Explore bucket handle fracture in pediatrics
Reading File
Finding Sources
Searching PubMed
"bucket handle fracture" AND pediatric
Searching Images
bucket handle fracture pediatric child abuse metaphyseal
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
I have rich content from multiple authoritative textbooks and excellent radiograph images. Let me now compile the comprehensive answer.
Bucket Handle Fracture in Pediatrics
What Is It?
A bucket handle fracture is a radiographic appearance of a Classic Metaphyseal Lesion (CML) — a shear injury to the immature metaphysis of a growing bone in infants. The term describes a specific projection: when the thin avulsed disc of bone is viewed end-on (AP view), its thicker peripheral rim creates the curved silhouette of a bucket handle. It is among the most specific radiologic indicators of non-accidental trauma (NAT) / child physical abuse.
Anatomy & Pathomechanism
The injury occurs through the primary spongiosa — the immature, weakest zone of the metaphysis just beneath the growth plate (physis). This zone is poorly mineralized and highly susceptible to shearing forces.
Mechanism: Violent shaking, yanking, or twisting of the infant's limb generates rapid acceleration-deceleration forces. The inertia of the relatively heavy epiphysis creates torsional and shearing stress at the metaphyseal-physeal junction. This propagates a planar fracture through the primary spongiosa across the full width (or part) of the metaphysis, separating a thin disc or wafer of bone.
"The injury is a result of shearing forces sustained during violent shaking or handling of the infant, outside those forces associated with daily care." — Grainger & Allison's Diagnostic Radiology
Radiographic Appearances
The CML has three projections depending on X-ray angle:
| Appearance | Description |
|---|---|
| Bucket handle fracture | AP view — thin wafer thicker at the periphery; curved "handle" |
| Corner fracture | Tangential view — only the thick peripheral rim is seen as a corner chip |
| Thin disc with thick rim | Full planar view — disc with dense peripheral margin |
These are the same lesion seen at different angles, not distinct injury types.
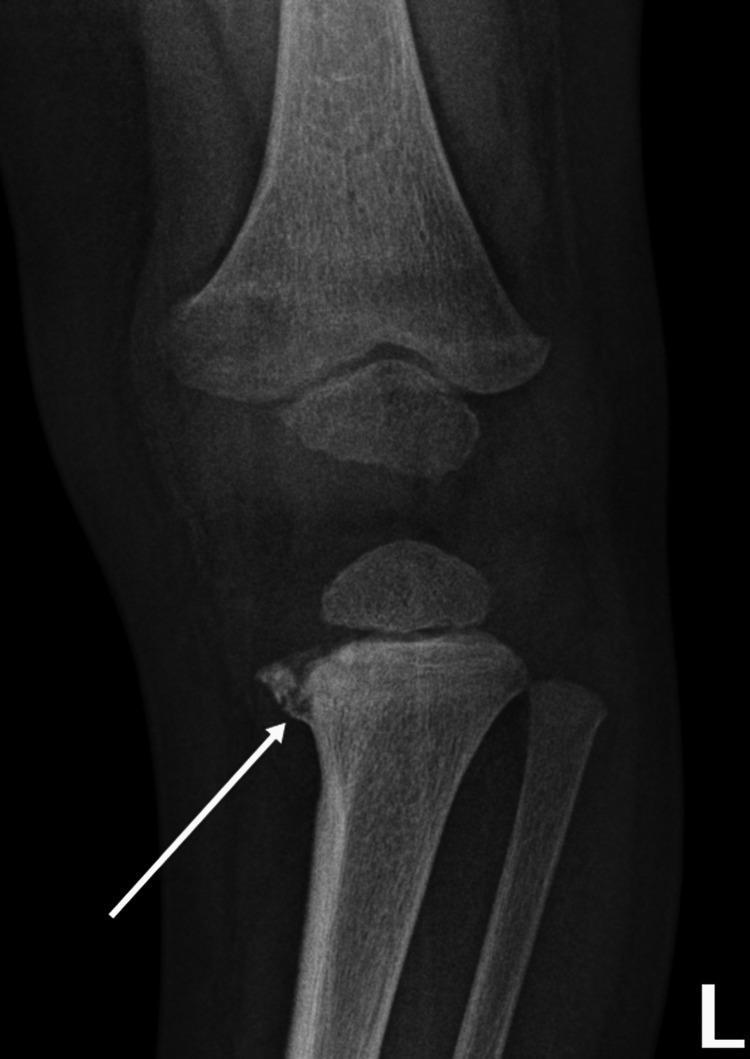
AP radiograph: curvilinear lucent line at the proximal tibial metaphysis — classic bucket handle fracture (CML)
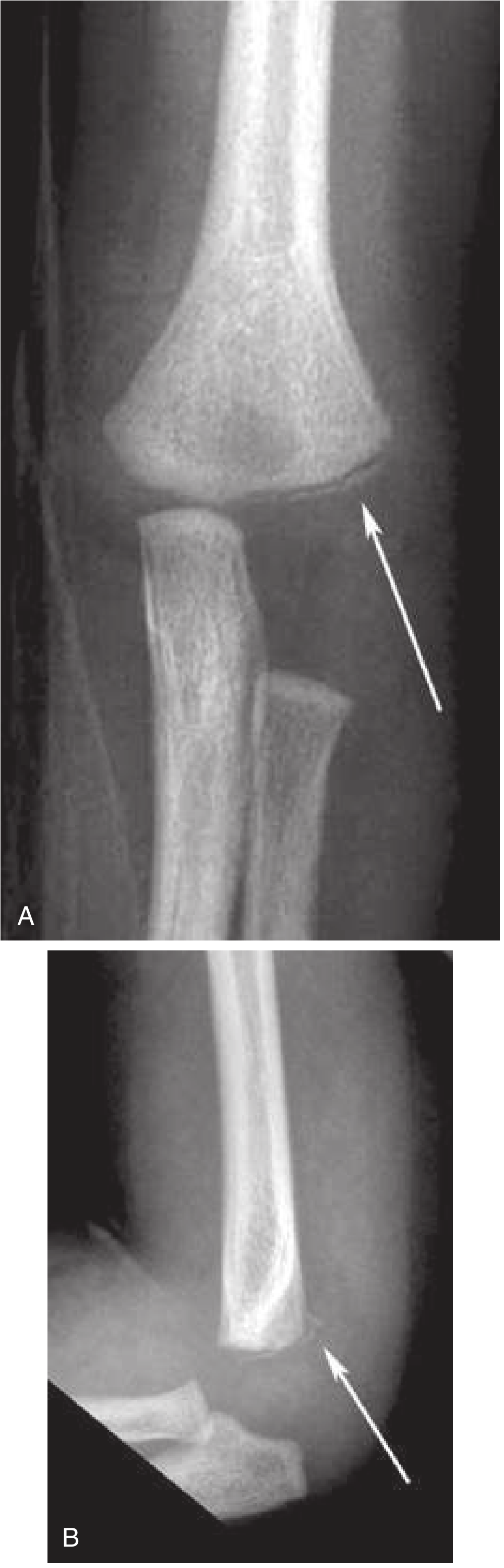
From Rosen's Emergency Medicine: (A) AP view — bucket handle conformation; (B) lateral view — same fracture appears as a "chip"
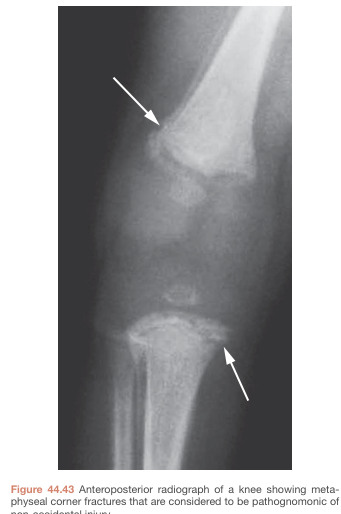
Bailey & Love's: Bilateral metaphyseal corner fractures at the distal femur and proximal tibia — pathognomonic for NAI
Epidemiology
- Seen in high proportions of physically abused infants, most commonly non-mobile infants < 12 months
- Most frequently affect the distal femur, proximal and distal tibia, and proximal humerus; also occur at the elbow and wrist
- May be unilateral or bilateral
- Typically asymptomatic and clinically silent — identified only on skeletal survey imaging
Clinical Significance
"No fracture is more specific for abuse than the CML, and identification should prompt a thorough evaluation for other injuries." — Rosen's Emergency Medicine
CMLs are considered highly specific (though not absolutely pathognomonic in isolation) for physical abuse. Their presence mandates:
- Full skeletal survey (head-to-toe radiographs)
- Neurology evaluation (for abusive head trauma / retinal hemorrhage)
- Child protection team involvement
- Mandatory reporting to child protective services
Associated Injuries (Non-Accidental Trauma Constellation)
Bucket handle fractures rarely occur in isolation. Co-existing injuries include:
- Posterior rib fractures (near costovertebral junction) — highly specific for abuse
- Subdural hematoma (bridging vein tears from acceleration-deceleration)
- Retinal hemorrhages (in up to 80% of abusive head trauma)
- Long bone fractures of different ages
- Spiral femur fractures in non-ambulatory infants
- Bruising in non-ambulatory or pre-mobile infants
- Spine, scapula, sternum, and pelvic fractures in non-ambulant children
Healing Pattern & Fracture Dating
- CMLs typically heal without callus formation via gradual bone consolidation over 4–8 weeks
- When the periosteum is stripped by shearing forces, subperiosteal hemorrhage occurs → periosteal reaction develops during healing
- Fracture dating by periosteal response:
| Stage | Time (days) |
|---|---|
| Appearance of subperiosteal new bone formation | 4–10 (early) → 10–14 (peak) |
| Loss of fracture line definition (soft callus) | 10–14 (early) → 14–21 (peak) |
| Hard callus (lamellar bone formation) | 14–21 (early) → 21–42 (peak) |
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Normal growth variants | Subtle metaphyseal step-off or "collar" without injury history |
| Physiological periosteal reaction | Bilateral, symmetric, confined to diaphysis; ages 1–4 months (up to 35% of normal infants) |
| Rickets | Diffuse cupping/fraying of metaphysis; low vitamin D/phosphate; responds to supplementation |
| Osteogenesis imperfecta | Blue sclerae, family history, diffuse osteopenia, wormian bones |
| Renal osteodystrophy | Chronic renal disease history, diffuse osseous changes |
| Toddler's fracture | Ambulatory child (9 months – 4 years), distal tibia spiral fracture, plausible mechanism (twist/fall) |
Early weight-bearing in bow-legged children (>15 months) can cause metaphyseal fragmentation that mimics CML — clinical correlation is essential.
Imaging Approach
Skeletal Survey (Standard of Care)
A complete skeletal survey includes:
- AP skull + lateral skull
- AP chest (ribs)
- AP/lateral spine
- AP pelvis
- AP and lateral extremities (including hands and feet)
Oblique rib views improve sensitivity for posterior rib fractures. A follow-up survey at 2 weeks can reveal healing fractures missed on the initial study, significantly increasing detection.
Key X-ray Tips
- CMLs are subtle — look for faint curvilinear lucency at the metaphysis
- Multiple projections are critical — a bucket handle on AP may only be a "chip" on lateral
- Bone scan has limited utility; MRI can show periosteal edema in acute phase
Management & Disposition
CML itself does not require orthopedic intervention — it heals reliably without splinting. The primary management is child protection:
- Admit or place in protective custody pending full investigation
- Multidisciplinary team — pediatrics, child protection team, social work, ophthalmology, neurology/neurosurgery as indicated
- Skeletal survey + follow-up survey at 2 weeks
- Brain imaging (CT/MRI) in all infants with suspected abuse
- Ophthalmologic examination for retinal hemorrhage
- Lab work — CBC, coagulation studies (PT/PTT/INR), liver enzymes, amylase/lipase, UA; metabolic bone panel (Ca, Phos, ALP, vitamin D, PTH) to exclude metabolic causes
- Mandatory reporting per jurisdiction
Key Points Summary
| Feature | Detail |
|---|---|
| Mechanism | Shearing/torsional forces at metaphysis — violent shaking/yanking |
| Zone of injury | Primary spongiosa (immature metaphysis) |
| Classic age | < 12 months, non-mobile infants |
| Most common sites | Distal femur, tibia, proximal humerus |
| AP X-ray appearance | Curved peripheral rim — "bucket handle" |
| Lateral X-ray appearance | Small corner chip |
| Specificity for abuse | Highest among all fracture types |
| Healing | 4–8 weeks; no callus; periosteal reaction if periosteum stripped |
| Action required | Full skeletal survey, child protection workup, mandatory reporting |
Sources:
- Grainger & Allison's Diagnostic Radiology, Chapter 74 (Child Abuse Imaging)
- Rosen's Emergency Medicine, Chapter 172 (Sentinel Injuries / Physical Abuse)
- Tintinalli's Emergency Medicine, Chapter 150 (Physical Abuse in Children)
- Bailey & Love's Short Practice of Surgery, 28th Edition
Recent evidence: Karmazyn et al. (2022, AJR) — multicenter study on radiologists' performance in differentiating rickets from CMLs, highlighting that distinction can be challenging and requires specialist input [PMID: 35792137].
This is a shared conversation. Sign in to Orris to start your own chat.