Classification of antihypertensives
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have thorough content from multiple authoritative textbooks. Let me compile the comprehensive answer.
Classification of Antihypertensive Drugs
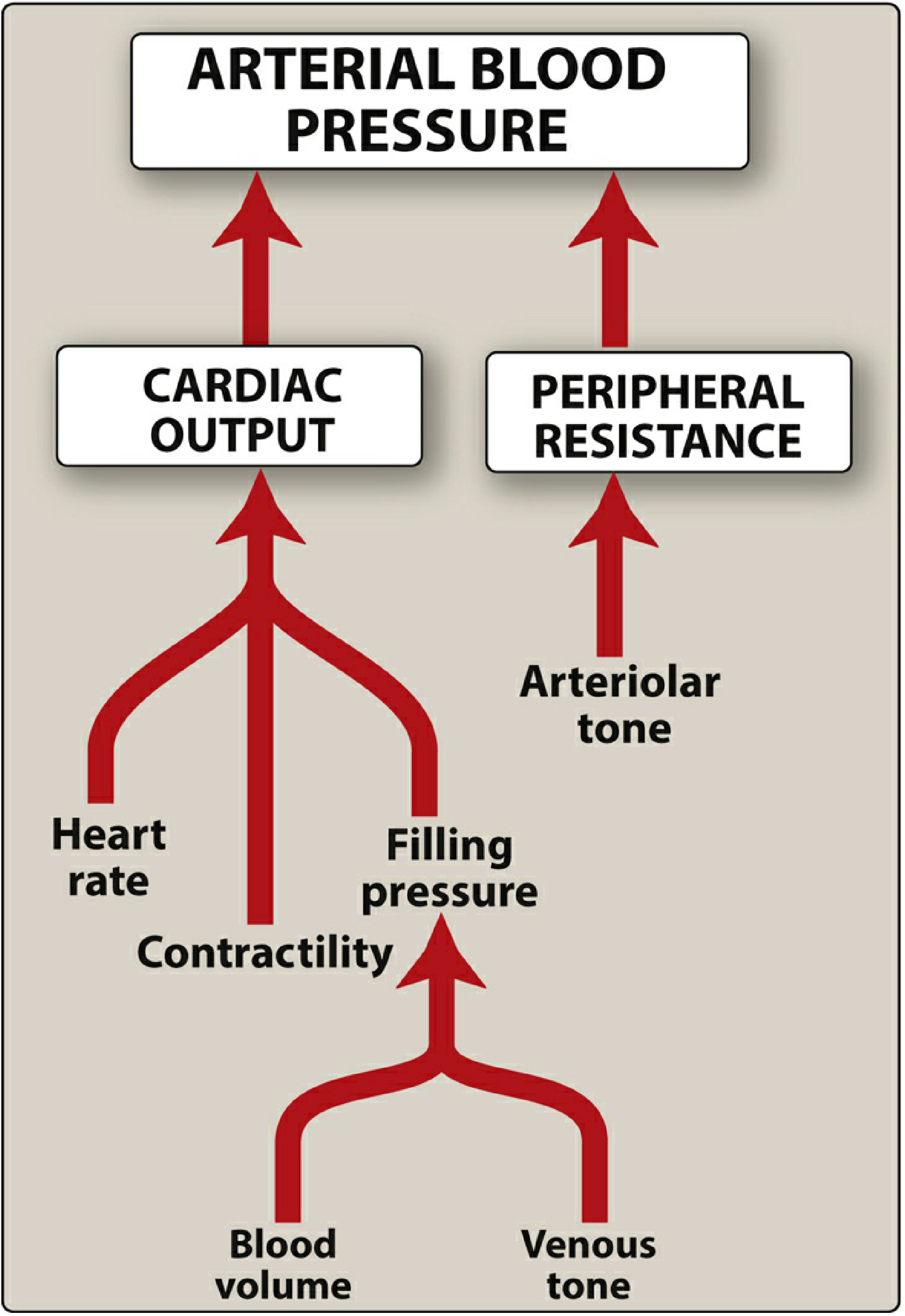
Arterial blood pressure = Cardiac Output x Peripheral Vascular Resistance. All antihypertensive drugs act by reducing one or both of these determinants, either by reducing blood volume, reducing sympathetic drive, blocking the renin-angiotensin system, or directly dilating blood vessels.
Katzung's Mechanistic Classification (4 Major Groups)
As described in [Katzung's Basic and Clinical Pharmacology, 16th Ed], antihypertensives are classified by their principal site or mechanism of action:
- Diuretics - reduce blood volume by depleting sodium
- Renin-Angiotensin system blockers - reduce peripheral vascular resistance and blood volume
- Direct vasodilators - relax vascular smooth muscle to dilate resistance vessels
- Sympathoplegic agents - reduce peripheral resistance, inhibit cardiac function, increase venous pooling
Full Detailed Classification
1. DIURETICS
Act on the kidney to promote sodium and water excretion, reducing blood volume and cardiac output.
| Subclass | Examples | Site of Action |
|---|---|---|
| Thiazides | Hydrochlorothiazide, Chlorthalidone, Indapamide, Metolazone | Distal convoluted tubule |
| Loop diuretics | Furosemide, Bumetanide, Torsemide, Ethacrynic acid | Thick ascending loop of Henle |
| Potassium-sparing | Triamterene, Amiloride | Collecting duct (ENaC block) |
| Mineralocorticoid receptor antagonists (MRAs) | Spironolactone, Eplerenone | Collecting duct (aldosterone block) |
Thiazides and chlorthalidone are first-line choices. In resistant hypertension, MRAs (especially spironolactone) are effective add-ons - Lippincott Illustrated Reviews Pharmacology.
2. RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM (RAAS) BLOCKERS
A. ACE Inhibitors
Block conversion of Ang I to Ang II by ACE. Also inhibit breakdown of bradykinin (causing the characteristic dry cough).
Sub-classified by chemical structure (Brenner & Rector's The Kidney):
- Sulfhydryl group: Captopril
- Carboxyl group: Enalapril, Lisinopril, Ramipril, Perindopril, Fosinopril, Benazepril, Quinapril, Trandolapril
- Phosphinyl group: Fosinopril
Mechanisms beyond ACE blockade: inhibit bradykinin breakdown, enhance NO-mediated vasodilation, reduce aldosterone, reduce sympathetic tone, reverse vascular hypertrophy.
Key ADEs: Dry cough (bradykinin), angioedema, hyperkalemia, teratogenic (contraindicated in pregnancy).
B. Angiotensin II Receptor Blockers (ARBs)
Block AT1 receptors directly. No bradykinin effect, so NO cough. Same end-organ benefits as ACEi.
Examples: Losartan, Valsartan, Candesartan, Irbesartan, Olmesartan, Telmisartan, Azilsartan
C. Direct Renin Inhibitor
- Aliskiren - inhibits renin directly, acts earliest in the RAAS cascade. Not combined with ACEi/ARB. Causes diarrhea; rare angioedema. Contraindicated in pregnancy.
Do NOT combine ACEi + ARB + renin inhibitor (dual RAAS blockade increases adverse outcomes).
3. CALCIUM CHANNEL BLOCKERS (CCBs)
Block L-type voltage-gated Ca²+ channels. Three chemical subclasses with distinct profiles (Lippincott Illustrated Reviews Pharmacology):
| Subclass | Drug(s) | Vascular Effect | Cardiac Effect | Key Use |
|---|---|---|---|---|
| Diphenylalkylamines | Verapamil | Moderate | Strong (neg. chrono/ino/dromotropy) | HTN, SVT, angina |
| Benzothiazepines | Diltiazem | Moderate | Moderate (less inotropic than verapamil) | HTN, SVT, angina |
| Dihydropyridines | Nifedipine, Amlodipine, Felodipine, Nicardipine, Isradipine, Nisoldipine | Strong | Minimal (mainly vascular) | HTN, angina |
Dihydropyridines are the preferred CCBs for hypertension. Verapamil and diltiazem are preferred when rate control is also needed. First-line in Black patients and elderly.
4. SYMPATHOPLEGIC AGENTS (Adrenergic Inhibitors)
Sub-divided by site of action along the sympathetic arc:
A. Centrally Acting Alpha-2 Agonists
Stimulate presynaptic α2 receptors in the CNS (nucleus tractus solitarius/vasomotor center) → reduce sympathetic outflow.
- Clonidine - also used for opioid withdrawal, ADHD
- Methyldopa - drug of choice in pregnancy (safest antihypertensive in pregnancy)
- Guanabenz, Guanfacine
ADEs: Sedation, dry mouth, rebound hypertension on abrupt withdrawal (clonidine).
B. Peripherally Acting Adrenergic Neuron Blockers
- Reserpine - depletes NE stores from vesicles; rarely used (depression, nasal stuffiness)
- Guanethidine, Guanadrel - block NE release from nerve terminals; largely obsolete
C. Beta-Blockers (β-Adrenoceptor Antagonists)
Reduce cardiac output (negative chrono + inotropic effects) and inhibit renin release.
Sub-classified by selectivity:
| Subtype | Examples | Selectivity |
|---|---|---|
| Cardioselective (β1) | Atenolol, Metoprolol, Bisoprolol, Betaxolol, Acebutolol | β1 selective |
| Non-selective (β1+β2) | Propranolol, Nadolol, Timolol, Pindolol (ISA) | β1 + β2 |
| Alpha + Beta blockers | Carvedilol, Labetalol | α1 + β1 + β2 |
| β1 + vasodilating | Nebivolol | β1 selective + NO release |
ADEs: Bradycardia, bronchospasm (non-selective), mask hypoglycemia, cold extremities, sexual dysfunction, dyslipidemia. Avoid abrupt withdrawal (rebound hypertension/angina). Contraindicated in decompensated asthma/COPD.
D. Alpha-1 Blockers (Peripheral)
Block postsynaptic α1 receptors → vasodilation of arterioles and veins.
- Prazosin, Doxazosin, Terazosin
- ADEs: First-dose orthostatic hypotension (take first dose at bedtime), reflex tachycardia, fluid retention
- Useful co-indication: Benign prostatic hyperplasia (BPH)
5. DIRECT VASODILATORS
Act directly on vascular smooth muscle to cause vasodilation; cause reflex tachycardia and fluid retention (must combine with β-blocker + diuretic).
| Drug | Mechanism | Route | Notes |
|---|---|---|---|
| Hydralazine | Arteriolar dilation (mechanism not fully known) | Oral/IV | Lupus-like syndrome at high doses (>400 mg/d), drug of choice in pregnancy-induced HTN (IV) |
| Minoxidil | Opens K+ channels → hyperpolarization → arteriolar dilation | Oral | Reserved for refractory HTN; causes hypertrichosis |
| Sodium nitroprusside | Releases NO → dilates arteries AND veins | IV only | Hypertensive emergencies; cyanide toxicity risk |
| Diazoxide | Opens K+ channels (like minoxidil) | IV | Hypertensive emergencies |
| Fenoldopam | Dopamine D1 receptor agonist → renal + peripheral vasodilation | IV | Hypertensive emergencies; preserves renal perfusion |
6. ADDITIONAL/MISCELLANEOUS
Aldosterone Antagonists / Mineralocorticoid Receptor Antagonists
(Also listed under diuretics)
- Spironolactone, Eplerenone - especially useful in resistant hypertension, primary hyperaldosteronism, heart failure with HTN
Nitrates (mainly for angina/HF, not primary antihypertensives)
- Nitroglycerin, Isosorbide dinitrate/mononitrate - primarily venodilators
Summary Table by First-Line Status
| Class | First-Line? | Compelling Indications |
|---|---|---|
| Thiazide diuretics | YES | Heart failure, isolated systolic HTN, elderly, Black patients |
| ACE inhibitors | YES | Diabetes + CKD, post-MI, heart failure, LV dysfunction |
| ARBs | YES | ACEi-intolerant, diabetes + CKD, heart failure |
| Dihydropyridine CCBs | YES | Elderly, Black patients, angina, isolated systolic HTN |
| Beta-blockers | Second-line | Post-MI, heart failure with reduced EF, angina, tachyarrhythmias |
| Alpha-1 blockers | Not first-line | BPH + HTN |
| Central alpha-2 agonists | Not first-line | Pregnancy (methyldopa) |
| Direct vasodilators | Resistant/emergency HTN | Hypertensive emergencies, refractory HTN |
| Renin inhibitors | Not first-line | Alternative RAAS blockade |
| MRAs | Add-on for resistant HTN | Primary hyperaldosteronism, heart failure |
Preferred Agents by Compelling Indication
| Condition | Preferred Drug(s) |
|---|---|
| Pregnancy | Methyldopa, Hydralazine (IV), Labetalol, Nifedipine |
| Diabetes + CKD | ACEi or ARB |
| Heart failure (HFrEF) | ACEi/ARB + beta-blocker + MRA + loop diuretic |
| Post-MI | Beta-blocker + ACEi |
| Atrial fibrillation | Beta-blocker or Verapamil/Diltiazem |
| BPH + HTN | Alpha-1 blocker (doxazosin) |
| Black patients | Thiazide or CCB (ACEi/ARB less effective as monotherapy) |
| Hypertensive emergency | IV nitroprusside, IV nicardipine, IV labetalol, IV fenoldopam |
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed; Lippincott Illustrated Reviews: Pharmacology; Brenner & Rector's The Kidney, 2-Vol Set; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.