Give me ingles and cohens contents in conservative dentistry . I need only contents like which topics are there in those textbooks
Ingle's Endodontics table of contents chapters list
table of contents chapters list
Cohen's Pathways of the Pulp table of contents chapters list 11th edition
table of contents chapters list
Ingle's Endodontics 7th edition complete chapter list table of contents
complete chapter list table of contents all 40 chapters
Ingle's Endodontics (7th Edition)
VOLUME 1
The Science of Endodontics
- Structure and Function of the Dentin-Pulp Complex
- Morphology of Teeth and Their Root Canal Systems
- Microbiology of Endodontic Disease
- Immunology of Pulpal and Periapical Diseases
- Periradicular Disease
- Pathobiology of Apical Periodontitis
- Dental Innervations and Pain of Pulpal Origin
The Practice of Endodontics - Diagnosis
- Examination and Diagnosis of Pulp, Root Canal, and Periapical/Periradicular Conditions
- Imaging Devices and Techniques
- 9A. Analog Radiography
- 9B. Digital Radiography
- 9C. Cone Beam Computed Tomography
- 9D. Magnetic Resonance Imaging
- 9E. Ultrasound
- Imaging Interpretation
Clinical Decision-Making
- Treatment Planning and Case Selection
- Endodontic Considerations in Dental Trauma
- Crown-Originating Dental Fractures
- Vertical Root Fractures
- Pathologic Tooth Resorption
- Rhinosinusitis and Endodontic Disease
- Nonodontogenic Toothache and Chronic Head and Neck Pain
Management
- Management of Pain, Fear, and Anxiety in the Endodontic Patient
- Preparation for Endodontic Treatment
- Preparation of the Coronal and Radicular Spaces
VOLUME 2
- Cleaning and Shaping the Root Canal System
- Root Canal Irrigants and Disinfection
- Obturation of the Root Canal System
- Endodontic Orthograde Retreatment and Management of Mishaps
- Endodontic Surgery
- Endodontic Instruments and Armamentarium
- Management of Immature Teeth with Open Apices
- Intentional Replantation of Endodontically Treated Teeth
- Regenerative Endodontics
- Management of Endodontic Abscesses/Cellulitis, Cysts, and Flare-ups
- Management Considerations for the Medically Complex Endodontic Patient
- Drug Interactions and Laboratory Tests
Prognosis
- Outcomes of Endodontic Therapy
- Achieving Long-term Success with Endodontic Therapy
Interdisciplinary Endodontics
- Contemporary Restoration of Endodontically Treated Teeth
- Endodontic-Periodontal Interrelationships
- Endodontic Therapy in the Elderly Patient
- Endodontic Therapy in the Pediatric Patient
- Interrelationships of Endodontics and Orthodontics in Treatment Planning and Patient Treatment
- Tooth Discoloration and Bleaching of Non-vital Teeth
Cohen's Pathways of the Pulp (11th Edition)
Intro
- A View to the Future
Part 1 - The Core Science of Endodontics
- Diagnosis
- Radiographic Interpretation (New)
- Case Assessment and Treatment Planning
- Pain Control (New)
- Tooth Morphology, Isolation, and Access Preparation
- Cleaning and Shaping of the Root Canal System
- Obturation of the Root Canal System
- Non-Surgical Re-Treatment
- Periradicular Surgery
- Regenerative Endodontics
- Evaluation of Outcomes (New)
- Structure and Functions of the Dental-Pulp Complex
- Pulpal Reactions to Caries and Dental Procedures
- Endodontic Microbiology and Treatment of Infections
- Pathobiology of Apical Periodontitis
- Root Resorption (New)
- Diagnosis of the Non-Odontogenic Toothache
- Management of Endodontic Emergencies
- Management of Iatrogenic Events (New)
- Dental Trauma
- Cracks and Fractures
- Restoration of the Endodontically Treated Tooth
- Pediatric Endodontics
- Endodontic and Periodontic Interrelationships
- Effects of Age on Endodontics
- Vital Pulp Therapy (New)
- Bleaching Procedures (New)
Online Chapters
- Understanding and Managing the Anxious Patient
- Endodontic Records and Legal Responsibilities
- Endodontic Practice Management
- Ingle's (7th ed.) is a 2-volume, 40-chapter reference text, more encyclopedic in scope, with greater depth on basic sciences, imaging modalities, and interdisciplinary topics.
- Cohen's (11th ed.) is a single-volume, 30-chapter text that's more clinically organized, widely used as a primary textbook in dental schools, with stronger emphasis on step-by-step clinical procedures and newer chapters on vital pulp therapy, bleaching, and outcome evaluation.
Is there any textbooks available for conservative dentistry
standard textbooks conservative dentistry operative dentistry list
Core Textbooks for Conservative Dentistry
1. Sturdevant's Art and Science of Operative Dentistry
- Authors: Theodore Roberson, Harald Heymann, Edward Swift
- Edition: 6th / 7th
- Considered the gold standard reference for operative dentistry worldwide. Covers cariology, tooth preparation, restorative materials, and all cavity classifications.
2. Textbook of Operative Dentistry - Nisha Garg & Amit Garg
- Widely used in Indian dental colleges (BDS)
- Covers cavity preparation, dental materials, pulp biology, caries management
- Simple, exam-oriented language
3. Pickard's Manual of Operative Dentistry
- Authors: Edwina Kidd, Ole Fejerskov
- Short, concise, evidence-based - popular in UK curriculum
4. Fundamentals of Operative Dentistry: A Contemporary Approach
- Authors: Summitt, Robbins, Schwartz
- Edition: 3rd / 4th
- Very comprehensive for understanding the biological basis of operative procedures
5. Conservative Dentistry - Marzouk
- Full title: Art and Science of Conservative Dentistry by Marzouk, Simonton & Gross
- Classic reference covering all aspects of restorative and operative dentistry
6. Dental Caries: The Disease and Its Clinical Management
- Authors: Fejerskov & Kidd
- Best book specifically for understanding caries science
7. Craig's Restorative Dental Materials
- Authors: Sakaguchi & Powers
- Best text for dental materials used in conservative dentistry
8. Textbook of Conservative Dentistry - Garg & Garg (Indian edition)
- Separate from the operative dentistry book - covers endodontics + restorative together
Endodontics (sub-speciality of Conservative Dentistry)
| Book | Author |
|---|---|
| Cohen's Pathways of the Pulp (11th ed.) | Hargreaves & Berman |
| Ingle's Endodontics (7th ed.) | Rotstein & Ingle |
| Grossman's Endodontic Practice | Grossman / Walton & Torabinejad |
| Textbook of Endodontics - Nisha Garg | Nisha Garg |
Direct and indirect tooth coloured restorations for 25 marks exam like answer with images please give me
direct indirect tooth coloured restorations composite resin ceramic veneer inlay onlay conservative dentistry
direct indirect tooth coloured restorations composite resin ceramic classification properties indications
composite resin classification GC filler matrix types direct restoration dentistry diagram
ceramic veneer porcelain inlay onlay indirect tooth coloured restoration clinical steps images
glass ionomer cement GIC composition structure properties restorative dentistry diagram
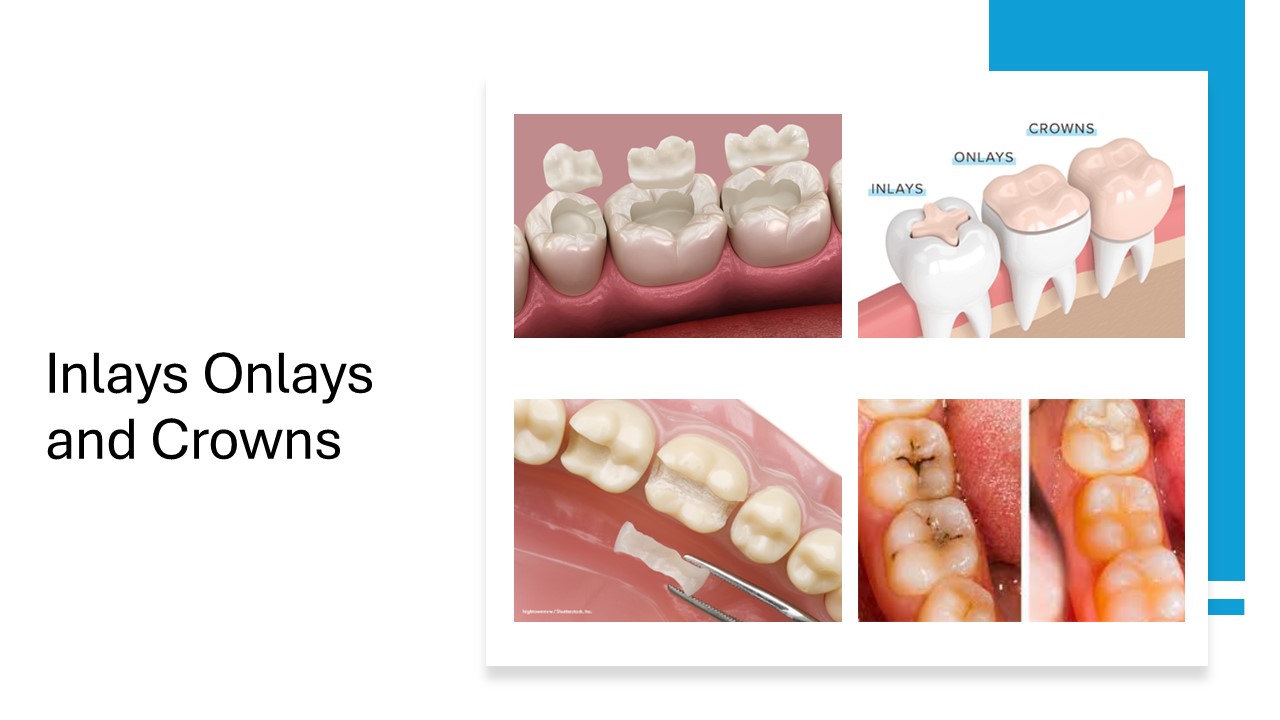
Direct and Indirect Tooth-Coloured Restorations
INTRODUCTION
A. DIRECT TOOTH-COLOURED RESTORATIONS
I. Composite Resin
1. Definition
2. Composition
| Component | Examples |
|---|---|
| Organic matrix (resin) | Bis-GMA, UDMA, TEGDMA |
| Inorganic filler | Quartz, silica, borosilicate glass, hydroxyapatite |
| Coupling agent | Silane (binds matrix to filler) |
| Initiator/Accelerator | Camphorquinone (light cure); BPO/amine (self cure) |
| Inhibitor | BHT (prevents premature polymerisation) |
| Pigments | Iron oxides (for shade matching) |
3. Classification (Based on Filler Particle Size)
| Type | Filler Size | Properties |
|---|---|---|
| Macrofilled (Traditional) | 10-100 µm | High strength, poor polish |
| Microfilled | 0.04-0.4 µm | Excellent polish, low strength |
| Hybrid | 0.6-1 µm + 40 nm | Good balance |
| Microhybrid | 0.4-1 µm | Most widely used |
| Nanofilled | 5-75 nm | Best polish + strength |
| Nanohybrid | Nano + micro | Best overall properties |
4. Properties
- Aesthetic: Excellent shade matching to natural tooth
- Adhesive: Bonds via acid-etch and bonding agents
- Polymerisation shrinkage: 2-4% (major disadvantage)
- Compressive strength: 250-300 MPa
- Radiopacity: Added by barium/zirconia fillers
- Thermal expansion: Higher than tooth structure
5. Indications
- Class I, II, III, IV, V cavities
- Diastema closure
- Composite veneers
- Core build-up
- Repair of fractured teeth
6. Advantages
- Excellent aesthetics
- Conservative preparation (adhesive)
- Direct bonding - no pins/slots needed
- Repairs are possible
- Less expensive
7. Disadvantages
- Polymerisation shrinkage leading to microleakage
- Wear in high-stress areas
- Technique-sensitive
- Colour change/staining over time
8. Clinical Steps for Composite Restoration
- Shade selection (before isolation)
- Isolation with rubber dam
- Cavity preparation (conservative)
- Acid etching (37% phosphoric acid - 15-30 sec enamel, 15 sec dentin)
- Bonding agent application and light cure
- Incremental placement (2 mm increments)
- Light curing each increment (20-40 sec)
- Finishing and polishing

II. Glass Ionomer Cement (GIC)
1. Introduction
2. Composition
| Component | Details |
|---|---|
| Powder | Fluoro-aluminosilicate glass |
| Liquid | Aqueous solution of polyacrylic acid (+ tartaric acid) |
3. Setting Reaction
- Stage 1: Dissolution - acid attacks glass, releases Ca²⁺, Al³⁺, F⁻
- Stage 2: Gelation - polysalt matrix forms
- Stage 3: Maturation - cross-linking continues (24-48 hrs)
4. Classification
| Type | Use |
|---|---|
| Type I | Luting/Cementing |
| Type II | Restorative - aesthetic (IIa), reinforced (IIb) |
| Type III | Liner/Base |
| Type IV | Pit & fissure sealant |
| Type V | Orthodontic cement |
| Type VI | Core build-up |
| Type VII | Fluoride releasing |
| Type VIII | ART (Atraumatic Restorative Treatment) |
| Type IX | Deciduous teeth/special populations |
5. Properties
- Chemical adhesion to enamel and dentin (ionic bonds with Ca²⁺)
- Fluoride release - cariostatic effect (major advantage)
- Biocompatible - minimal pulpal irritation
- Low mechanical strength - not ideal for occlusal surfaces
- Thermal expansion - similar to tooth structure
6. Indications
- Class III and V cavities (non-stress bearing)
- Deciduous tooth restorations
- High caries risk patients
- Cervical erosion/abrasion lesions
- Sandwich technique with composite
- ART in community settings
7. Resin-Modified GIC (RMGIC)
- Contains 10-20% HEMA + GIC components
- Set by dual mechanism - acid-base + light polymerisation
- Better strength and moisture tolerance than conventional GIC
- Examples: Vitremer, Fuji II LC
8. Compomers (Polyacid-Modified Composite)
- Composite matrix + GIC filler
- Light cured only
- Limited fluoride release
- Better aesthetics than GIC
- Examples: Dyract, Compoglass
B. INDIRECT TOOTH-COLOURED RESTORATIONS

I. Ceramic/Porcelain Restorations
Types
- Porcelain inlays/onlays
- Ceramic veneers
- All-ceramic crowns
- CAD/CAM milled ceramics
1. Classification of Ceramics
| Category | Examples | Strength |
|---|---|---|
| Feldspathic porcelain | Conventional porcelain | Low |
| Leucite-reinforced | IPS Empress | Moderate |
| Lithium disilicate | IPS e.max | High (400 MPa) |
| Zirconia (Y-TZP) | Lava, Cercon | Very High (1000+ MPa) |
| Alumina-based | In-Ceram Alumina | High |
2. Properties of Ceramics
- Aesthetics: Most natural appearance (translucency like enamel)
- Hardness: Very high (can wear opposing teeth)
- Brittle - fractures under tensile stress
- Biocompatible - excellent gingival response
- Colour stable - no staining
- Thermal conductivity - low
3. Indications for Ceramic Inlays/Onlays
- Class I and II restorations in esthetic zones
- Large defects needing cusp coverage
- Replacement of large failing restorations
- When high strength and aesthetics both needed
4. Contraindications
- Insufficient tooth structure for support
- Heavy bruxism (parafunctional habits)
- Inability to achieve isolation for bonding
- Young patients (large pulp chambers)
5. Advantages of Indirect Restorations
| Advantage | Explanation |
|---|---|
| Reduced polymerisation shrinkage | Shrinkage occurs outside the mouth |
| Better contours | Lab fabrication allows ideal contact/contour |
| Superior wear resistance | Ceramics outlast direct composites |
| Better marginal adaptation | Precise fit on die |
| Improved physical properties | Lab/industrial conditions |
| Variety of materials | Ceramics, composite, CAD/CAM |
6. Disadvantages
- Higher cost - lab fees
- Two appointments needed
- Provisional restoration required
- Brittleness of ceramics - fracture risk during try-in
- Difficult to polish after cementation
- Irreversible preparation
7. Clinical Steps for Ceramic Inlay/Onlay
- Local anesthesia and rubber dam isolation
- Cavity preparation (divergent walls, flat floor, rounded line angles)
- Impression with addition silicone/polyether
- Shade selection
- Provisional restoration placement
- Provisional removal
- Try-in of restoration (fit, contacts, occlusion)
- Tooth preparation - etching (if porcelain: HF acid etching + silane)
- Adhesive cementation with resin cement
- Light curing and excess cement removal
- Final occlusal check and adjustment

II. Indirect Composite Restorations
- Composite fabricated in the lab and cemented
- Advantages over ceramic: Easier to polish, easier repair, less brittle
- Disadvantages: More wear than ceramic, higher polymerisation shrinkage than ceramic
- Materials: Solidex, Belleglass, Targis
III. CAD/CAM Restorations
- Computer-Aided Design / Computer-Aided Manufacturing
- Chairside systems: CEREC (Sirona), E4D
- Lab systems: Lava (3M), Procera (Nobel)
- Materials: Feldspathic blocks, Lithium disilicate (IPS e.max CAD), Zirconia
- Advantages: Single visit, no temporaries, precise fit
COMPARISON: Direct vs Indirect
| Feature | Direct (Composite) | Indirect (Ceramic) |
|---|---|---|
| Visits | Single visit | Two visits |
| Cost | Lower | Higher |
| Polymerisation shrinkage | Present (2-4%) | Minimal |
| Wear resistance | Moderate | Excellent |
| Aesthetics | Good | Excellent |
| Marginal adaptation | Good | Excellent |
| Repair | Easy | Difficult |
| Brittleness | No | Yes (ceramic) |
| Indications | Small-medium cavities | Large cavities, high aesthetics |
CONCLUSION
Find research papers on ceramic inlay longevity vs composite
ceramic inlay longevity survival composite resin
indirect composite inlay ceramic comparison clinical outcomes
Research Papers: Ceramic Inlay Longevity vs Composite
TIER 1 - Systematic Reviews & Meta-Analyses (Highest Evidence)
- 21 studies included (1983-2020), published in J Conserv Dent
- Key Findings:
| Material | 5-Year Survival | 10-Year Survival |
|---|---|---|
| Resin (indirect composite) | 86% | 75% |
| Feldspathic porcelain | 90% | 91% |
| Glass ceramic | 92% | 89% |
- Conclusion: Ceramic (both types) significantly outperforms resin at 5 and 10 years. Most common failures: fracture (6.2%), endodontic problems (3%), secondary caries (1.7%), debonding (0.9%)
- 14 studies (5,811 restorations), published in J Dent Res
- Key Findings:
- Glass-ceramics and feldspathic porcelain: 92-95% survival at 5 years, 91% at 10 years
- Main failure cause: fractures/chipping (4%), then endodontic complications (3%)
- Type of ceramic (feldspathic vs glass-ceramic), study design, follow-up time, and setting did NOT significantly affect survival
- Conclusion: Ceramic inlays/onlays/overlays show high survival at both 5 and 10 years
- 12 studies, 946 restorations, published in Clin Oral Investig
- Key Findings:
- Indirect composite has 18% higher failure rate vs gold over 5-7 years (RD = -0.18; 95% CI: -0.27 to -0.09; p=0.0002)
- Lithium disilicate and indirect composite show comparable survival in short-term follow-up
- Gold > Lithium disilicate ≈ Indirect composite > (Leucite ≈ Indirect composite)
- Conclusion: Medium-quality evidence supports lithium disilicate as a reliable alternative with survival comparable to indirect composite in the short term, but gold remains superior
- 7 studies (6 RCTs), published in Clin Oral Investig
- Key Findings:
- CAD/CAM resin-based composite success rate: 85.7 - 100%
- Ceramic partial coverage success rate: 93.3 - 100%
- Fractures and debonding = most common failures
- Conclusion: CAD/CAM resin-matrix ceramics are a reliable alternative to conventional ceramics with comparable short-term performance - but long-term data is still lacking
TIER 2 - Meta-Analysis
- Classic landmark study, published in J Adhes Dent
- Annual failure rates:
| Material | Annual Failure Rate |
|---|---|
| Amalgam | 0 - 7% |
| Direct composite | 0 - 9% |
| Glass ionomer | 1.4 - 14.4% |
| Composite inlays | 0 - 11.8% |
| Ceramic restorations | 0 - 7.5% |
| CAD/CAM ceramic | 0 - 4.4% |
| Cast gold | 0 - 5.9% |
- Principal reasons for failure: secondary caries, fracture, marginal deficiencies, wear, postoperative sensitivity
TIER 3 - Clinical Studies / Retrospective
- 91 patients, published in Dent Mater
- Key Findings:
- Lithium disilicate (LiDiSi) survival: 96.8% at mean 7.8 years
- Indirect composite (RBC) survival: 84.9% at mean 7.8 years
- Annual failure rate: 0.2% (LiDiSi) vs 1.0% (RBC)
- Both materials excellent in first 6 years; by year 15, RBC dropped to 60% survival
- Risk factors: material type (OR=6.8), poor oral hygiene (OR=8.0), bruxism (OR=1.9)
- Conclusion: Similar short-term survival, but significantly more long-term failures expected for indirect composites
- 783 ceramic restorations, up to 116 months follow-up, published in J Dent
- Key Findings:
- 96.7% still in place at last observation
- Overall survival probability: 90% (95% CI: 0.86-0.94) after 45 months
- No significant influence from: endodontic status, tooth type, operator experience, gender
Summary of Key Numbers
| Study | Ceramic Survival | Composite/Resin Survival | Follow-up |
|---|---|---|---|
| Naik 2022 (SR+MA) | 90-92% (5yr), 89-91% (10yr) | 86% (5yr), 75% (10yr) | 5-10 yrs |
| Morimoto 2016 (SR+MA) | 92-95% (5yr), 91% (10yr) | Not directly compared | 5-10 yrs |
| Bresser 2023 (SR+MA) | LiDiSi ≈ composite (short-term) | 18% higher failure vs gold | 5-7 yrs |
| Lempel 2023 (Retrospective) | 96.8% (LiDiSi) | 84.9% (RBC) | 7.8 yrs |
| Fathy 2022 (SR) | 93.3-100% | 85.7-100% | Variable |
Please give me hand drawn images for cavity preparation for exam