Infective endocarditis
Reading File
Finding Sources
Searching PubMed
"infective endocarditis"[MeSH Terms] AND ("diagnosis" OR "management")
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have all the information needed for a comprehensive, well-structured answer. Let me compile it.
Infective Endocarditis (IE)
Definition
Infective endocarditis is a microbial infection of the heart valves or endocardium leading to the formation of vegetations - friable masses composed of thrombotic debris, inflammatory cells, and organisms - often with destruction of the underlying cardiac tissue. The aorta, aneurysmal sacs, other blood vessels, and prosthetic devices may also be infected. The vast majority of cases are bacterial, though fungi, rickettsiae (Q fever), and chlamydia can also be responsible.
- Robbins & Kumar Basic Pathology, p. 368
Classification
| Type | Course | Features |
|---|---|---|
| Acute IE | Days to weeks | Rapidly destructive, high morbidity/mortality even with therapy; caused by virulent organisms (e.g., S. aureus) on normal or abnormal valves |
| Subacute IE | Weeks to months | Insidious onset; most recover with antibiotics; caused by less virulent organisms (e.g., viridans streptococci) on damaged valves |
Epidemiology
- Annual incidence: ~3-14 cases per 100,000 persons/year in Western countries
- In developing countries: predominantly subacute IE from viridans streptococci on rheumatic heart disease valves
- In developed countries: predominantly S. aureus, often healthcare-associated or linked to injection drug use (IDU)
- S. aureus has become the most common cause in most high-income countries due to increasing medical interventions
- Prosthetic valve IE (PVE) accounts for 10-20% of all IE cases
Braunwald's Heart Disease, p. 3529-3535
Microbiology
| Organism | Setting | Notes |
|---|---|---|
| Staphylococcus aureus | Healthcare, IDU, prosthetic valves | Most common cause in high-income countries; MRSA increasingly prevalent; attacks normal and diseased valves |
| Viridans group streptococci | Community; native damaged valves | 50-60% of community-acquired cases; oral flora; subacute presentation |
| Enterococci | Healthcare, GI/GU tract | Ampicillin + gentamicin or ampicillin + ceftriaxone regimen |
| HACEK group | Community-acquired | Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella; 5-10% of community IE; slow-growing gram-negatives |
| Coagulase-negative staph | Prosthetic valves | S. epidermidis, S. lugdunensis |
| Fungi | IDU, immunocompromised | Rare; Candida in early PVE |
| Culture-negative | ~10% | Prior antibiotics, or fastidious organisms (Coxiella burnetii, Bartonella, Brucella, Tropheryma whipplei, Legionella) |
Robbins & Kumar, p. 368; Washington Manual of Medical Therapeutics, p. 5461
Pathogenesis
- Predisposing cardiac lesion - turbulent flow disrupts endothelium, creating a sterile platelet-fibrin thrombus (NBTE)
- Bacteremia - organisms seed the thrombus (dental procedures, IV lines, skin infections, IDU, gut bacteria)
- Vegetation formation - organisms proliferate within the thrombus, which expands with more fibrin and platelets
- Local destruction - leaflet perforation, annular abscess, ring abscess (can extend to conduction system)
- Embolization - friable vegetations shed septic emboli to brain, kidneys, spleen, lungs
Predisposing cardiac conditions:
- Mitral valve prolapse (now the leading pre-existing risk factor as rheumatic disease declines)
- Bicuspid aortic valve
- Calcific valvular stenosis
- Rheumatic heart disease
- Congenital heart disease (VSD)
- Prosthetic heart valves
- Intracardiac devices, pacemaker leads
Robbins & Kumar Basic Pathology, p. 368; Washington Manual, p. 5466
Morphology of Vegetations
The diagram below illustrates how vegetations in IE (bulky, destructive) compare to other forms of valvular endocarditis:
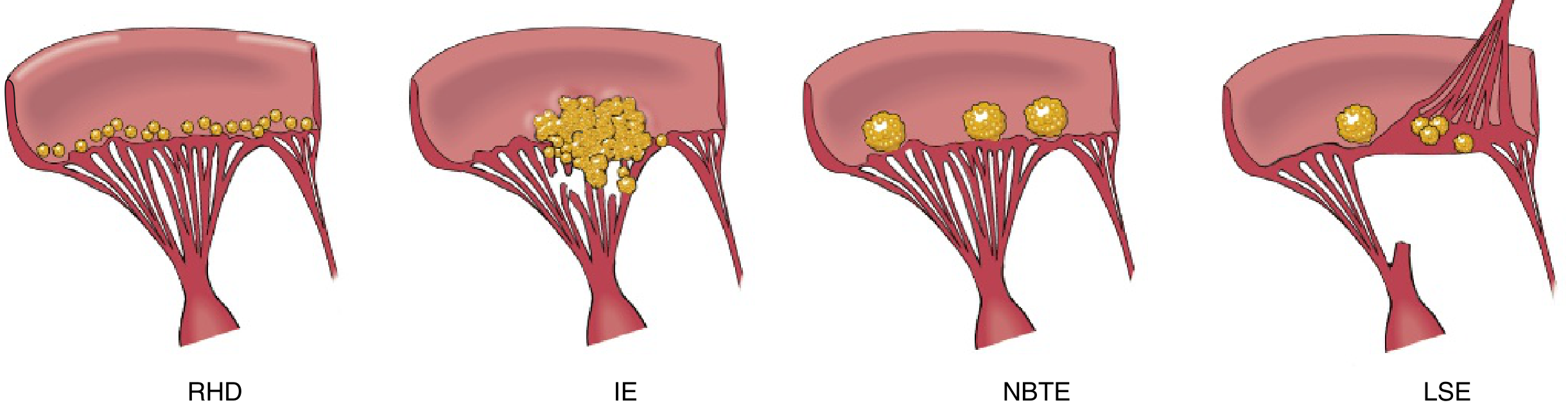
- RHD: Small beaded deposits along the line of closure
- IE: Large, friable, destructive vegetations with organisms; can invade underlying myocardium → ring abscess
- NBTE: Small, sterile, non-destructive vegetations on previously normal valves
- LSE (Libman-Sacks): Small, irregular lesions on both sides of the leaflet (SLE)
Most common valves affected: aortic and mitral (left-sided). Tricuspid is the dominant site in IDU.
Robbins & Kumar Basic Pathology, p. 368
Clinical Features
Classic Signs
- Fever - the most consistent sign (may be absent in subacute IE in elderly)
- New or changing cardiac murmur - present in 90% of left-sided IE
- Splenomegaly - more common in subacute IE
Peripheral Stigmata (from emboli or immune complex deposition)
| Sign | Description | Mechanism |
|---|---|---|
| Petechiae | Small pinpoint hemorrhages (skin, conjunctiva) | Emboli/vasculitis |
| Splinter hemorrhages | Linear subungual hemorrhages | Microemboli |
| Janeway lesions | Painless erythematous macules on palms/soles | Septic emboli |
| Osler nodes | Painful tender nodules on fingertips/toes | Immune complex deposition |
| Roth spots | Retinal hemorrhages with pale center | Emboli |
Janeway lesions = painless (embolic); Osler nodes = pAinful (immune)
Complications
- Local: Valvular destruction, perivalvular abscess, intracardiac fistula, heart block (from conduction system involvement), acute heart failure
- Embolic: Stroke (brain), renal/splenic infarcts, septic pulmonary emboli (right-sided IE), mycotic aneurysms
- Immune: Glomerulonephritis (immune complex-mediated), rheumatoid factor, arthralgias
Robbins & Kumar, p. 368-369; Washington Manual, p. 5574-5578
Diagnosis: Modified Duke Criteria
DEFINITE IE
- 2 major criteria, OR
- 1 major + 3 minor criteria, OR
- 5 minor criteria
POSSIBLE IE
- 1 major + 1 minor, OR 3 minor criteria
REJECTED IE
- Firm alternate diagnosis, or resolution with antibiotics ≤4 days
Major Criteria
1. Microbiologic:
- Two separate blood cultures with typical IE organisms (S. viridans, S. gallolyticus, S. aureus, HACEK, Enterococcus without primary focus)
- Persistently positive blood cultures: ≥2 cultures drawn >12 hours apart, OR all of 3 or majority of 4 cultures drawn ≥1 hour apart
- Single positive culture for Coxiella burnetii (Q fever) or antiphase 1 IgG titer ≥1:800
- Positive PCR from blood for C. burnetii, Bartonella, or T. whipplei
2. Imaging/Echocardiographic:
- Vegetation, valvular perforation/aneurysm, abscess, pseudoaneurysm, intracardiac fistula
- New valvular regurgitation
- New abnormal activity on 18F-FDG PET/CT (useful especially in PVE)
Minor Criteria
- Predisposing heart condition or IDU
- Fever ≥38°C
- Vascular phenomena: major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, Janeway lesions
- Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
- Positive blood culture not meeting major criteria (or serological evidence of active infection with organism consistent with IE)
Textbook of Clinical Echocardiography (2023 Duke Criteria); Washington Manual, p. 5477-5565
Investigations
| Test | Details |
|---|---|
| Blood cultures | 3 sets from separate sites, 30 minutes apart, BEFORE antibiotics; most important diagnostic test |
| TTE (Transthoracic Echo) | First-line; sensitivity 50-60%; cannot rule out IE if negative |
| TEE (Transesophageal Echo) | Sensitivity ~90%; first-line for suspected PVE, perivalvular abscess, poor TTE quality, or high clinical suspicion |
| 18F-FDG PET/CT | Useful for PVE; role in native valve IE still under study |
| CBC, ESR, CRP | Nonspecific markers of infection/inflammation |
| Urinalysis | Hematuria, proteinuria (glomerulonephritis) |
Washington Manual, p. 5587-5597
Treatment
Empirical Therapy (before cultures)
- Native valve suspected: Vancomycin 15 mg/kg IV q12h (covers MRSA and streptococci)
- S. aureus confirmed: If MSSA - switch to oxacillin 2g IV q4h (superior to vancomycin for MSSA)
Specific Antibiotic Regimens
| Organism | Regimen | Duration |
|---|---|---|
| VGS/S. gallolyticus (MIC <0.12 μg/mL) | Penicillin G (12-18 MU/day) or ceftriaxone 2g/day ± gentamicin | 4 weeks (± 2-wk gent) |
| VGS (MIC 0.12-0.5 μg/mL) | Penicillin G + gentamicin | 4 weeks |
| Penicillin allergy | Vancomycin 15 mg/kg IV q12h | 4-6 weeks |
| Enterococcus (PCN-susceptible) | Ampicillin 2g IV q4h + gentamicin OR ampicillin + ceftriaxone | 4-6 weeks |
| Enterococcus (PCN-resistant) | Vancomycin + gentamicin | 6 weeks |
| VRE | Linezolid 600 mg q12h or daptomycin ≥10 mg/kg/day | ≥6 weeks |
| MSSA (native valve) | Oxacillin/nafcillin 2g IV q4h | 4-6 weeks |
| MRSA | Vancomycin OR daptomycin | 4-6 weeks |
Washington Manual of Medical Therapeutics, p. 5615-5636; Goodman & Gilman's Pharmacological Basis of Therapeutics
Infectious diseases consultation is strongly recommended to guide antimicrobial selection and duration.
Surgical Indications (AHA Guidelines)
Native Valve IE - Class I (Early Surgery Required)
- Valve dysfunction causing symptoms of heart failure
- IE caused by fungal or highly resistant organisms (e.g., VRE, MDR gram-negatives)
- IE complicated by heart block, annular/aortic abscess, or destructive penetrating lesions
- Persistent bacteremia or fever >5-7 days despite appropriate antibiotics
Native Valve IE - Class IIa (Early Surgery Reasonable)
- Recurrent emboli + persistent/enlarging vegetations despite antibiotics
- Severe valve regurgitation + mobile vegetations >10 mm
Right-Sided IE
- Surgery for heart failure, recurrent emboli, or resistant organisms
- Valve repair preferred over replacement when feasible
- Avoid surgery if possible in active IDU patients
Post-Stroke
- Surgery may proceed without delay if intracranial hemorrhage excluded and neurologic damage not severe
- Delay at least 4 weeks if major ischemic stroke or intracranial hemorrhage
Fuster & Hurst's The Heart, 15th Edition, Table 23-16; AHA 2015 Scientific Statement
Prophylaxis (AHA 2021 Update)
Antibiotic prophylaxis is recommended before invasive dental procedures for high-risk patients:
High-risk cardiac conditions:
- Prosthetic cardiac valves (including transcatheter-implanted)
- History of IE
- Congenital heart disease (unrepaired cyanotic CHD; repaired CHD with residual defects near prosthetic material; within 6 months of repair)
- Cardiac transplant recipients with valvulopathy
- Ventricular assist devices and implantable hearts (added in 2021)
Prophylaxis regimen:
- Amoxicillin 2g PO 30-60 min before procedure (preferred)
- Clindamycin removed from 2021 guidelines due to C. difficile risk
- Doxycycline added as alternative in true penicillin-allergic patients
- Allergy screening: 90% of patients with reported penicillin allergy have negative skin testing - so amoxicillin can often be used
Braunwald's Heart Disease, 2021 AHA update; p. 1227-1232
Prognosis
- Untreated IE is uniformly fatal
- With appropriate antibiotics ± surgery, in-hospital mortality remains 15-30%
- Adverse prognostic factors: S. aureus, heart failure, large vegetations, perivalvular extension, embolic stroke, renal failure, prosthetic valve involvement
- Multidisciplinary "endocarditis team" approach (infectious disease + cardiology + cardiac surgery) has been shown to improve outcomes
Braunwald's Heart Disease, p. 3524; Goldman-Cecil Medicine
Key Sources: Braunwald's Heart Disease (11th Ed.) | Robbins & Kumar Basic Pathology | Washington Manual of Medical Therapeutics | Fuster & Hurst's The Heart (15th Ed.) | Textbook of Clinical Echocardiography (2023 Duke Criteria) | AHA Scientific Statements (2015, 2021)
This is a shared conversation. Sign in to Orris to start your own chat.