Explain heart pathology with pictures
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent! I now have all the images and content I need to write a comprehensive, well-illustrated explanation of heart pathology. Let me compose the full response now.
Heart Pathology - A Comprehensive Overview with Pictures
Source: Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease
Overview
Heart disease is the leading cause of death globally, responsible for over 7.5 million deaths per year. The major categories of cardiac pathology are:
- Ischemic Heart Disease (IHD)
- Hypertensive Heart Disease
- Valvular Heart Disease
- Cardiomyopathies
- Congenital Heart Disease
- Pericardial Disease / Myocarditis
1. Ischemic Heart Disease (IHD)
IHD is caused by an imbalance between myocardial oxygen supply and demand. Over 90% of cases are caused by atherosclerotic coronary artery disease (CAD). The clinical spectrum includes:
| Syndrome | Mechanism |
|---|---|
| Stable angina | Fixed atherosclerotic narrowing; pain on exertion |
| Unstable angina | Plaque rupture + partial thrombosis; pain at rest |
| Myocardial Infarction (MI) | Complete occlusion → cardiomyocyte necrosis |
| Sudden cardiac death | Lethal ventricular fibrillation from ischemia |
| Chronic IHD / CHF | Progressive pump failure from accumulated ischemic damage |
Pathogenesis pathway:
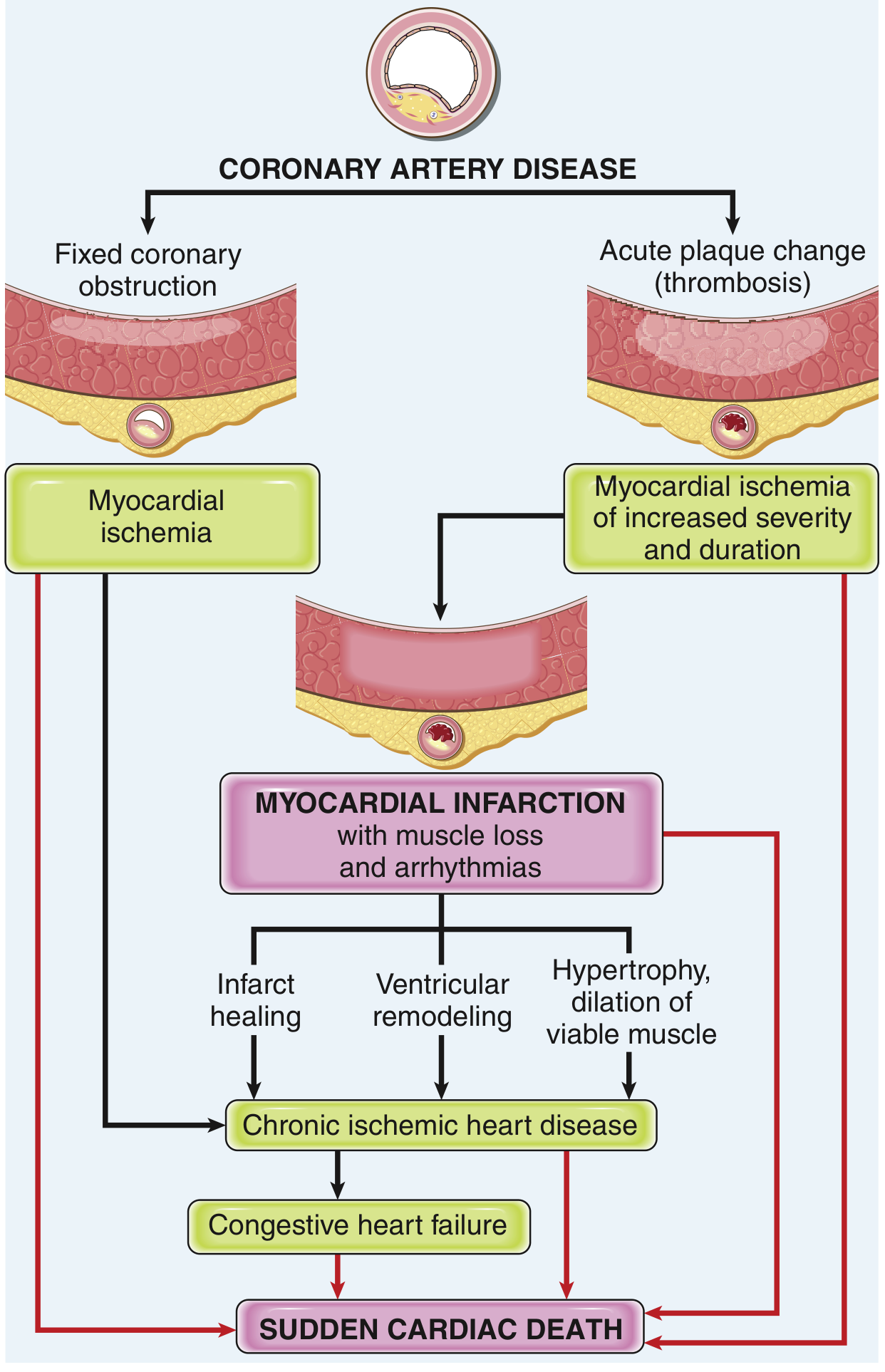
FIG. 9.15 - Robbins Basic Pathology: Pathways in the progression of ischemic heart disease.
Myocardial Infarction (MI)
MI = necrosis of heart muscle from ischemia. The sequence of events:
- Atheromatous plaque erodes or ruptures, exposing subendothelial collagen
- Platelet aggregation + thromboxane A2 release → vasospasm
- Coagulation cascade activation → growing thrombus
- Within minutes, the thrombus completely occludes the coronary lumen
Patterns of infarction depend on which vessel is occluded and whether flow is restored:
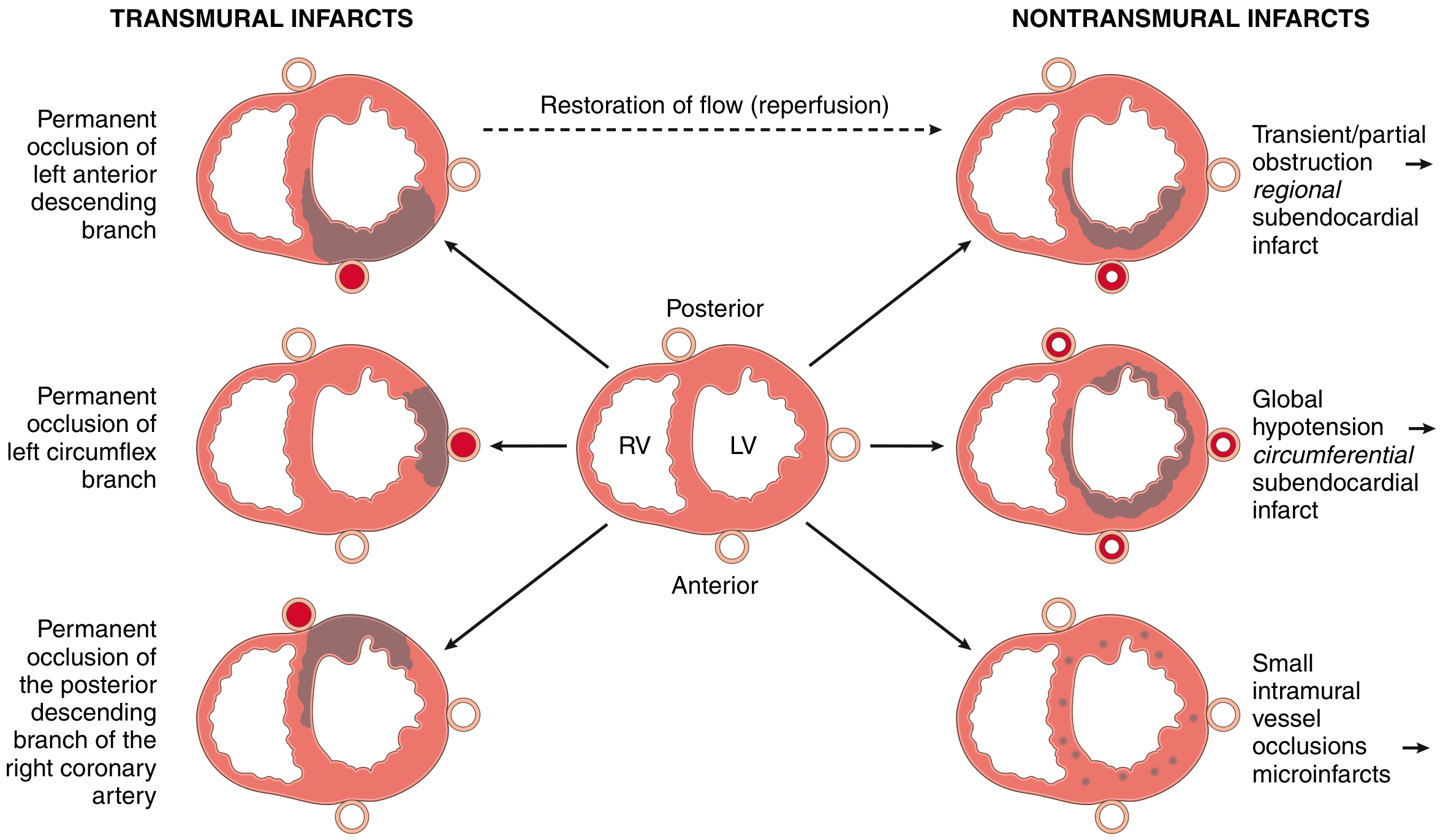
FIG. 9.9 - Robbins Basic Pathology: Dependence of MI on location and nature of diminished perfusion. Left = transmural infarcts from complete occlusion. Right = nontransmural patterns from partial or transient occlusion.
Morphologic evolution of MI (gross and microscopic):
| Time | Gross | Microscopy |
|---|---|---|
| 0-4 hours | None visible | Waviness of fibers at border |
| 4-12 hours | Occasional dark mottling | Coagulation necrosis begins; edema, hemorrhage |
| 12-24 hours | Dark mottling | Coagulation necrosis, pyknosis of nuclei, neutrophilic infiltrate |
| 1-3 days | Yellow-tan center | Ongoing necrosis, dense neutrophil infiltrate |
| 3-7 days | Hyperemic border; soft yellow-tan center | Macrophage phagocytosis at infarct border |
| 7-10 days | Maximally soft, yellow | Granulation tissue with neovascularization |
| 2-8 weeks | Gray-white fibrosis progressing | Scar collagen deposition |
| >2 months | Dense white scar | Dense fibrosis - complete scar |
Gross pathology specimen - acute MI stained with triphenyl tetrazolium chloride (TTC):
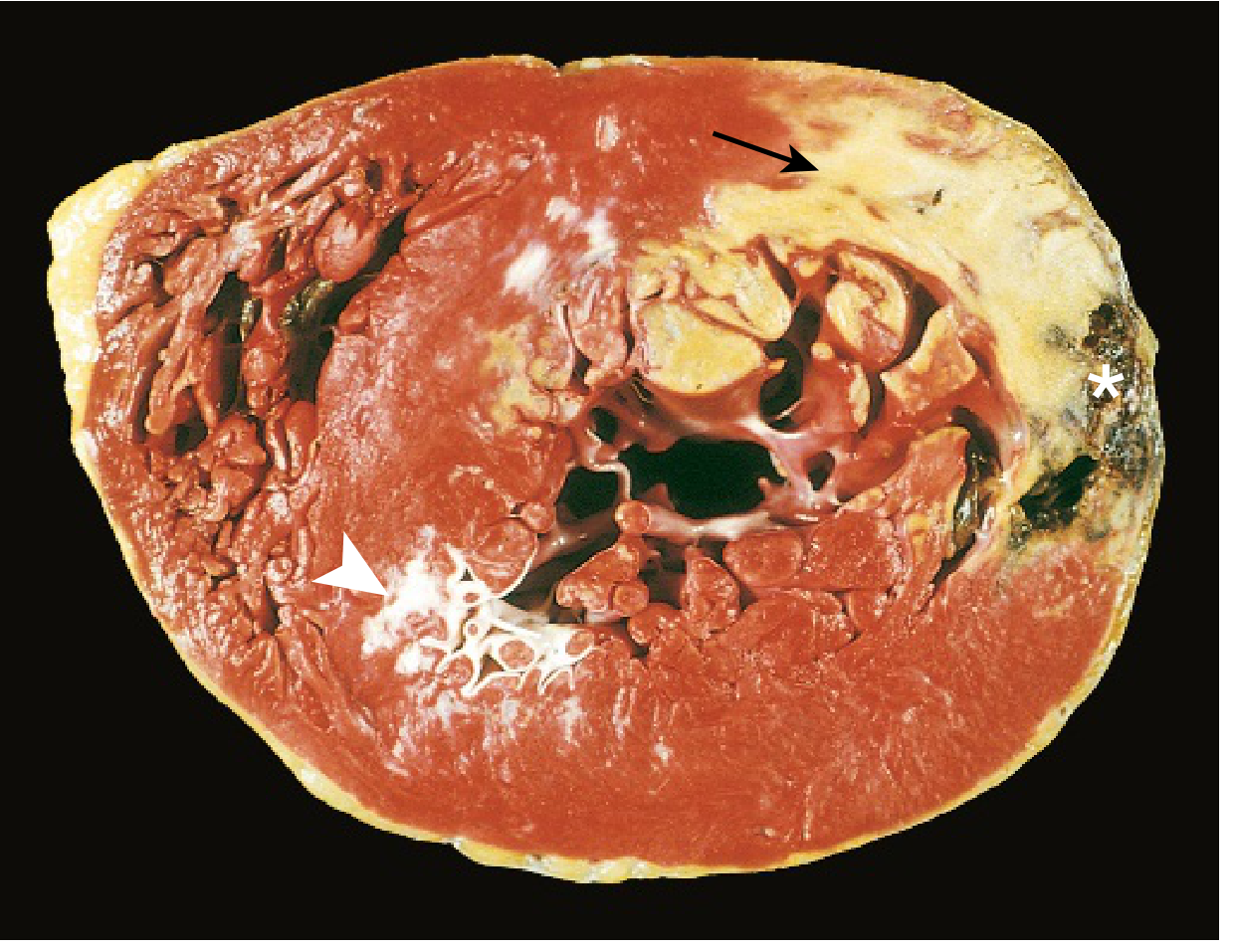
FIG. 9.10 - Robbins Basic Pathology: Acute MI of the posterolateral LV demonstrated by lack of TTC staining in areas of necrosis (arrow = acute infarct, pale/yellow). White arrowhead = old scar from remote infarction. Asterisk = myocardial hemorrhage from ventricular rupture (cause of death).
Complications of MI include:
- Contractile dysfunction - cardiogenic shock
- Papillary muscle rupture → acute mitral regurgitation
- Ventricular wall rupture (3-7 days, peak risk) → cardiac tamponade
- Ventricular septal defect (rupture of necrotic septum)
- Mural thrombus → systemic emboli
- Ventricular aneurysm → paradoxical bulging, arrhythmias
- Arrhythmias → VF is the most common cause of death in the first 24 hours
2. Hypertensive Heart Disease
Sustained hypertension imposes pressure overload on the left ventricle, driving concentric hypertrophy. Key features:
- LV wall thickness >2.0 cm (normal 1.2-1.4 cm)
- Heart weight >500 g (normal ~320-360 g in a 60-70 kg person)
- Microscopy: increased myocyte transverse diameter, "boxcar nuclei" (prominent nuclear enlargement), interstitial fibrosis
- Diastolic dysfunction (stiff LV) precedes systolic dysfunction
- Late-stage: LV dilation and congestive heart failure
Right-sided hypertensive heart disease = cor pulmonale, caused by pulmonary hypertension from diseases like COPD, interstitial fibrosis, or recurrent PE.
3. Valvular Heart Disease
Valves can fail in two ways:
- Stenosis - valve fails to open fully → obstructs forward flow
- Insufficiency / Regurgitation - valve fails to close fully → backflow
Most common causes of acquired valve disease:
| Valve | Common Causes |
|---|---|
| Mitral stenosis | Rheumatic heart disease |
| Mitral regurgitation | MVP, endocarditis, ischemic papillary muscle dysfunction |
| Aortic stenosis | Senile calcification, bicuspid AV, rheumatic disease |
| Aortic regurgitation | Infective endocarditis, Marfan syndrome, rheumatic disease |
Calcific Degenerative Valve Disease (gross pathology):
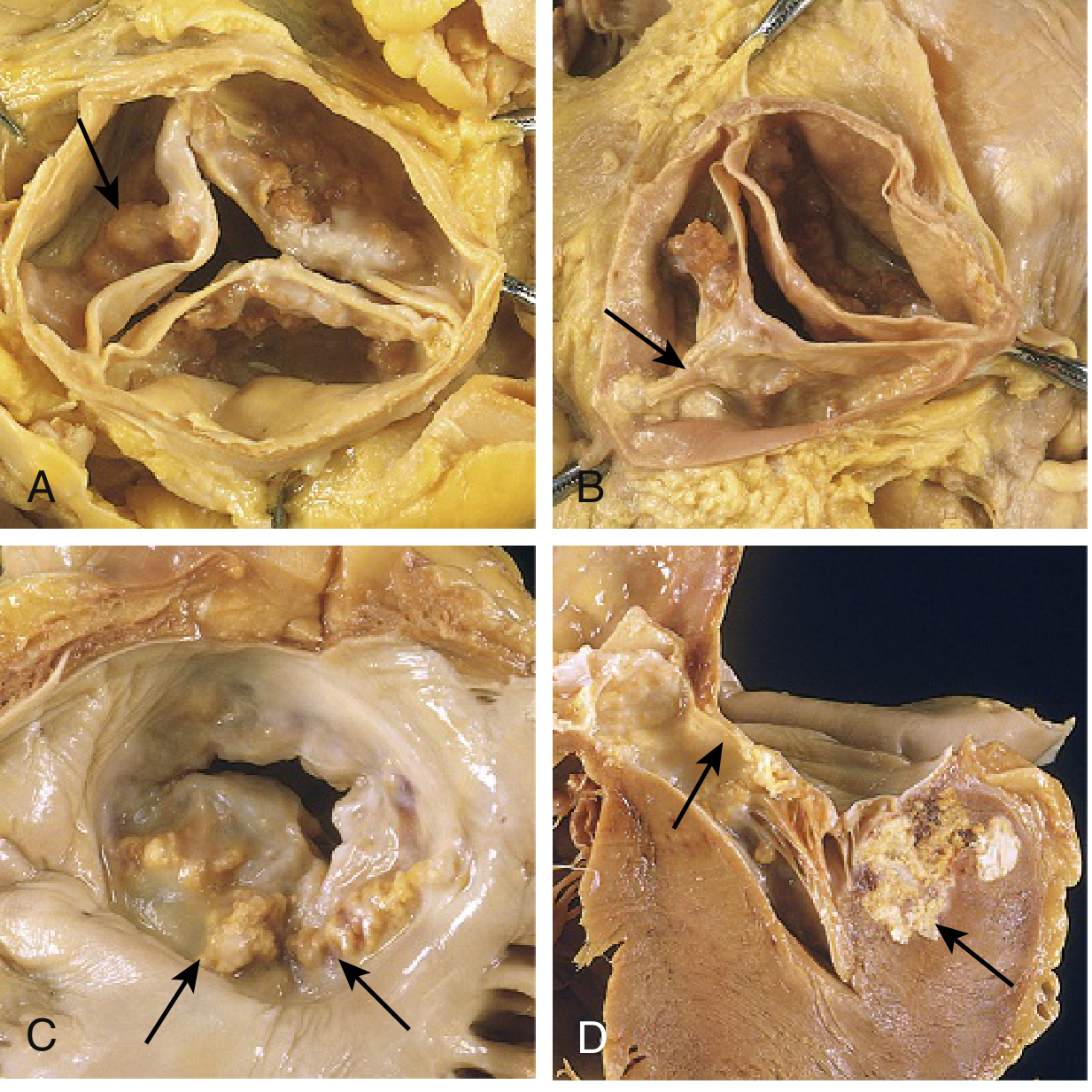
FIG. 9.17 - Robbins Basic Pathology: Calcific valvular degeneration. (A) Aortic stenosis - calcific nodules in sinuses of Valsalva, commissures NOT fused (unlike rheumatic). (B) Bicuspid aortic valve with raphe (arrow). (C-D) Mitral annular calcification, with extension into myocardium (can impinge on the conduction system).
Rheumatic heart disease is caused by cross-reactive antibodies after Group A Streptococcal pharyngitis (molecular mimicry). The mitral valve is most commonly affected. Acute features include:
- Aschoff bodies (foci of fibrinoid necrosis with multinucleated giant cells) - pathognomonic
- Small verrucous vegetations along valve closure line
Chronic changes: leaflet thickening, commissural fusion, chordal shortening → "fish-mouth" or "buttonhole" mitral stenosis orifice.
4. Cardiomyopathies
Cardiomyopathies are diseases of the myocardium itself. There are three major patterns:
Side-by-side comparison of the three types:
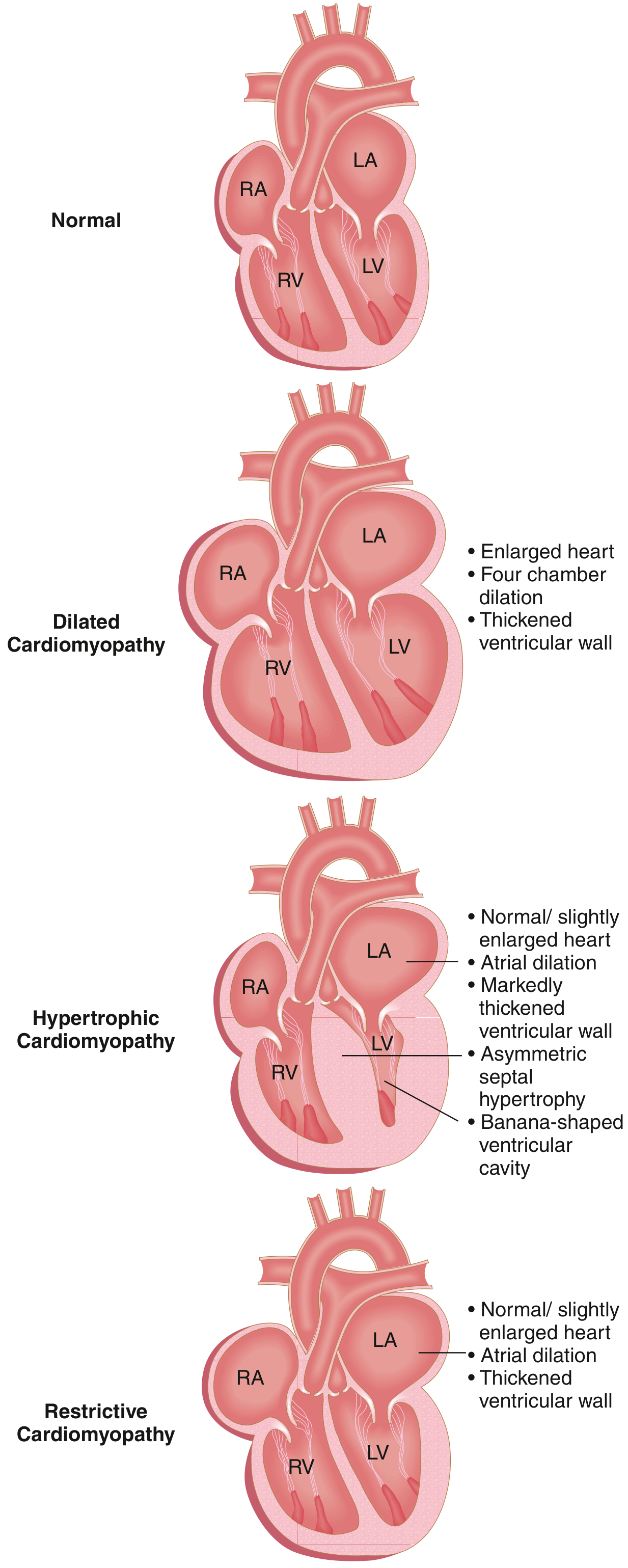
FIG. 9.23 - Robbins Basic Pathology: Three major forms of cardiomyopathy. DCM = systolic dysfunction. HCM and Restrictive = diastolic dysfunction.
Dilated vs Hypertrophic - Causes, Pathology, and Clinical Features:
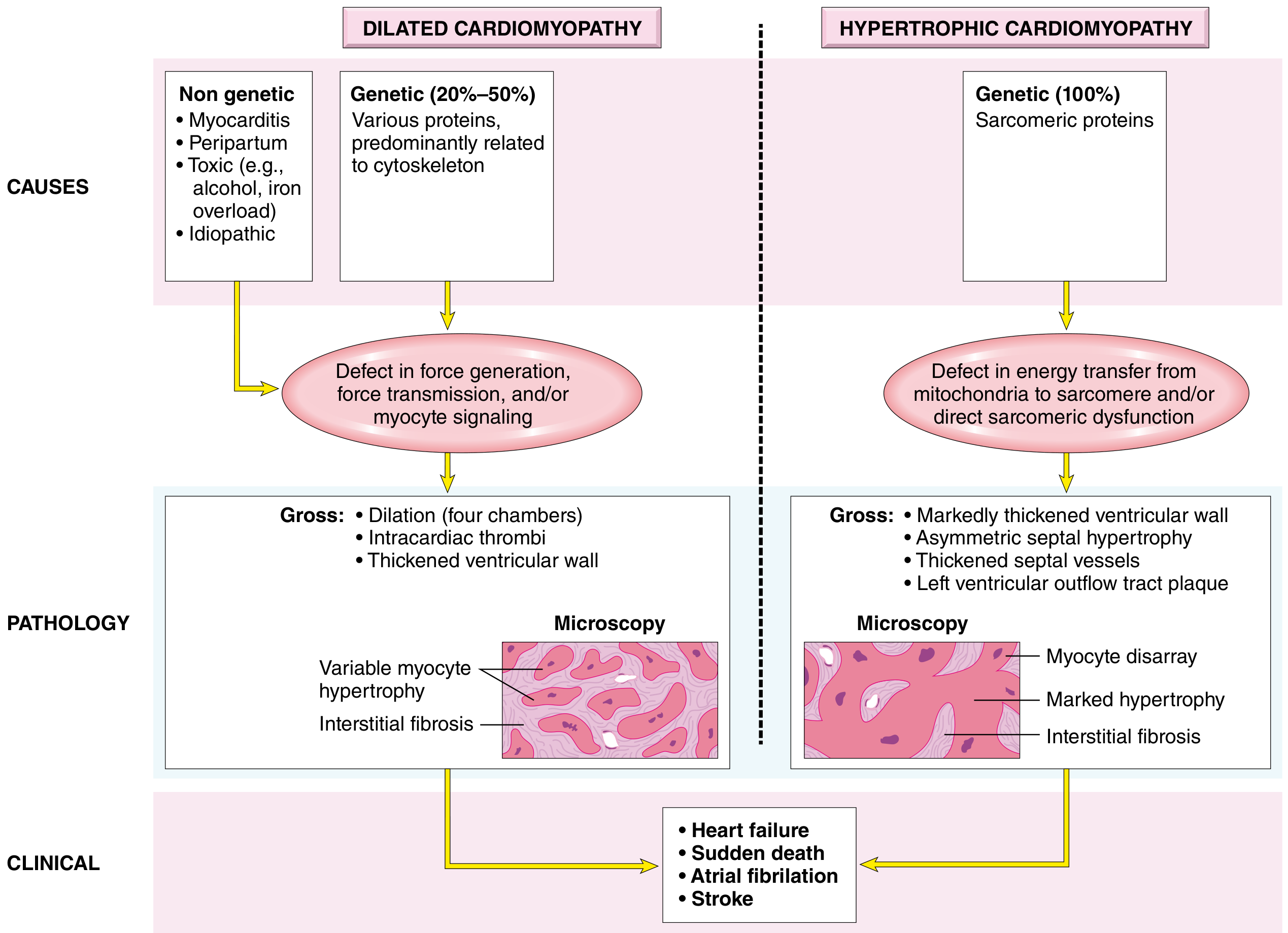
FIG. 12.33B - Robbins Pathologic Basis of Disease: Dilated vs Hypertrophic Cardiomyopathy.
Dilated Cardiomyopathy (DCM)
- Most common (90% of all cardiomyopathies)
- Progressive four-chamber dilation + systolic (contractile) dysfunction
- Causes: genetic (titin, dystrophin, β-myosin mutations), myocarditis (viral), alcohol, peripartum, doxorubicin toxicity
- Gross: flabby, enlarged heart; mural thrombi common → embolic stroke risk
- Micro: variable myocyte hypertrophy + interstitial fibrosis
- Treatment: heart failure therapy; eventual transplant
Hypertrophic Cardiomyopathy (HCM)
- 100% genetic - mutations in sarcomeric proteins (β-MHC, cardiac troponin T, myosin binding protein C)
- Massive asymmetric septal hypertrophy → banana-shaped LV cavity → dynamic outflow obstruction
- Micro: myocyte disarray (chaotically arranged myocytes) - pathognomonic
- Most common cause of sudden cardiac death in young athletes (<35 years)
- Diastolic dysfunction (stiff, non-compliant LV)
Restrictive Cardiomyopathy
- Least common; ventricular walls are stiff, impeding diastolic filling
- Causes: amyloidosis, sarcoidosis, post-radiation fibrosis, hemochromatosis
- Normal/near-normal systolic function; severely impaired diastolic filling
- Bilateral atrial dilation is characteristic
5. Congenital Heart Disease
Congenital heart disease (CHD) affects ~1% of live births. The top 12 lesions account for 85% of all CHD:
| Malformation | Incidence per million live births | % of CHD |
|---|---|---|
| Ventricular septal defect (VSD) | 4482 | 42% |
| Atrial septal defect (ASD) | 1043 | 10% |
| Pulmonary stenosis | 836 | 8% |
| Patent ductus arteriosus (PDA) | 781 | 7% |
| Tetralogy of Fallot | 577 | 5% |
| Coarctation of aorta | 492 | 5% |
| AV septal defect | 396 | 4% |
| Aortic stenosis | 388 | 4% |
| Transposition of great arteries | 388 | 4% |
Key Lesions Explained
Left-to-right shunts (acyanotic initially; may become cyanotic late via Eisenmenger syndrome):
- VSD - most common; harsh holosystolic murmur; spontaneous closure common in small VSDs
- ASD - fixed split S2; pulmonary overcirculation; thromboembolism risk
- PDA - continuous "machinery" murmur; closes with indomethacin (inhibits prostaglandin)
Right-to-left shunts (cyanotic from birth):
- Tetralogy of Fallot (TOF): 4 components - (1) VSD, (2) pulmonary stenosis, (3) aorta overriding the VSD, (4) right ventricular hypertrophy. Classic "boot-shaped heart" on CXR. Presents with cyanosis, "tet spells," squatting (increases SVR).
- Transposition of the great arteries (TGA): Aorta arises from RV, pulmonary artery from LV → two parallel circuits incompatible with life unless ASD/VSD/PDA exists. "Egg on a string" CXR.
Obstructive lesions:
- Coarctation of the aorta: Segmental narrowing, usually postductal (near ligamentum arteriosum). Presents with upper-body hypertension, weak femoral pulses, rib notching on CXR from dilated intercostal collaterals.
6. Myocarditis
Myocarditis = inflammatory disease of the myocardium.
- Most common cause: Viral (Coxsackievirus B, parvovirus B-19, HIV, COVID-19)
- Chagas disease (Trypanosoma cruzi) - most common cause worldwide in South America
- Autoimmune: giant cell myocarditis (rapidly fatal without transplant), sarcoidosis
- Presents with: sudden onset heart failure in a previously healthy young person, chest pain mimicking MI, arrhythmias
- Diagnosis: cardiac MRI (late gadolinium enhancement) + endomyocardial biopsy
- Dallas criteria (biopsy): myocyte necrosis + adjacent inflammatory infiltrate
Summary Table
| Category | Hallmark Pathology | Key Feature |
|---|---|---|
| Ischemic / MI | Coagulation necrosis → scar | Pale/yellow area on TTC stain |
| Hypertensive | LV concentric hypertrophy | Boxcar nuclei, wall >2 cm |
| Valvular (calcific) | Calcium in cusps/annulus | Aortic > mitral; commissures not fused |
| Valvular (rheumatic) | Aschoff bodies, commissural fusion | "Fish-mouth" mitral orifice |
| DCM | 4-chamber dilation, interstitial fibrosis | Systolic dysfunction |
| HCM | Asymmetric septal hypertrophy, myocyte disarray | #1 cause SCD in young athletes |
| Restrictive | Stiff ventricle, atrial dilation | Amyloidosis most common cause |
| TOF | VSD + PS + overriding aorta + RVH | Cyanosis, tet spells, boot-shaped heart |
| Myocarditis | Myocyte necrosis + inflammation | Coxsackie B virus most common |
Sources: Robbins & Kumar Basic Pathology (9780323790185) and Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
This is a shared conversation. Sign in to Orris to start your own chat.