Send me detailed questions for FON 1 and 2 important questions for Gujrat University Main Exam please
Asking for Preferences
Reading File
Searching the Web
Foundations of Nursing FON 1 2 Gujarat University important exam questions syllabus
Reading Web Page
https://www.studocu.com/in/document/gujarat-university/basic…
Finding Sources
Finding Sources
Searching the Web
BSc Nursing FON 1 FON 2 Gujarat University syllabus topics foundations of nursing 1st 2nd year
Reading Web Page
https://www.spuvvn.edu/orbit-cdn/uploads/Syllabi_data/bsc_nu…
I now have enough information about the Gujarat University / INC syllabus for FON 1 & 2. Here is a complete and detailed question bank covering all types:
📚 FON 1 & FON 2 - Important Questions for Gujarat University Main Exam
B.Sc. Nursing - Foundations of Nursing (INC / Gujarat University Syllabus)
🔵 FOUNDATIONS OF NURSING - 1 (FON 1)
✅ LONG ANSWER QUESTIONS (10 Marks each)
-
Define health. Explain WHO definition of health. Discuss the concepts of health, illness, and wellness with their interrelationship.
-
Define nursing. Trace the historical development of nursing profession in India and internationally. What are Florence Nightingale's contributions to modern nursing?
-
Explain the functions, roles, and responsibilities of a professional nurse. What qualities should a nurse possess?
-
Define hospital. Classify hospitals. Explain the organizational structure of a hospital and the role of a nurse within it.
-
Explain the nursing process in detail. Describe each step: Assessment, Diagnosis, Planning, Implementation, and Evaluation (ADPIE) with examples.
-
Define communication. Explain the types and process of communication. Discuss therapeutic communication techniques with examples.
-
Explain medical and surgical asepsis. Describe the chain of infection and the nursing measures to break each link.
-
Define vital signs. Explain the procedure of recording temperature, pulse, respiration, and blood pressure with normal values and deviations.
-
Explain the principles and procedure of hand hygiene. Describe the types of isolation precautions used in hospital settings.
-
Define ethics. Discuss the ethical principles in nursing practice. Explain the nurses' code of ethics and professional conduct.
✅ SHORT ANSWER QUESTIONS (5 Marks each)
- Define health. Write the WHO definition of health.
- Differentiate between health and wellness.
- What is the nursing process? Name its five steps.
- Define nursing diagnosis. Give two examples.
- What is therapeutic communication? Give five techniques.
- Define medical asepsis. List five principles.
- Explain Standard Precautions (Universal Precautions).
- What is the chain of infection? List its six links.
- Define vital signs. What are the normal values of all four vital signs in adults?
- Explain types of thermometers and procedure to record temperature.
- What is pulse? Write the sites, normal rate, and characteristics of pulse.
- What is documentation? Write the principles of documentation and reporting.
- Define ethics and list the ethical principles in nursing.
- Explain admission, discharge, and transfer procedure of a patient.
- Write a short note on primary health care and its principles.
- What is the nurse-patient relationship? Describe its phases.
- Define hospital infection (nosocomial infection). List preventive measures.
- What are the qualities of a good nurse?
- Explain the roles of ICN (International Council of Nurses).
- Write a short note on Indian Nursing Council (INC).
✅ MCQs (FON 1)
-
WHO defines health as a state of complete ___ well-being.
- a) Physical
- b) Mental
- c) Social
- d) Physical, mental and social ✓
-
The nursing process was introduced by:
- a) Florence Nightingale
- b) Ida Jean Orlando ✓
- c) Virginia Henderson
- d) Dorothea Orem
-
The first step of the nursing process is:
- a) Assessment ✓
- b) Planning
- c) Diagnosis
- d) Evaluation
-
Normal body temperature (oral) is:
- a) 36°C
- b) 37°C (98.6°F) ✓
- c) 38°C
- d) 36.5°C
-
Normal adult pulse rate is:
- a) 40-60 beats/min
- b) 60-100 beats/min ✓
- c) 100-120 beats/min
- d) 50-80 beats/min
-
Normal respiratory rate in adults is:
- a) 10-14 breaths/min
- b) 12-20 breaths/min ✓
- c) 20-30 breaths/min
- d) 8-12 breaths/min
-
The color of the apron used for isolation in contact precautions is:
- a) Blue
- b) Yellow ✓
- c) Green
- d) Red
-
Nosocomial infection refers to:
- a) Community-acquired infection
- b) Hospital-acquired infection ✓
- c) Congenital infection
- d) Opportunistic infection
-
Florence Nightingale is known as:
- a) Mother of Medicine
- b) Lady with the Lamp ✓
- c) Angel of Mercy
- d) Pioneer of Surgery
-
The principle of "do no harm" in nursing ethics is called:
- a) Beneficence
- b) Non-maleficence ✓
- c) Autonomy
- d) Justice
-
Standard precautions apply to:
- a) Only blood
- b) Only body fluids
- c) All body fluids, blood, secretions, and excretions ✓
- d) Only patients with HIV
-
The site most commonly used for taking temperature in unconscious patients is:
- a) Oral
- b) Axillary
- c) Rectal ✓
- d) Tympanic
🟢 FOUNDATIONS OF NURSING - 2 (FON 2)
✅ LONG ANSWER QUESTIONS (10 Marks each)
-
Explain bed making. Describe the procedure of making an occupied bed. What are the principles and purposes of bed making?
-
Define physical examination. Explain the four methods of physical examination (Inspection, Palpation, Percussion, Auscultation). Describe the preparation of a patient for physical examination.
-
Explain health assessment. Describe the techniques of head-to-toe assessment in a nursing patient.
-
Explain the principles and procedure of administration of medications by oral, subcutaneous, intramuscular, and intravenous routes. List the 10 rights of medication administration.
-
Define personal hygiene. Describe the procedure of bed bath (sponge bath). What are the purposes and principles of personal hygiene?
-
Define oxygenation. Explain the types of oxygen therapy, methods of oxygen administration, and nursing responsibilities during oxygen therapy.
-
Define nutrition. Explain the classification of nutrients with their functions and food sources. Describe nasogastric tube feeding procedure.
-
Explain fluid and electrolyte balance. Describe the signs of fluid imbalance. Discuss nursing management of a patient on intravenous therapy.
-
Describe the nursing care of a patient with pressure ulcer (bedsores). Include etiology, stages, prevention, and treatment.
-
Define pain. Explain the types of pain, pain assessment tools (VAS, numeric scale), and pharmacological and non-pharmacological nursing management of pain.
✅ SHORT ANSWER QUESTIONS (5 Marks each)
- Write the 10 rights of medication administration.
- Define body mechanics. Write the principles of good body mechanics.
- What is patient positioning? Describe Fowler's, Sims', and Trendelenburg positions with their purposes.
- Write a short note on pressure ulcer (bedsores) - stages and prevention.
- Explain the procedure for insertion and care of a urinary catheter.
- Describe the procedure for administration of enema. List its purposes and contraindications.
- What is intake and output chart? Why is it important? How is it maintained?
- Describe the procedure of nasogastric tube insertion and feeding.
- Write a short note on oxygen therapy - types, indications, and nursing care.
- What is specimen collection? Describe collection of urine for routine examination and culture.
- Explain the procedure of sponge bath (bed bath) and its purposes.
- Write a short note on chest physiotherapy - techniques and purposes.
- Describe the procedure of blood glucose monitoring (GRBS).
- What are the signs and symptoms of fluid and electrolyte imbalance?
- Define elimination. Describe nursing care for a patient with urinary incontinence.
- Write the procedure for care of unconscious patient.
- Explain the principles and procedure of steam inhalation.
- Describe care of a terminally ill and dying patient. Include psychological support.
- Write a short note on wound care and dressing procedure.
- What is oral hygiene? Write the procedure of oral care in a conscious and unconscious patient.
✅ MCQs (FON 2)
-
The 10 rights of medication administration include all EXCEPT:
- a) Right drug
- b) Right dose
- c) Right diagnosis ✓
- d) Right patient
-
The Fowler's position has the head of the bed elevated at:
- a) 15-30°
- b) 45-60° ✓
- c) 90°
- d) 30°
-
The angle used for intramuscular injection is:
- a) 15°
- b) 45°
- c) 90° ✓
- d) 30°
-
The preferred site for IM injection in adults is:
- a) Deltoid
- b) Vastus lateralis / Ventrogluteal ✓
- c) Dorsogluteal
- d) Rectus femoris
-
Braden scale is used to assess risk of:
- a) Fall
- b) Pain
- c) Pressure ulcer ✓
- d) Malnutrition
-
Normal urine output per hour in adults is:
- a) 10-20 mL/hr
- b) 30-60 mL/hr ✓
- c) 80-100 mL/hr
- d) 5-10 mL/hr
-
The angle for subcutaneous injection is:
- a) 90°
- b) 45° ✓
- c) 15°
- d) 30°
-
The oxygen flow rate for nasal prongs (low-flow) is:
- a) 1-6 L/min ✓
- b) 6-10 L/min
- c) 10-15 L/min
- d) 0.5-1 L/min
-
Trendelenburg position is used in:
- a) Respiratory distress
- b) Hypovolemic shock ✓
- c) Head injury
- d) Cardiac failure
-
The Numeric Rating Scale (NRS) for pain ranges from:
- a) 0-5
- b) 0-10 ✓
- c) 1-10
- d) 0-100
-
A Foley catheter is a type of:
- a) Nasogastric tube
- b) Urinary catheter ✓
- c) IV catheter
- d) Chest tube
-
The normal blood glucose (GRBS) in a fasting adult is:
- a) 50-70 mg/dL
- b) 70-100 mg/dL ✓
- c) 100-140 mg/dL
- d) 110-140 mg/dL
-
Pressure ulcer Stage II is characterized by:
- a) Intact skin with non-blanchable redness
- b) Partial thickness skin loss involving epidermis and dermis ✓
- c) Full thickness tissue loss
- d) Exposed bone/tendon
-
Nasogastric tube is measured from:
- a) Tip of nose - earlobe - xiphisternum ✓
- b) Nose to umbilicus
- c) Ear to stomach
- d) Mouth to xiphoid
-
Semi-Fowler's position is at:
- a) 15°
- b) 30-45° ✓
- c) 60°
- d) 90°
📌 MOST EXPECTED TOPICS (High Frequency in Gujarat University Exams)
| Topic | Expected Question Type |
|---|---|
| Nursing Process (ADPIE) | Long + Short |
| Vital Signs | Long + Short + MCQ |
| Infection Control / Asepsis | Long + Short |
| Medication Administration (10 Rights) | Long + Short + MCQ |
| Oxygen Therapy | Short + MCQ |
| Pressure Ulcer | Short + MCQ |
| Physical Examination Methods | Long + Short |
| Bed Making / Personal Hygiene | Short |
| Fluid & Electrolyte Balance | Short + MCQ |
| Nasogastric Tube Feeding | Short |
| Nursing Ethics | Short + Long |
| History of Nursing / Florence Nightingale | Long |
| Patient Positioning | Short + MCQ |
| Communication / Therapeutic Communication | Short + Long |
Exam tip: Gujarat University consistently asks about Vital Signs, Nursing Process, Medication Administration, Infection Control, and Personal Hygiene as long questions every year. Make sure you know procedures step-by-step, including the purpose, principles, equipment, and after-care for each skill. For MCQs, focus on normal values, angles of injection, oxygen flow rates, and positioning degrees.
Pathophysiology of TB in detail please
Reading File
Finding Sources
Finding Sources
Searching the Web
pathophysiology of tuberculosis TB detailed mechanism granuloma formation
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all I need for a comprehensive answer. Here is the detailed pathophysiology of TB:
Pathophysiology of Tuberculosis (TB) - Detailed
1. The Causative Organism
Mycobacterium tuberculosis (MTB) is a Gram-positive, obligate aerobe and obligate intracellular parasite. Its defining feature is acid-fastness - the ability to resist decolorization by an alcohol/acid mixture after staining (Ziehl-Neelsen stain). This property comes from its thick, waxy cell wall rich in mycolic acids. It has a very slow replication time (~15-20 hours), which has major implications for disease progression and treatment duration.
2. Transmission
MTB is transmitted person-to-person via aerosolized droplet nuclei (1-5 μm in diameter). These particles are small enough to bypass mucociliary clearance and reach the distal alveoli directly. Key points:
- Infectiousness depends on the severity of cough (promoted by sulfolipid in the mycobacterial cell envelope) and bacterial burden.
- Patients with cavitary lesions harbor 10⁷-10⁹ bacilli and are the most infectious.
- An infectious individual infects on average 3-10 people per year.
- In household contacts with intense and prolonged exposure, 25-50% become infected.
- HIV-positive patients are less likely to be smear-positive or develop cavitary disease, making them less infectious but more vulnerable.
3. The Pathogenesis: A Step-by-Step Sequence
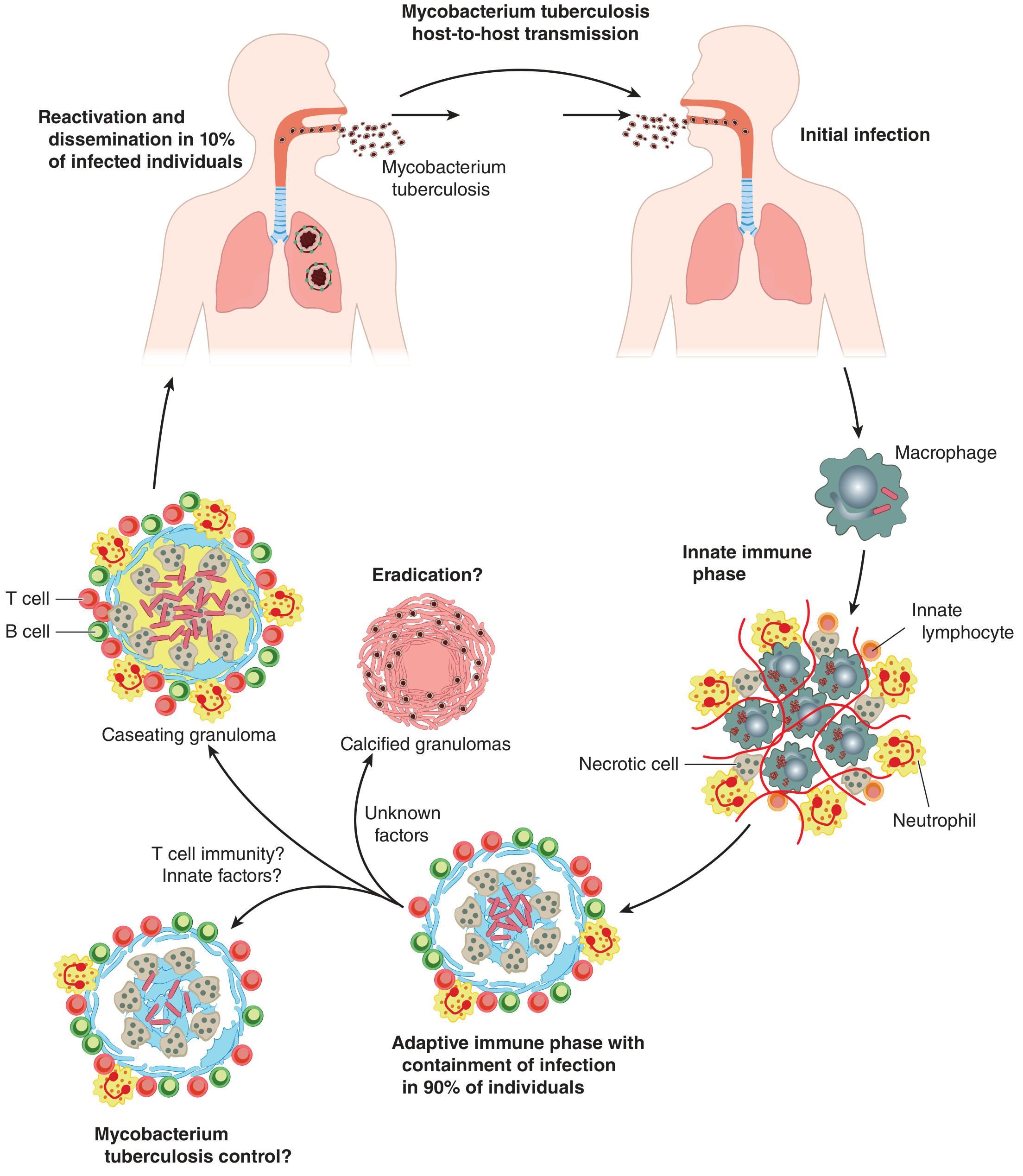
Figure: Complete cycle of MTB pathogenesis - from initial infection through innate immune phase, adaptive immune containment, granuloma formation, latency, and reactivation. (Goldman-Cecil Medicine, 22e)
Stage 1 - Initial Encounter: Alveolar Macrophage Infection (Days 1-7)
When MTB bacilli reach the distal alveoli, they are phagocytosed by alveolar macrophages. Normally, macrophages destroy pathogens through phagolysosome fusion. However, MTB has evolved multiple immune evasion strategies:
- Phagosome maturation arrest - MTB prevents the phagosome from fusing with lysosomes by secreting factors that inhibit Rab7 and other fusion proteins.
- Inhibition of acidification - The phagosome cannot acidify to a bactericidal pH.
- Resistance to reactive oxygen species - MTB's thick cell wall and catalase-peroxidase enzymes neutralize oxidative bursts.
- Surviving inside macrophages, MTB uses the lipid-rich intracellular environment as a nutrient source.
The alveolar macrophages are poorly equipped to handle MTB and fail to control bacterial replication at this stage.
Stage 2 - Innate Immune Phase: Bacterial Proliferation (Days 7-21)
During this phase, the patient typically remains asymptomatic while bacteria multiply rapidly inside macrophages. The innate immune system responds by recruiting additional cells:
- Monocyte-derived macrophages
- Interstitial macrophages
- Neutrophils
- Innate lymphocytes
These cells also fail to control MTB replication. Infected and necrotic cells accumulate at the site.
Meanwhile, infected dendritic cells carry MTB antigens via lymphatics to the draining hilar/mediastinal lymph nodes, where they present antigens to naive T cells. This triggers the adaptive immune response - but this takes time.
Stage 3 - Adaptive Immune Response and Granuloma Formation (2-8 Weeks)
The interval from initial infection to a positive tuberculin skin test (TST) or IGRA (interferon-gamma release assay) is usually 2-8 weeks. This delay allows MTB to establish infection.
Once activated, antigen-specific T cells (primarily CD4+ Th1 cells) return to the infected lung and orchestrate the adaptive response:
- CD4+ T cells secrete IFN-γ, which activates macrophages to upregulate bactericidal activity (nitric oxide production, autophagy).
- Activated macrophages, T cells, B cells, and neutrophils aggregate around infected macrophages to form the granuloma - the hallmark histopathological lesion of TB.
- TNF-α (from macrophages) is essential for granuloma formation and maintenance.
In 90% of immunocompetent individuals, the adaptive immune response successfully contains the infection within granulomas, leading to latent TB.
4. The Granuloma - Structure and Function
The tuberculous granuloma is the central pathological feature of TB. It is an organized immune structure with the following cellular composition (from inside out):
| Zone | Cell Type | Function |
|---|---|---|
| Central core | Caseous necrotic debris | Bactericidal low-O₂ environment |
| Inner layer | Epithelioid macrophages | Antigen presentation, contain bacilli |
| Giant cells | Langhans' giant cells (fused macrophages with peripheral nuclei) | Engulf large bacilli clusters |
| Middle layer | Activated/foamy macrophages | Lipid-laden; may harbor dormant bacilli |
| Outer rim | CD4+ and CD8+ T lymphocytes, B cells | Immune surveillance |
| Periphery | Fibroblasts + fibrous capsule | Wall off the lesion |
Why Caseation Occurs
- The low oxygen tension inside the granuloma inhibits macrophage function and bacillary growth.
- Macrophage death leads to central caseation - the "cheese-like" necrosis that gives TB its characteristic gross appearance.
- This process is a Type IV (delayed-type) hypersensitivity reaction, mediated by sensitized T lymphocytes.
The Granuloma as a Double-Edged Sword
While granulomas contain infection, they also:
- Provide a protected niche where MTB can persist in a dormant state.
- Create an immunosuppressive microenvironment around the bacilli.
- Keep CD4+ T cells peripherally located, away from centrally infected macrophages, reducing their effectiveness.
- Facilitate bacterial spread between aggregated macrophages if they rupture.
5. Outcomes After Primary Infection
MTB exposure
|
▼
Alveolar Macrophage Infection
|
├──► ~10% → Immune resistance (innate) → No infection established
|
▼
Innate immune response fails
|
▼
Adaptive immune response (2-8 weeks)
|
├──► ~90% → LATENT TB (Granuloma containment)
| → Calcified Ghon complex
| → 10% lifetime risk of reactivation
|
└──► ~10% → ACTIVE TB (Progressive primary or reactivation)
→ Pulmonary (80%)
→ Extrapulmonary (20%)
6. Ghon Complex - Primary Infection Lesion
The Ghon focus is a small (1-2 cm) area of patchy opacity in the peripheral mid-lung zone (typically lower lobes) where initial infection occurs. It consists of:
- A subpleural parenchymal granuloma (the Ghon lesion)
- Lymphangitis connecting it to the hilum
- Hilar/mediastinal lymphadenopathy
Together, the Ghon focus + hilar adenopathy = the Ghon complex (also called Ranke complex when calcified). Over time, these calcify and may remain visible on chest X-ray as evidence of prior TB.
7. Latent TB Infection (LTBI)
In LTBI, MTB bacilli survive in a dormant, non-replicating state within granulomas, especially in the lung apices (due to high O₂ tension favoring dormant bacilli). The host's immune system maintains dynamic containment:
- The bacteria are metabolically inactive but viable.
- Patients are asymptomatic and non-infectious.
- Diagnosis is made via TST (Mantoux) or IGRA (detecting IFN-γ response).
- A positive TST/IGRA with no clinical disease = LTBI.
8. Reactivation TB (Post-Primary/Secondary TB)
Approximately 10% of LTBI patients will develop active disease during their lifetime. Risk factors include:
| Risk Factor | Mechanism |
|---|---|
| HIV infection | CD4+ T cell depletion → granuloma breakdown |
| TNF-α inhibitors (biologics) | Prevent granuloma formation |
| Diabetes mellitus | Impaired macrophage and T cell function |
| Malnutrition / low BMI | Impaired cell-mediated immunity |
| Silicosis | Macrophage destruction by silica particles |
| End-stage renal disease | Uremia suppresses immunity |
| Corticosteroids / immunosuppressants | General immune suppression |
| Old age / extremes of age | Waning cell-mediated immunity |
Mechanism of Reactivation:
- The balance between host immunity and bacterial dormancy is disrupted.
- Hydrolytic enzymes liquefy the caseous center of the granuloma.
- The caseous material, which is highly bactericidal when solid (due to low O₂, low pH, fatty acids), becomes a liquid culture medium when liquefied.
- Liquefied caseum allows explosive bacterial multiplication (up to 10⁹ bacilli).
- The softened granuloma wall erodes into a bronchus, spilling caseous material and bacteria.
- This creates a tuberculous cavity - the hallmark of reactivation TB.
Typical Location of Reactivation TB:
- Apical and posterior segments of the upper lobes (highest O₂ tension = best growth environment for obligate aerobe MTB)
- Superior segments of the lower lobes
- This is in contrast to primary TB, which typically occurs in the mid-lung zones.
9. Cavitary Disease and Tissue Destruction
Once a cavity forms:
- It contains 10⁷-10⁹ bacilli and is highly infectious.
- The cavity may expand due to continued immune-mediated destruction and bacterial growth.
- Secondary infections with bacteria, fungi (Aspergillus forming aspergilloma), or yeasts enhance further tissue destruction.
- Erosion into blood vessels causes hemoptysis (can be life-threatening).
- Bronchial wall involvement leads to bronchiectasis.
10. Extrapulmonary Dissemination
MTB disseminates via hematogenous or lymphatic spread from pulmonary lesions. Virtually any organ can be seeded. Common extrapulmonary sites:
| Site | Disease |
|---|---|
| Lymph nodes | Scrofula (cervical TB adenitis) - most common extrapulmonary form |
| Pleura | Tuberculous pleuritis/effusion |
| Meninges | TB meningitis (most dangerous) |
| Spine | Pott's disease (vertebral TB) |
| Kidney | Renal TB (sterile pyuria, "rice-water" urine) |
| Adrenals | Addison's disease (bilateral adrenal destruction) |
| Pericardium | Constrictive pericarditis |
| Bone/Joints | Osteoarticular TB |
| Peritoneum | Tuberculous peritonitis |
| Liver/Spleen | Hepatosplenomegaly |
Miliary TB
When MTB spreads massively through the bloodstream (typically with profound immunosuppression), it seeds multiple organs simultaneously. The chest X-ray shows a pattern of diffuse tiny 1-3 mm nodules resembling millet seeds (hence the term "miliary"). It is the most severe form and can be fatal if untreated.
11. Immunopathology Summary
MTB survives in macrophages
↓
Dendritic cells → Lymph node → CD4+ T cell activation
↓
IFN-γ secretion → Macrophage activation
↓
TNF-α production → Granuloma formation (Type IV HSR)
↓
Granuloma = Epithelioid macrophages + Langhans giant cells
+ Lymphocytes + Fibrous capsule
↓
Central caseation (low O₂ → macrophage death)
↓
├─► Calcification → Latent TB (LTBI)
└─► Liquefaction → Cavity → Active TB
12. Why MTB is So Successful as a Pathogen
- Phagosome maturation arrest - survives inside macrophages
- Slow growth rate - evades rapid immune detection
- Thick waxy cell wall - resists killing by oxidative burst
- Dormancy - can persist for decades in granulomas
- Exploits CD4+ T cell destruction - HIV co-infection triggers rapid reactivation
- Aerosol transmission - highly efficient spread in crowded settings
Sources: Goldman-Cecil Medicine, 22e; Schwartz's Principles of Surgery, 11e; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.