How the function of health communication is organization but not community participation?
functions of health communication organization vs community participation
health communication function "organization" NOT "community participation" public health definition
Functions of Health Communication: Why "Organization" Is a Function but "Community Participation" Is Not
- Information
- Education
- Motivation
- Persuasion
- Counselling
- Raising morale
- Health development
- Organization
The Function of Organization (Function #8)
"Communication is the life and blood of an organization."
- Vertical communication - flows downward (from top administrators through the hierarchy of professionals and non-professionals, down to beneficiaries/employees) and upward (feedback from the field to management).
- Horizontal (cross) communication - takes place between equals at any level within an organization.
- Coordinating health teams internally (e.g., hospital departments communicating policies)
- Enabling inter-sectoral coordination (e.g., the health ministry communicating with education or agriculture ministries)
- Ensuring administrators and frontline workers stay aligned
- Maintaining the structural flow of health services
Why "Community Participation" Is NOT Listed as a Function of Health Communication
-
Conceptual difference: Communication functions describe what communication does internally to systems and people (it informs, educates, motivates, persuades, organizes). Community participation describes what communities do in response - it is an outcome or a process in its own right, not an activity of communication.
-
Direction of action: Communication functions are acts performed by health communicators or health systems. Community participation is an act performed by the community - it is a response, not a transmission.
-
Scope: Health communication can support community participation (e.g., by raising awareness, motivating action), but participation itself involves governance, empowerment, decision-making, and collective action that go far beyond the communicative act alone.
-
Classification in public health: Community participation is classified under primary health care principles (as laid out in the Alma-Ata Declaration, 1978) and under health promotion strategies (Ottawa Charter, 1986). It is not a sub-function of communication.
How the Two Relate (Without Being Equivalent)
| Aspect | Organization (Function of Health Communication) | Community Participation |
|---|---|---|
| Who acts | Health organizations, administrators, professionals | Community members, the public |
| What it does | Coordinates institutions; ensures internal/external information flow | Engages the public as active co-creators of health solutions |
| Direction | Top-down and lateral within systems | Bottom-up; community-driven |
| Listed in Park's functions | Yes (Function #8) | No |
| Role in health | Structural coordination | Empowerment and ownership |
- Park's Textbook of Preventive and Social Medicine, Functions of Health Communication, p. 961
What is the conceptual difference between a restrictive and obstructive lung disease?
restrictive vs obstructive lung disease conceptual difference pathophysiology spirometry
Restrictive vs. Obstructive Lung Disease: The Conceptual Difference
The Core Concept
"Diffuse pulmonary diseases can be classified into two categories: (1) obstructive (airway) disease, characterized by an increase in resistance to airflow caused by partial or complete obstruction at any level; and (2) restrictive disease, marked by reduced expansion of lung parenchyma, and decreased total lung capacity."
- Robbins & Kumar Basic Pathology
| Obstructive | Restrictive | |
|---|---|---|
| Core problem | Cannot empty the lungs (airflow out is blocked) | Cannot fill the lungs (expansion is limited) |
| Mechanical defect | Increased airway resistance | Reduced lung/chest wall compliance |
| What is reduced | Airflow rate (FEV1) | Lung volume (FVC, TLC) |
| FEV1/FVC ratio | Decreased (< 0.70) | Normal or increased (≥ 0.70) |
Obstructive Lung Disease
- FEV1 is markedly reduced (the patient blows air out slowly)
- FVC is normal or only slightly reduced
- The FEV1/FVC ratio is therefore low (< 0.70)
- Air trapping occurs, so Total Lung Capacity (TLC) is normal or increased
- The spirometry curve shows a slow, prolonged, flattened expiratory slope
- Airway narrowing - as in asthma (bronchoconstriction) or chronic bronchitis (mucosal thickening)
- Loss of elastic recoil - as in emphysema, where destruction of alveolar walls means the airways collapse during expiration
Restrictive Lung Disease
- FVC is reduced (the lung cannot hold a normal volume)
- FEV1 is reduced proportionally
- The FEV1/FVC ratio is normal or elevated (air moves out quickly from a smaller lung)
- TLC is reduced (the hallmark finding)
- Intrinsic (parenchymal) - the lung itself is stiff: pulmonary fibrosis, pneumoconiosis, sarcoidosis, ARDS
- Extrinsic (extrapulmonary) - something outside the lung restricts its movement: severe obesity, kyphoscoliosis, neuromuscular disease (Guillain-Barré), pleural effusion, pregnancy, ascites, ankylosing spondylitis
The Spirometry Picture
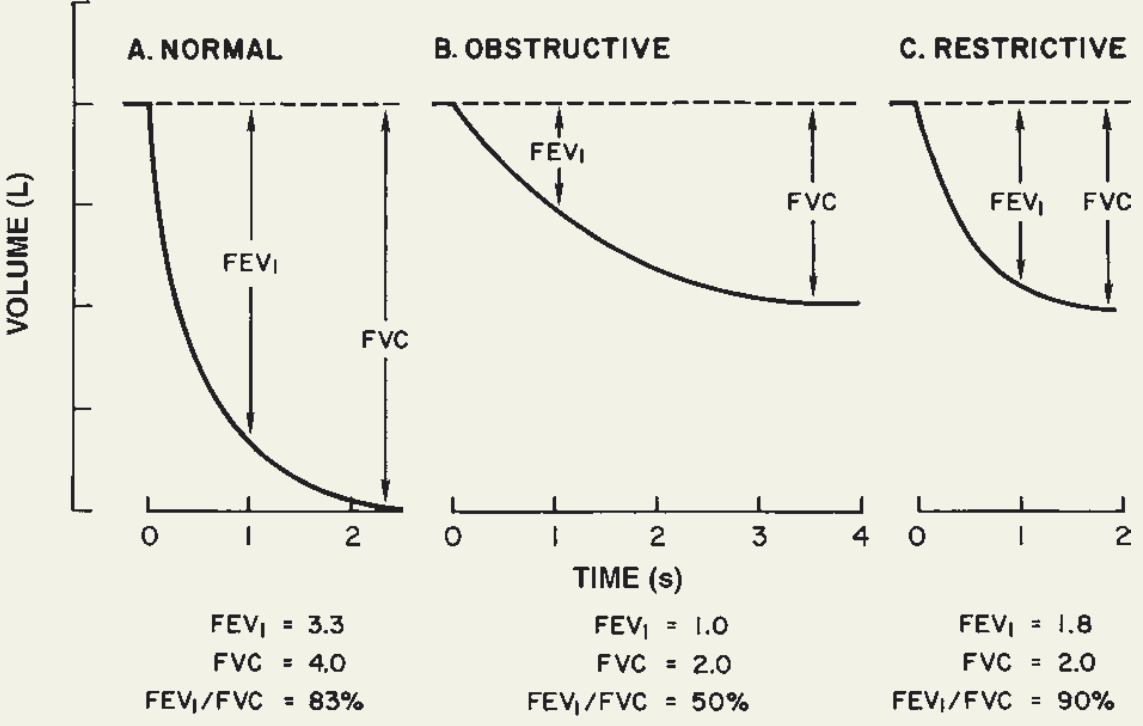
- Normal: FEV1 = 3.3 L, FVC = 4.0 L, FEV1/FVC = 83%
- Obstructive: FEV1 = 1.0 L, FVC = 2.0 L, FEV1/FVC = 50% - the curve is flat and prolonged; the patient takes >4 seconds to empty what little they can
- Restrictive: FEV1 = 1.8 L, FVC = 2.0 L, FEV1/FVC = 90% - the curve is steep and short; the patient empties quickly but there is simply less total air to expel
Why the Distinction Matters Clinically
| Clinical point | Obstructive | Restrictive |
|---|---|---|
| Confirm with | Spirometry (FEV1/FVC ratio) | Lung volume measurement (TLC by plethysmography) |
| Reversibility test | Bronchodilator response (asthma) | Not applicable |
| DLCO | Low in emphysema; normal in asthma | Low in ILD; normal in extrapulmonary causes |
| Treatment target | Bronchodilators, anti-inflammatory | Treat underlying cause; antifibrotics for IPF |
- Robbins & Kumar Basic Pathology, Obstructive and Restrictive Pulmonary Diseases, p. 447
- Ganong's Review of Medical Physiology, Airflow Measurements of Obstructive & Restrictive Disease
- Miller's Anesthesia, Restrictive Lung Disease, p. 4179
How does 2% propionic acid spray helps in prevention of baggosis?
propionic acid spray 2% bagassosis prevention sugarcane bagasse thermophilic actinomycetes
2% Propionic Acid Spray in the Prevention of Bagassosis
What is Bagassosis?
How Propionic Acid Prevents Bagassosis
- Lowers the pH of the bagasse surface, creating an acidic environment hostile to Thermoactinomyces sacchari and other thermophilic actinomycetes and moulds
- Inhibits microbial growth and sporulation - the organisms cannot multiply or produce the spores that become airborne and pathogenic
- Prevents decomposition and heating of the stored bagasse - thermophilic actinomycetes require warmth and fermentation to proliferate; propionic acid halts this process
- Reduces antigen load - by killing the organisms in the stored material, the total burden of inhaled antigen is dramatically reduced or eliminated
"By keeping the moisture content above 20 per cent and spraying the bagasse with 2 per cent propionic acid, a widely used fungicide, bagasse can be rendered safe for manufacturing use."
Why Moisture Control Accompanies It
- Moisture above 20% prevents the dry, dusty conditions that allow spores to become airborne when bagasse is handled
- Propionic acid kills the organisms already present in the stored material
Place of Propionic Acid in the Full Prevention Strategy
| # | Category | Measures |
|---|---|---|
| 1 | Dust control | Wet process, enclosed apparatus, exhaust ventilation |
| 2 | Personal protection | Masks/respirators with mechanical filters or air supply |
| 3 | Medical control | Pre-employment and periodic medical check-ups |
| 4 | Bagasse control | Moisture >20% + 2% propionic acid spray |
- Park's Textbook of Preventive and Social Medicine, Bagassosis (Preventive Measures), p. 4708

Explain the 3 leverages for children
Factories Act India "leverages for children" child workers night shift leave hours provisions
3 Leverages for Children Under the Factories Act, 1948
1. No Night Duties
2. 1 Extra Leave Every 14 Days
3. Maximum 4½ Hours Per Day
- Limits physical and mental strain
- Allows time for schooling and education
- Prevents exploitation through excessive working hours
- Aligns with the Constitutional spirit of Article 39 (right to education and protection from hazardous work)
Constitutional Backing (from your notes)
| Article | Provision |
|---|---|
| Article 34 (likely Article 24) | No employment of children under 14 years - child's right |
| Article 39 | Children of tender age (15-19 yrs) must be given adequate and applicable work; no hazardous work; free and compulsory education for all |
Summary Table
| Leverage | Protection Given | Purpose |
|---|---|---|
| No night duties | No work during night hours | Prevent physiological harm and safety risks |
| 1 extra leave/14 days | Additional rest days | Adequate recovery and wellbeing |
| 4½ hr/day max | Shorter working hours than adults | Prevent overwork; allow time for education |

Explain this in direct benefits of esic
ESIC direct benefits list sickness maternity disablement dependent death funeral India ESI Act
https://www.novabenefits.com/blog/esic-employees-state-insur…
ESIC direct benefits table "sickness benefit" "maternity benefit" "disablement" "dependent benefit" "funeral" wage percentage days
https://roap.esic.gov.in/ro-sro-information-benefits
https://desicalculator.com/indian-finance/esic-benefits-calc…
ESIC Direct Benefits
1. Sickness Benefit (SB)
| Disease/Event | Any type of illness preventing work |
| Cash paid | 70% of average daily wages |
| Duration | Up to 91 days in two consecutive benefit periods per year |
| Extended SB | 80% of wages for up to 2 years for specified long-term illnesses (e.g., TB, cancer, mental illness) |
| Eligibility | Must have contributed for at least 78 days in the preceding contribution period |
2. Maternity Benefit (MB)
| Disease/Event | Confinement (childbirth), miscarriage, or adoption |
| Cash paid | 100% of average daily wages |
| Duration | 26 weeks (182 days) for childbirth; 6 weeks for miscarriage; 12 weeks for adoption |
| Additional | Medical bonus also provided |
3. Disablement Benefit
| Disease/Event | Employment injury or occupational disease causing disability |
| Temporary disablement | 90% of daily wages - paid until recovery, no time limit |
| Permanent disablement | Lifelong monthly pension based on certified percentage loss of earning capacity (up to 90%) |
| No minimum contribution required - benefit starts from Day 1 of employment |
4. Dependants' Benefit (DB)
| Disease/Event | Death of insured person due to employment injury |
| Cash paid | 90% of daily wages as monthly pension, shared among dependants |
| Who gets it | Widow (3/5 share), children (2/5 share), parents (if no widow/children) |
| Duration | Widow - lifelong (or until remarriage); children - until age 18 |
5. Funeral Expenses
| Disease/Event | Death of the insured person (any cause) |
| Cash paid | Lump sum of ₹15,000 (paid to eldest surviving family member or person who performs the funeral) |
| Purpose | One-time reimbursement to cover funeral costs |
6. Unemployment Allowance (Rajiv Gandhi Shramik Kalyan Yojana)
| Disease/Event | Involuntary loss of job (factory closure, retrenchment) |
| Cash paid | 50% of wages |
| Duration | Up to 2 years |
Summary Table (Direct Benefits at a Glance)
| Benefit | Event/Disease | Cash Amount | Duration |
|---|---|---|---|
| Sickness Benefit | Any illness | 70% of wages | 91 days/year |
| Extended Sickness | Long-term illness | 80% of wages | Up to 2 years |
| Maternity Benefit | Childbirth | 100% of wages | 26 weeks |
| Temporary Disablement | Work injury | 90% of wages | Until recovery |
| Permanent Disablement | Work injury (permanent) | Up to 90% of wages | Lifelong pension |
| Dependants' Benefit | Death from work injury | 90% of wages | Lifelong (dependants) |
| Funeral Expenses | Death (any cause) | ₹15,000 lump sum | One-time |
Contrast with Indirect Benefit (from your image)
| Direct Benefit | Indirect Benefit | |
|---|---|---|
| Form | Cash payment to employee | Service provision |
| Example | Sickness cash allowance | Empanelled hospital treatment |
| Who pays | ESIC pays employee | ESIC pays the private hospital |
| Received by | Employee directly | Employee uses hospital; govt pays hospital |