle
Nasal airway resistance is derived from two simultaneous measurements:
- Trans-nasal pressure (ΔP) - the pressure difference between the posterior nares and the nostril entrance (atmospheric or mask pressure)
- Nasal airflow (V) - measured by a flow head consisting of a mesh resistance inside a tube; the pressure drop across the mesh is proportional to airflow
Resistance formula:
$$R = \frac{\Delta P}{V}$$
Where:
- R = nasal airway resistance (Pa/cm³/s, or cm H₂O/L/s)
- ΔP = trans-nasal pressure (Pa or cm H₂O)
- V = nasal airflow (cm³/s or L/s)
Total nasal resistance (combining both sides measured separately by anterior method):
$$\frac{1}{R_{total}} = \frac{1}{R_{left}} + \frac{1}{R_{right}}$$
Classification of Rhinomanometry
1. Active vs. Passive
| Type | Airflow Source |
|---|---|
| Active | Patient's own normal breathing |
| Passive | External source (fan/pump) drives air through the nose - useful for separating upper and lower airways in research |
2. Anterior vs. Posterior (Active rhinomanometry)
Active Anterior Rhinomanometry (AAR)
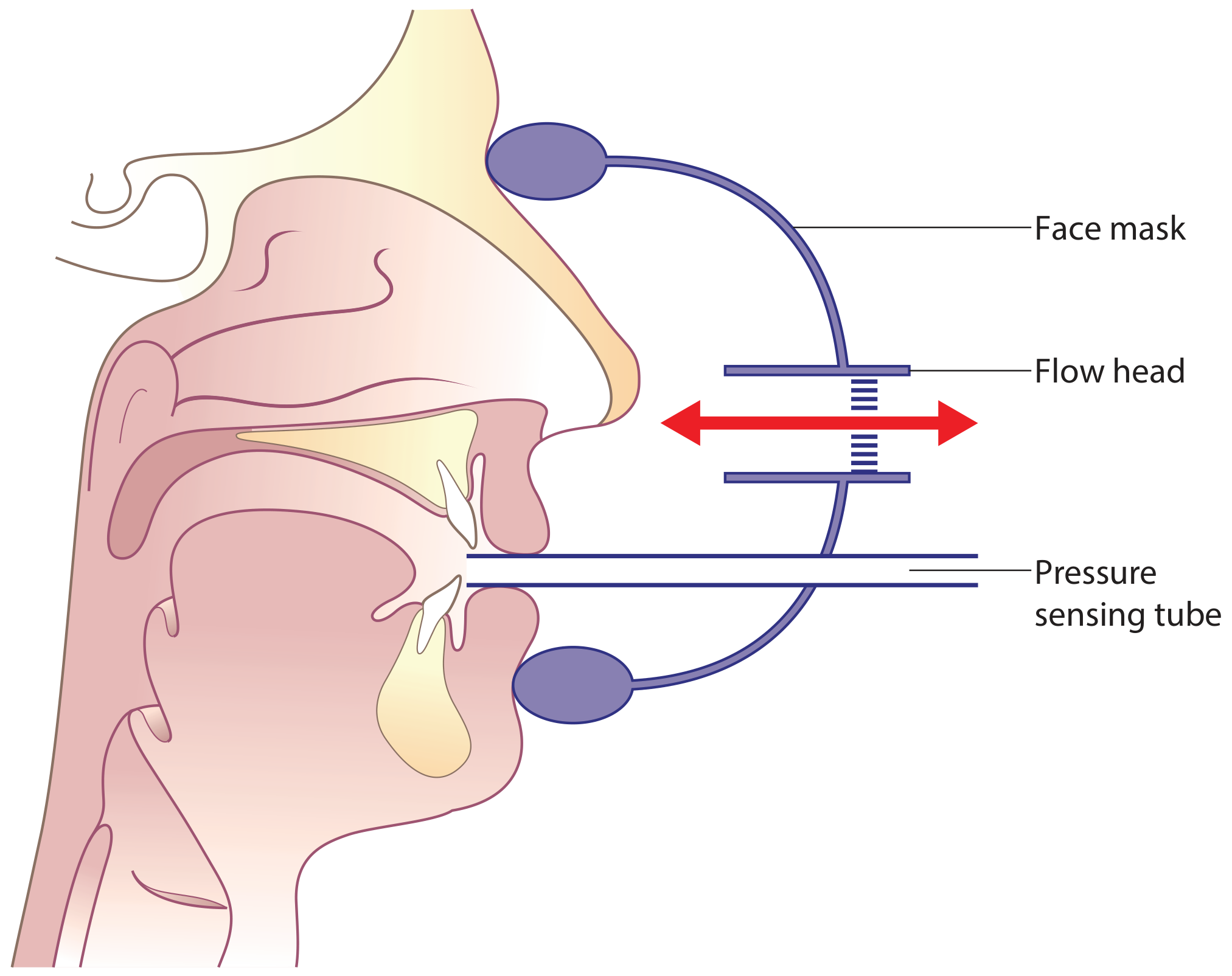
Technique of posterior rhinomanometry (Scott-Brown's Fig 90.1) - the pressure sensing tube in the mouth detects posterior nares pressure while the face mask measures total nasal airflow
- The pressure-sensing tube is taped to one nostril (sealing it), which then acts as an extension to measure posterior nares pressure
- Airflow is measured from the other (open) nostril
- The sides are tested one at a time (tube moved from side to side)
- Resistance is determined separately for each side, then total resistance calculated using the above formula
- Most commonly used clinical method, recommended by international standardization committees
- Limitation: Cannot be used when nasal septal perforation is present (the sealed nostril cannot accurately sense posterior pressure)
Active Posterior Rhinomanometry
- The pressure-sensing tube is held in the mouth, detecting posterior nares pressure when the soft palate is open
- Total nasal airflow from both nostrils simultaneously can be measured
- Total nasal resistance is determined directly from total airflow and trans-nasal pressure
- Advantage: Total resistance measured directly without calculations
- Limitation: Not all patients can maintain an open soft palate airway to mouth; requires coaching; achievable in ~90% of subjects with training
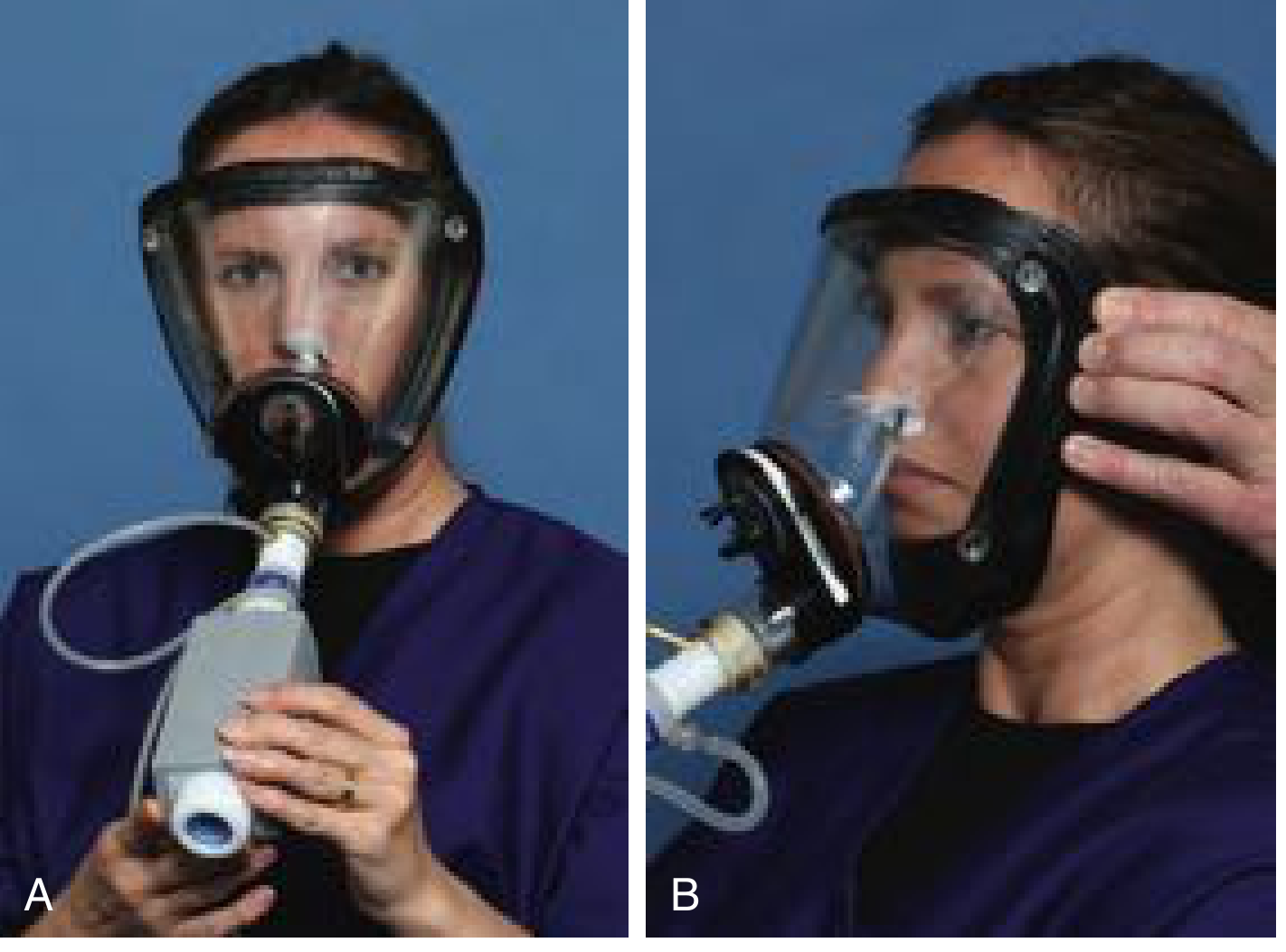
Patient performing anterior active rhinomanometry (Cummings Fig 37.2). Left: front view. Right: lateral view showing pressure tube at the contralateral nostril.
Standard Measurement Points
- Unilateral (anterior method): sample pressure point of 150 Pa
- Bilateral (posterior method): sample pressure point of 75 Pa
- For Asian populations: 100 Pa and 50 Pa respectively (due to smaller body size and smaller lung volumes making the standard 150 Pa unachievable during quiet breathing)
The Pressure-Flow Curve
- Plotting ΔP (x-axis) vs. flow (y-axis) produces a curvilinear (sigmoid-shaped) relationship
- Nasal airflow increases with rising pressure, but at higher pressures turbulent airflow effects limit further flow increase
- Because the curve is non-linear, resistance cannot be read from the slope alone - it is defined at a fixed standard sample pressure point
- A more obstructed airway produces a curve lying closer to the pressure axis (greater pressure required to generate a given flow)
- Flattening of the curve distally at a single flow rate suggests nasal valve/alar collapse
Normal Values
| Parameter | Normal Range |
|---|---|
| Total NAR (adults) | ~0.15-0.25 Pa/cm³/s (at 150 Pa) |
| Children | Higher NAR than adults (decreases with age) |
| Girls | Lower NAR than boys (posterior RM data) |
4-Phase Rhinomanometry (4PR)
An advance on classic rhinomanometry introduced by Vogt et al. (2010):
- Classic AAR uses a single fixed pressure point (150 Pa) for NAR calculation
- 4PR calculates NAR across all four phases of the breathing cycle (acceleration/deceleration of inspiration and expiration)
- Parameters measured:
- Vertex Resistance (VR) - resistance at peak flow point; best correlates with symptom of nasal obstruction
- Effective Resistance (Reff) - across entire breath
- ReffIn / ReffEx - inspiratory and expiratory components
- Advantage: A result can be obtained even in patients who cannot reach 150 Pa during quiet breathing
- 4PR and classic RM do not significantly differ in outcomes
Clinical Applications
- Pre- and post-operative assessment - septoplasty, turbinoplasty, functional rhinoplasty; objective documentation of surgical improvement
- Nasal challenge tests - allergen, exercise, or pharmacological challenges to assess mucosal reactivity
- Drug trials - assessing efficacy of decongestants, antihistamines, nasal steroids
- Diagnosis of nasal obstruction - distinguishing structural vs. mucosal causes
- Nasal cycle research - physiological alternating congestion/decongestion
- Positional assessment - can be performed supine to evaluate recumbent nasal obstruction
- Pediatric assessment - feasible from ~2 years of age with smaller face mask
Sources of Error and Standardization
- Mask leak is the most common error - multiple measurements with repositioning of the mask between readings are mandatory
- A single measurement of nasal airway resistance is unreliable
- A standard operating procedure (SOP) must be implemented to prevent investigator bias
- Equipment must be accurately calibrated before measurements
- The International Standards Committee (Clement 1984) has defined standardized methods for reporting
Comparison with Acoustic Rhinometry
| Feature | Rhinomanometry | Acoustic Rhinometry |
|---|---|---|
| Measures | Airflow + pressure (functional) | Nasal cross-sectional area (anatomical) |
| Output | Nasal resistance | Minimum cross-sectional area, nasal volume |
| Nature | Dynamic (during breathing) | Static (at rest) |
| Clinical use | Functional nasal obstruction | Anatomical mapping of nasal cavity |
| Septal perforation | Anterior method contraindicated | Not affected |
Key Points for Exam
- Rhinomanometry = simultaneous measurement of nasal airflow + trans-nasal pressure to compute NAR
- Formula: R = ΔP / V (resistance = pressure / flow)
- Anterior active = most used clinically; one nostril at a time; pressure tube taped to contralateral closed nostril
- Posterior active = pressure tube in mouth; measures both sides simultaneously; cannot be used if patient cannot keep soft palate open
- Standard sample pressures: 150 Pa (unilateral), 75 Pa (bilateral)
- P-F curve is curvilinear/sigmoid; resistance reported at a fixed pressure point
- Total resistance formula: 1/R(total) = 1/R(left) + 1/R(right)
- 4-phase rhinomanometry analyzes all four phases of breathing - better for patients who can't reach 150 Pa
- Important for pre/post-op objective documentation in nasal surgery
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1 (p. 1039-1040); Cummings Otolaryngology Head and Neck Surgery (p. 767)
This is a shared conversation. Sign in to Orris to start your own chat.