Crvo and prp laser
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
I have all the information needed. Here is the complete, structured answer:
CRVO and PRP Laser
Central Retinal Vein Occlusion (CRVO) - Overview
CRVO is classified into three types based on severity:
| Type | Features |
|---|---|
| Impending CRVO | Younger patients, mild venous dilatation/tortuosity, few scattered dot-blot haemorrhages, mild or no macular oedema. Usually good prognosis but can deteriorate. |
| Non-ischaemic CRVO | More common. Sudden painless monocular vision fall. Tortuosity and dilatation of all retinal vein branches, dot/blot/flame haemorrhages in all quadrants. Absent or mild RAPD. ~1/3 progress to ischaemic CRVO. |
| Ischaemic CRVO | Substantially reduced retinal perfusion with capillary closure. VA typically "counting fingers" or worse. RAPD present. High risk of rubeosis iridis (~50%) and neovascular glaucoma. |
Key diagnostic pointer: VA <6/60 + RAPD = significant ischaemia + poor visual prognosis in CRVO.
Ischaemic CRVO - Fundus & Investigations
Fundus findings:
- Severe tortuosity and engorgement of all retinal vein branches
- Extensive deep blot and flame haemorrhages (peripheral and posterior)
- Prominent cotton-wool spots
- Optic disc swelling and hyperaemia
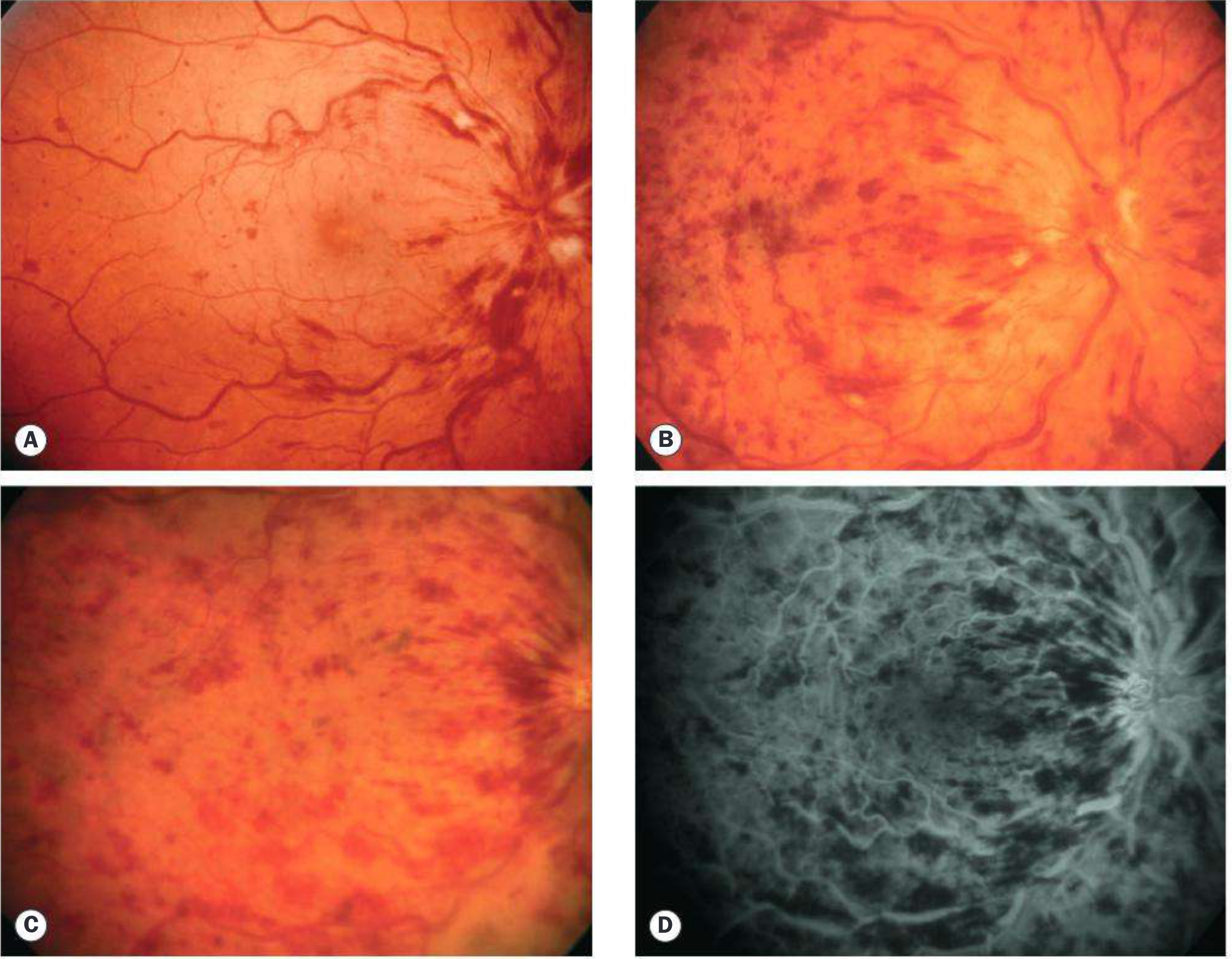
FA findings: Marked delay in arteriovenous transit time, extensive capillary non-perfusion, vessel wall staining/leakage. More than 10 disc areas of capillary non-perfusion = substantially increased neovascularization risk.
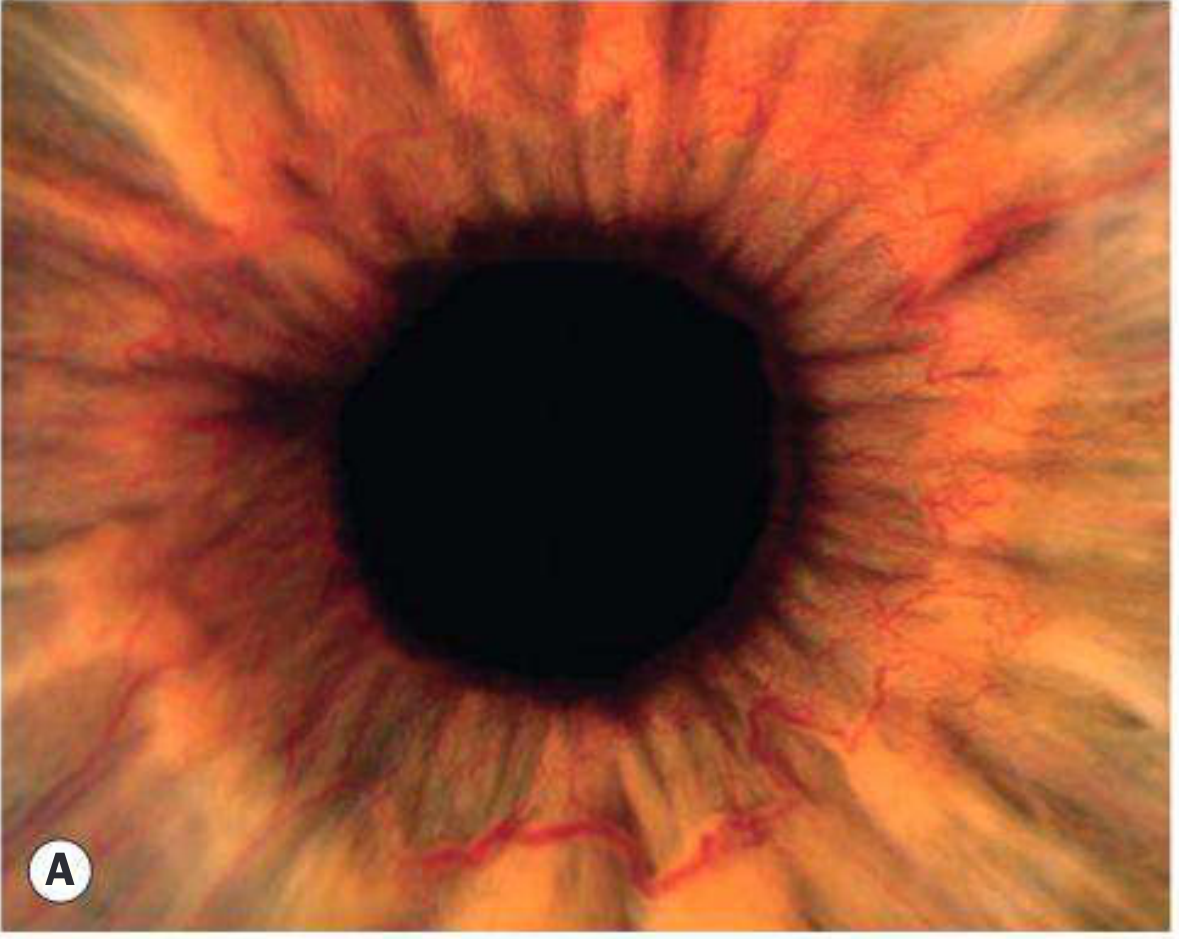
NVI (Rubeosis iridis): Develops in ~50% of ischaemic CRVO, typically 2-4 months after occlusion ("hundred-day glaucoma"). Gonioscopy is mandatory before pupillary dilatation (angle NV can occur without visible rubeosis).
Rubeosis iridis at the pupillary border:
Treatment of Macular Oedema in CRVO
Treatment is indicated when VA is worse than 6/9 and/or central macular thickness >250 µm on OCT. It is unlikely to benefit if VA is 6/120 or worse.
1. Intravitreal anti-VEGF agents (current standard of care):
- Ranibizumab (CRUISE study): monthly injections x6 months superior to placebo
- Aflibercept (COPERNICUS study): effective even on "as-needed" protocol
- Bevacizumab: effective in practice, commonly used
2. Intravitreal dexamethasone implant (Ozurdex 700 µg) - GENEVA trial:
- Substantial visual and anatomical improvement in first 2 months
- Declines to baseline by 6 months; can be repeated after 4-6 months
- Administer within 90 days of CMO onset for best results
- COMRADE study: ranibizumab shows better VA than dexamethasone at 6 months
- Side effects: IOP elevation, cataract
3. Intravitreal triamcinolone (SCORE study):
-
25% improve by 3+ lines at 1 year (vs 7% controls), using 1 mg preservative-free preparation
- Higher risk of IOP elevation with 4 mg vs 1 mg
4. Laser photocoagulation for macular oedema:
- Although anatomically improves oedema, laser is not beneficial for visual outcome in CRVO (except possibly in some younger patients)
PRP (Pan-Retinal Photocoagulation) in CRVO
When NOT to do PRP:
There is NO benefit in performing PRP before the development of iris and angle neovascularization. Prophylactic PRP in ischaemic CRVO is not recommended.
Indication for PRP:
PRP is indicated when NVI or angle neovascularization develops. It should be performed without delay once these appear.
PRP Parameters:
| Parameter | Value |
|---|---|
| Number of burns | 1500-2000 initially |
| Duration | 0.05-0.1 seconds |
| Spacing | One burn width apart |
| Energy | Sufficient for moderate reaction |
| Avoid | Areas of retinal haemorrhage |
| Approach | Treatment may be fractionated (split into sessions) |
| Further photocoagulation | Commonly required |
Special situations:
- Poor retinal view: Indirect ophthalmoscopic PRP, or performed in the operating room with iris hooks
- Opaque media: Trans-scleral cryotherapy as alternative or adjunct
PRP + Anti-VEGF:
Adjunctive intravitreal anti-VEGF injections are commonly given every 6 weeks until stabilization:
- Leads to faster regression of NV than PRP alone
- Reduces macular oedema simultaneously
- Onset of NVG may be delayed by up to 18 months
- These patients need 3-monthly follow-up for at least 2-3 years
What PRP does and doesn't do:
- Does: Induces regression of neovascularization; prevents progression to neovascular glaucoma if performed early
- Does not: Reverse an established fibrovascular membrane
Management of Neovascular Glaucoma (NVG) in CRVO
If NVG develops despite PRP:
- Medical IOP treatment (avoid miotics; use topical atropine 1% twice daily)
- Cyclodiode (ciliary body ablation) if IOP uncontrolled
- Filtration surgery (glaucoma drainage device or trabeculectomy with MMC) if VA is HM or better
- Preoperative anti-VEGF to control active neovascularization before surgery
Review Schedule
- Ischaemic CRVO: Monthly for 6 months, then every 3 months for 2-3 years
- Non-ischaemic CRVO: Review at 3 months; discharge usually at 18-24 months
- Once optic disc collaterals develop, neovascularization risk reduces
Prognosis
- Main cause of poor vision after CRVO: chronic macular oedema
- Ischaemic CRVO: generally very poor visual prognosis due to macular ischaemia
- Non-ischaemic CRVO without progression: ~50% return to normal or near-normal VA
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th edition
This is a shared conversation. Sign in to Orris to start your own chat.