
20260620_134716.jpg
Analysis report
Reading File
Finding Sources
Finding Sources
Searching PubMed
"early repolarization" ECG pattern clinical significance
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough analysis of this ECG report.
ECG Analysis Report - Goutam Giri
Patient Demographics
| Field | Value |
|---|---|
| Name | Goutam Giri |
| ID | 200549 |
| Age / Sex | 36 years, Male, 78 kg |
| Date / Time | 20/06/2026, 12:56:50 |
| Facility | Nidan, Vipul Plaza, Bhubaneswar |
Recorded Parameters
| Parameter | Value | Normal Range |
|---|---|---|
| Heart Rate | 62 bpm | 60-100 bpm |
| PR Interval | 152 ms | 120-200 ms |
| QRS Duration | 90 ms | 70-110 ms |
| QT Interval | 328 ms | 350-450 ms (varies by HR) |
| QTc | 332 ms | <440 ms (male) |
| P Axis | 01° | Normal |
| QRS Axis | 05° | Normal (-30° to +90°) |
| T Axis | 18° | Normal |
Machine Interpretation (as printed)
The ECG machine flagged three findings:
- Sinus Rhythm - normal baseline rhythm
- Lateral ST Elevation - Possible Early Repolarization
- Inferior T Wave Abnormality is Nonspecific
Detailed Interpretation
Rhythm
- Sinus rhythm at 62 bpm - normal rate, no arrhythmia detected.
ST Elevation - Lateral Leads (I, aVL, V4-V6)
The machine flags lateral ST elevation and correctly identifies it as possible early repolarization (ER). In a 36-year-old male, this is the most common benign explanation. The classic features of benign early repolarization (BER) are:
- ST segment elevation with upward concavity (saddle-shaped, not domed)
- J-point notching at the QRS-ST junction
- Large, concordant (upright) T waves in the same leads
- ST elevation typically <2 mm in precordial leads, <0.5 mm in limb leads
- Temporal stability - does not evolve or change acutely
BER is present in up to 10-19% of young males and has historically been considered a normal variant. Per Rosen's Emergency Medicine, "BER is a normal electrocardiographic variant that does not imply or exclude ACS or CAD."
Inferior T-Wave Abnormality (Nonspecific)
The machine notes a nonspecific T-wave abnormality in the inferior leads (II, III, aVF). The term "nonspecific" is important - it means the finding does not clearly fit any single diagnosis. Causes include:
- Normal variant / positional change
- Early repolarization extending to inferior leads
- Mild ischemia (less likely without symptoms)
- Vagotonia (common in young athletic males)
- Electrolyte imbalance (hypokalemia, hypomagnesemia)
QTc of 332 ms
The corrected QT is mildly short (normal lower limit ~350 ms). Short QTc can be a normal variant in young males, especially with slower heart rates, but very short QTc (<320 ms) raises concern for Short QT Syndrome. At 332 ms, this is borderline and worth noting.
Clinical Significance & Risk Stratification
This ECG pattern in a 36-year-old asymptomatic male is most consistent with benign early repolarization. However, context matters greatly:
| Clinical Scenario | Significance |
|---|---|
| Asymptomatic, routine check | Very likely benign; no treatment needed |
| Chest pain / syncope | Urgent further workup required |
| Family history of sudden cardiac death | Risk stratification with cardiologist |
| J-point elevation >2 mm in inferior leads | Elevated risk - requires evaluation |
Per Fuster & Hurst's The Heart (15th Ed.): "In patients with early repolarization but no ventricular arrhythmias, no specific treatment is recommended, because the ECG finding is highly prevalent and benign in the vast majority of cases."
Important caveat: Data from a Finnish cohort of ~10,864 participants showed that J-point elevation ≥0.1 mV in inferior leads (not lateral) was associated with a 43% increased risk of arrhythmic death; elevation ≥0.2 mV in inferior leads carried nearly a 3-fold risk increase. The inferior T-wave abnormality on this ECG warrants clinical correlation.
Differential Diagnosis for ST Elevation
These conditions should be considered and excluded clinically:
- Benign early repolarization (most likely given age, sex, pattern)
- Acute STEMI - excluded if ST segments are concave, stable, and no symptoms
- Acute pericarditis - diffuse ST elevation with PR depression; usually has chest pain
- Left ventricular hypertrophy - would show increased QRS voltage
- Vasospastic (Prinzmetal) angina - transient; resolves spontaneously
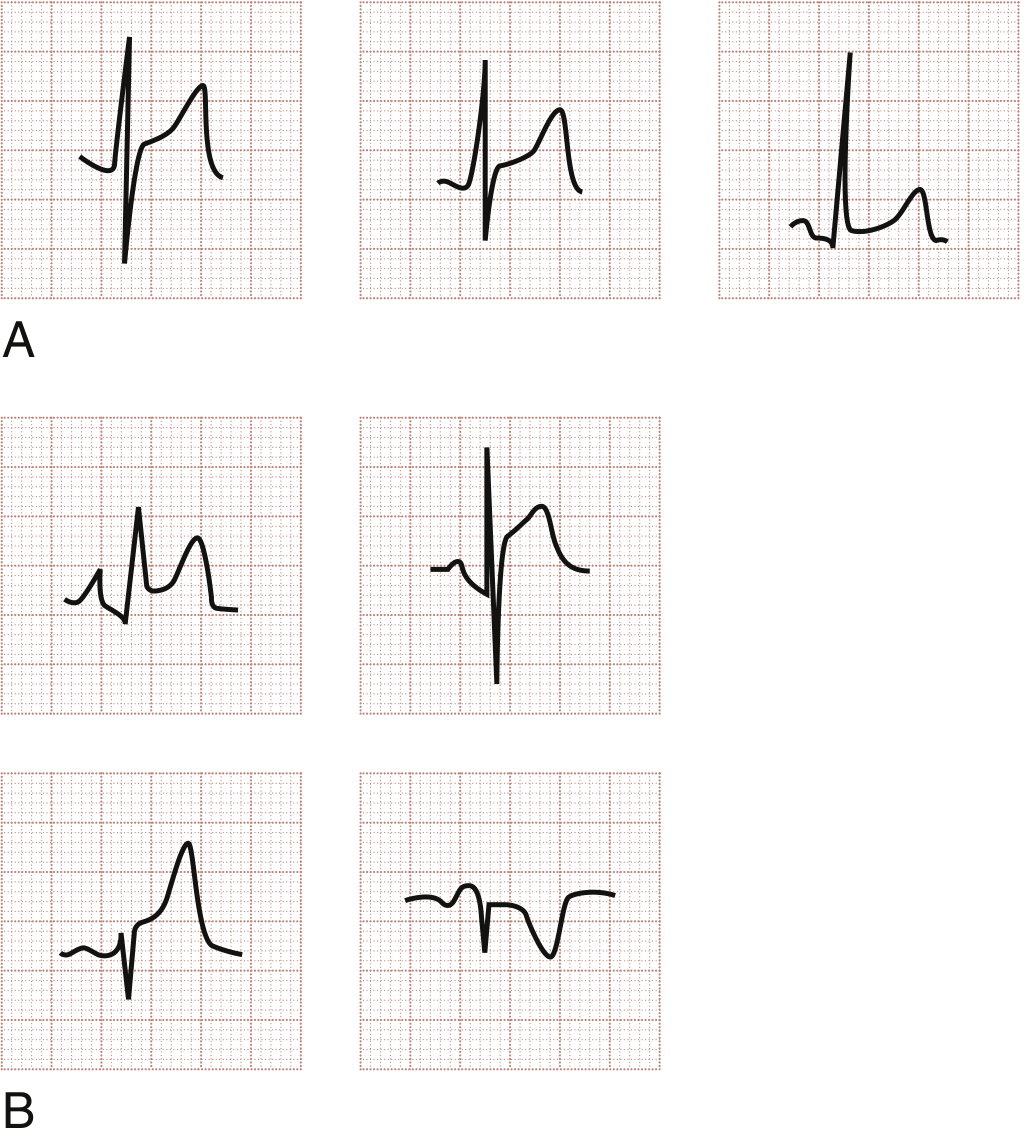
The reference ECG waveform patterns for BER vs. pericarditis are shown below for comparison:
Recommendations
- Correlate clinically - Is the patient symptomatic (chest pain, palpitations, syncope, dyspnea)? This changes urgency significantly.
- Serial ECGs - BER is stable over time. Dynamic change = red flag for ACS or pericarditis.
- Cardiac biomarkers (troponin, CK-MB) if any chest pain is present.
- Electrolyte panel - especially potassium and magnesium, to explain nonspecific T-wave changes and borderline short QTc.
- Echocardiography - if LVH or structural cause is suspected.
- Cardiology referral - if symptoms (syncope, palpitations) are present, or if family history of sudden cardiac death exists.
- No treatment is required for isolated asymptomatic early repolarization per current guidelines.
Summary
This ECG shows sinus rhythm at 62 bpm with lateral ST elevation consistent with early repolarization and a nonspecific inferior T-wave abnormality in a 36-year-old male. The findings are most likely benign but require correlation with symptoms, history, and possibly serial ECGs and biomarkers to exclude acute coronary syndrome or pericarditis. The borderline short QTc (332 ms) should also be noted.
Recent evidence note: A 2025 meta-analysis (PMID: 40306149) confirmed early repolarization is associated with a modestly increased mortality risk overall, reinforcing the importance of clinical context in interpretation.
This analysis is based on the machine-printed ECG parameters and the automated interpretation. Final clinical interpretation should always be made by a qualified physician in conjunction with the patient's clinical presentation.
This is a shared conversation. Sign in to Orris to start your own chat.