Hypersensitivity* Reactions - define*; classify, discuss; Type I Hypersensitivity Reactions - discuss 2. Amyloid***** - define, classify*, molecular structure, special stains***; physiochemical properties 3. Sago Spleen; Amyloidosis of Spleen - gross, microscopic features 4. Autoimmune Disorders - mechanisms 5. Neoplasms found in patients with HIV infection 1. Autoimmunity - define, pathogenesis 2. AIDS - etiology, routes of transmission, natural history (phases), diagnosis answer in detail covering imp points as welll in exaam point of view 2mbbs pathology refer robbin harsh moham add diagrams as well cover required points for muhs exam Add histo pathology diagram and gross as well for exam easy to draw diagram
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is your comprehensive 2nd MBBS Pathology notes for MUHS exam, based on Robbins/Cotran Pathologic Basis of Disease, Harsh Mohan, and Jawetz Microbiology:
2nd MBBS PATHOLOGY - MUHS EXAM NOTES
TOPIC 1: HYPERSENSITIVITY REACTIONS
Definition
Hypersensitivity is a condition in which an exaggerated or augmented immune response occurs that is harmful to the host. It requires a presensitized state - reactions typically occur after the second encounter with a specific antigen (allergen).
Robbins: "Hypersensitivity refers to the tissue-damaging immune reactions that may be elicited by exogenous environmental antigens or by endogenous self-antigens."
Classification (Gell & Coombs, 1963)
| Type | Name | Mechanism | Mediators | Time | Examples |
|---|---|---|---|---|---|
| I | Immediate / Anaphylactic | IgE-mediated | Mast cells, basophils, histamine | Seconds-minutes | Anaphylaxis, asthma, hay fever, urticaria |
| II | Cytotoxic / Antibody-dependent | IgG/IgM against cell surface | Complement, ADCC | Hours | Hemolytic anemia, Goodpasture syndrome, ABO incompatibility |
| III | Immune complex-mediated | Antigen-antibody complexes | Complement, PMNs | Hours | SLE, serum sickness, post-strep GN |
| IV | Delayed / Cell-mediated | T lymphocytes | Cytokines, macrophages | 24-72 hrs | TB (tuberculin test), contact dermatitis, graft rejection |
TYPE I HYPERSENSITIVITY (IMMEDIATE) - Detailed
Definition
Type I hypersensitivity manifests in tissue reactions occurring within seconds after antigen combines with specific IgE antibody. Also called immediate hypersensitivity or allergy/atopy.
Mechanism (Step-by-Step)
┌─────────────────────────────────────────────────────────────────┐
│ TYPE I HYPERSENSITIVITY - MECHANISM │
│ │
│ SENSITIZATION PHASE (1st Exposure) │
│ Antigen (allergen) → B cell → Plasma cell │
│ → IgE production │
│ → IgE binds to Fc-ε-RI on MAST CELLS & BASOPHILS │
│ │
│ ELICITATION PHASE (2nd Exposure) │
│ Same antigen enters → Cross-links IgE on mast cells │
│ → DEGRANULATION │
│ → Release of PREFORMED & NEWLY FORMED mediators │
│ │
│ ┌─────────────────┐ ┌──────────────────────────────────┐ │
│ │PREFORMED (stored)│ │ NEWLY FORMED (synthesized) │ │
│ │- Histamine │ │ - Prostaglandins (PGD2) │ │
│ │- Heparin │ │ - Leukotrienes (LTC4, LTD4, LTE4)│ │
│ │- Eosinophil │ │ - Platelet activating factor │ │
│ │ chemotactic │ │ - Cytokines (IL-4, IL-5, TNF-α) │ │
│ │ factor (ECF) │ │ │ │
│ └─────────────────┘ └──────────────────────────────────┘ │
└─────────────────────────────────────────────────────────────────┘
Diagram (Easy to Draw in Exam)
1st EXPOSURE 2nd EXPOSURE
| |
[ALLERGEN] [ALLERGEN]
| |
[B cell] → IgE [IgE on mast cell]
| cross-linked
IgE binds to |
mast cell Fc-ε-RI DEGRANULATION
(sensitization) |
┌──────┴──────┐
EARLY LATE
(mins) (hrs)
| |
Histamine Leukotrienes
Edema Prostaglandins
Bronchospasm Cytokines
Vasodilation Tissue damage
Mediators of Type I Hypersensitivity
PRIMARY (Preformed - released immediately):
- Histamine - vasodilation, increased capillary permeability, bronchospasm
- Heparin - anticoagulant effect
- Eosinophil chemotactic factor (ECF) - attracts eosinophils
- Proteases - tissue damage
SECONDARY (Newly formed - synthesized after activation):
- Prostaglandins (PGD2) - bronchoconstriction, vasodilation
- Leukotrienes LTC4, LTD4, LTE4 (SRS-A = Slow Reacting Substance of Anaphylaxis) - potent bronchoconstriction, increased vascular permeability
- Leukotriene B4 (LTB4) - chemotaxis of leukocytes
- Platelet Activating Factor (PAF) - activates platelets, causes bronchoconstriction
- Cytokines: IL-4, IL-5, IL-13, TNF-α
Clinical Manifestations of Type I
| Form | Features |
|---|---|
| Systemic Anaphylaxis | Life-threatening; urticaria, bronchospasm, laryngeal edema, hypotension, shock; triggered by drugs (penicillin), bee stings, food (peanuts) |
| Atopy (Local) | Genetic predisposition; elevated IgE; hay fever, asthma, eczema, urticaria |
| Bronchial Asthma | Bronchospasm, wheezing, eosinophilia |
| Allergic Rhinitis | Hay fever, sneezing, watery discharge |
| Food Allergy | Nausea, vomiting, diarrhea |
Types II, III, IV (Brief for Completeness)
TYPE II - Cytotoxic:
- Antibodies (IgG/IgM) directed against cell surface antigens
- Mechanisms: Complement lysis, ADCC (antibody-dependent cellular cytotoxicity), opsonization
- Examples: Transfusion reactions (ABO), Rh hemolytic disease of newborn, Goodpasture syndrome (anti-GBM), Graves' disease, Myasthenia gravis
TYPE III - Immune Complex:
- Antigen-antibody complexes deposited in tissues → activate complement → PMN recruitment → tissue damage
- Examples: SLE, serum sickness, post-streptococcal GN, Arthus reaction
- Key: Complement consumption → hypocomplementemia during acute phase
TYPE IV - Delayed (Cell-Mediated):
- T lymphocytes sensitized by antigen; release cytokines on second contact
- CD4+ Th1 cells → activate macrophages (granuloma formation)
- CD8+ CTLs → direct cytotoxicity
- Examples: Tuberculin (Mantoux) test, contact dermatitis (poison ivy), graft rejection, granulomatous diseases (TB, sarcoidosis)
TOPIC 2: AMYLOID - DEFINITION, CLASSIFICATION, STRUCTURE, STAINS
Definition
Amyloid is an extracellular deposit of abnormal, misfolded proteins that aggregate into insoluble fibrils, which accumulate in tissues and cause organ dysfunction by pressure atrophy and disruption of tissue architecture.
Robbins: "Amyloidosis results from abnormal folding of proteins, which become insoluble, aggregate, and deposit as fibrils in extracellular tissues."
Molecular Structure
┌────────────────────────────────────────────────────────┐
│ MOLECULAR STRUCTURE OF AMYLOID │
│ │
│ Misfolded protein → β-sheet configuration │
│ ↓ │
│ Monomers self-assemble │
│ ↓ │
│ AMYLOID FIBRIL │
│ - Non-branching fibrils, 7.5-10 nm diameter │
│ - Antiparallel β-pleated sheet configuration │
│ - Cross β-sheet structure (perpendicular to fibril │
│ axis) = gives apple-green birefringence │
│ ↓ │
│ + Serum Amyloid P component (SAP) - all amyloids │
│ + Glycosaminoglycans (heparan sulfate) │
│ + Apolipoprotein E │
└────────────────────────────────────────────────────────┘
Key structural features:
- Beta-pleated sheet (cross-β structure) - universal property
- Non-branching fibrils (7.5-10 nm wide, 30-100 nm long)
- All forms contain Serum Amyloid P (SAP) component and glycosaminoglycans
- The β-pleated sheet conformation is responsible for the characteristic optical property (apple-green birefringence)
Classification of Amyloidosis (Robbins Table 6.17)
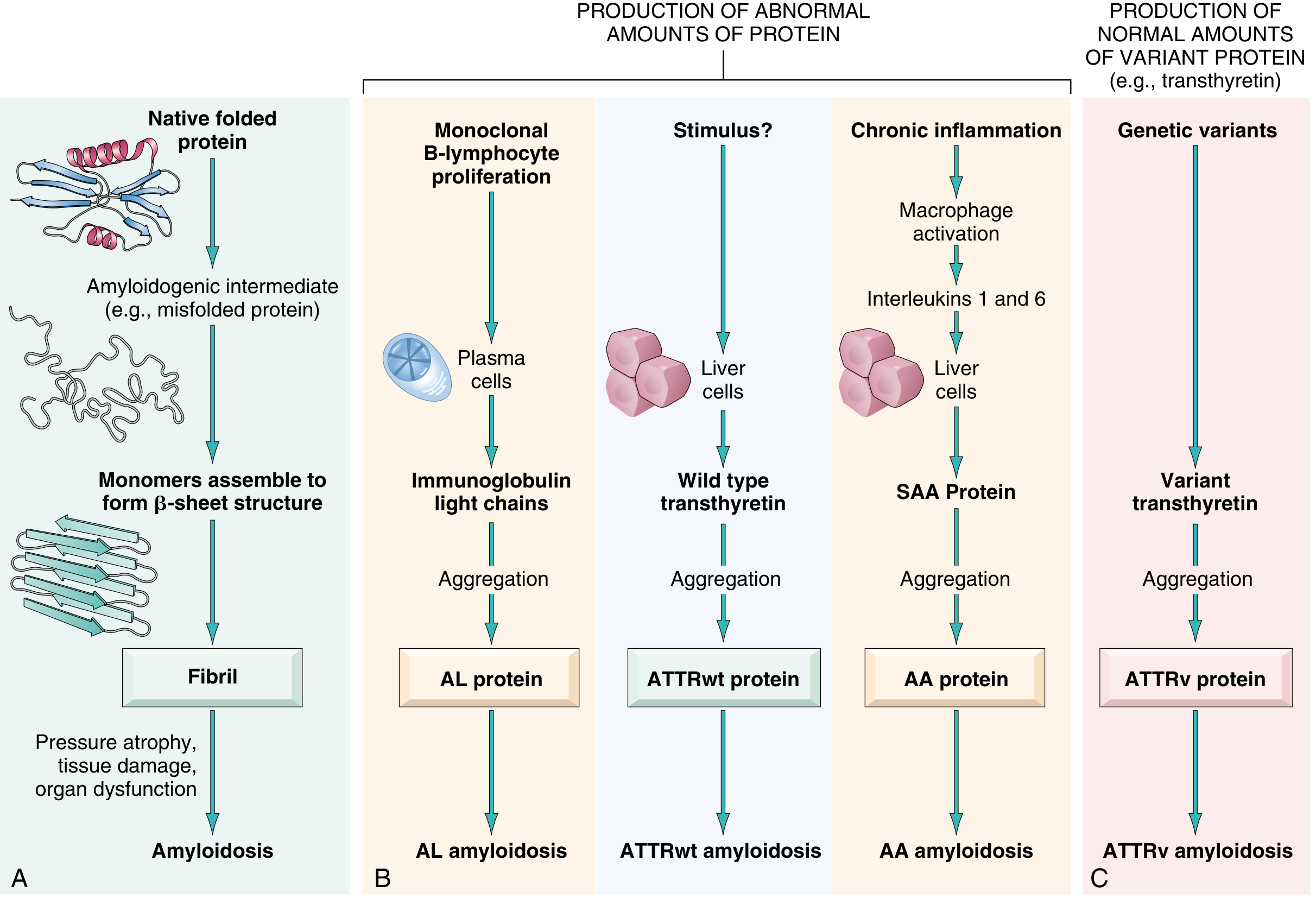
Fig. from Robbins: Pathogenesis of amyloidosis showing formation of amyloid fibrils and their types
A. Based on Distribution
| Type | Description |
|---|---|
| Systemic (Generalized) | Affects multiple organs |
| Localized | Limited to single organ/tissue |
B. Based on Biochemical Nature (Current Classification)
| Amyloid Type | Fibril Protein | Precursor | Clinical Setting |
|---|---|---|---|
| AL (Amyloid Light chain) | Ig light chains (λ > κ) | Plasma cell (monoclonal) | Multiple myeloma, plasma cell dyscrasias - MOST COMMON |
| AA (Amyloid Associated) | Serum Amyloid A (SAA) | SAA protein (acute phase reactant) | Secondary/reactive amyloidosis - chronic inflammations (TB, RA, osteomyelitis, FMF) |
| ATTRwt | Wild-type transthyretin | Normal transthyretin (liver) | Old age - "senile systemic amyloidosis"; cardiac involvement |
| ATTRv | Variant transthyretin | Mutant transthyretin | Familial amyloid polyneuropathy (autosomal dominant) |
| Aβ2M | β2-microglobulin | β2-microglobulin | Hemodialysis-associated amyloidosis |
| Aβ | Aβ peptide (derived from APP) | Amyloid precursor protein | Alzheimer's disease (brain plaques) |
C. Old/Traditional Classification
| Type | Description |
|---|---|
| Primary | No predisposing disease; associated with plasma cell disorders; AL type |
| Secondary (Reactive) | Associated with chronic inflammatory disease; AA type |
| Heredofamilial | ATTRv - familial Mediterranean fever, familial amyloid polyneuropathy |
| Localized | Single organ; lung, skin, tongue, bladder |
| Endocrine | Medullary thyroid carcinoma (calcitonin precursor), type 2 DM (IAPP), pheochromocytoma |
| Senile | ATTRwt; heart predominantly; old age |
| Hemodialysis-associated | β2-microglobulin; carpal tunnel syndrome |
Special Stains for Amyloid ⭐⭐⭐ (HIGH YIELD)
┌──────────────────────────────────────────────────────────────────┐
│ SPECIAL STAINS FOR AMYLOID │
│ │
│ 1. CONGO RED (Most specific, routinely used) │
│ - Normal light: SALMON PINK / ORANGE-RED color │
│ - Polarized light: APPLE-GREEN BIREFRINGENCE ★★★ │
│ (pathognomonic for amyloid) │
│ │
│ 2. CRYSTAL VIOLET (Metachromatic stain) │
│ - Amyloid appears PURPLE/ROSE color │
│ - Normal color of crystal violet = purple │
│ - Metachromasia = color change │
│ │
│ 3. THIOFLAVIN T (Fluorescent stain) │
│ - Yellow-green FLUORESCENCE under UV light │
│ - Very sensitive but less specific │
│ │
│ 4. PAS STAIN │
│ - Weakly positive (pale pink) │
│ - Diastase resistant │
│ │
│ 5. SIRIUS RED - Can also detect amyloid │
└──────────────────────────────────────────────────────────────────┘
Mnemonic for Congo Red appearance: "Salmon in the Sun turns Apple Green in the Dark"
- Normal light → salmon/orange-red
- Polarized light → apple-green birefringence
Physicochemical Properties of Amyloid
| Property | Details |
|---|---|
| Solubility | Insoluble in physiologic solvents |
| Structure | Non-branching fibrils, 7.5-10 nm diameter |
| Configuration | Antiparallel β-pleated sheets |
| Staining | Congo red positive with apple-green birefringence |
| X-ray diffraction | Cross-β diffraction pattern (4.7 Å and 10 Å reflections) |
| Electron microscopy | Non-branching fibrils |
| Components | Fibrils + SAP (serum amyloid P) + glycosaminoglycans + Apo-E |
| Resistance | Resistant to proteolysis |
TOPIC 3: SAGO SPLEEN / AMYLOIDOSIS OF SPLEEN
Gross Features (Two Patterns)
┌──────────────────────────────────────────────────────────────────┐
│ AMYLOIDOSIS OF SPLEEN - GROSS │
│ │
│ PATTERN 1: SAGO SPLEEN │
│ ──────────────────────── │
│ - Amyloid deposits in WHITE PULP (splenic follicles) │
│ - Gross: Small translucent, pale gray, waxy nodules │
│ resembling "TAPIOCA/SAGO GRAINS" │
│ - The follicles look like boiled sago seeds │
│ - Spleen may be normal or slightly enlarged │
│ │
│ PATTERN 2: LARDACEOUS SPLEEN (Bacon/Ham Spleen) │
│ ────────────────────────── │
│ - Amyloid deposits in RED PULP (sinuses + connective tissue) │
│ - Gross: Uniform waxy, firm, homogeneous enlargement │
│ - Cut surface: resembles LARD (solidified fat/bacon) │
│ - Spleen markedly ENLARGED (splenomegaly) │
│ - Appears like "ham" or "bacon" → lardaceous │
│ │
│ ADVANCED: Combination of both patterns │
└──────────────────────────────────────────────────────────────────┘
Robbins: "In one, the deposits are largely limited to the splenic follicles, producing tapioca-like granules on gross inspection, designated sago spleen. In the other pattern, the amyloid involves the walls of the splenic sinuses and connective tissue framework in the red pulp..."
Easy Exam Diagram for Sago Spleen
SAGO SPLEEN LARDACEOUS SPLEEN
(White pulp affected) (Red pulp affected)
┌─────────────────────┐ ┌─────────────────────┐
│ Normal red pulp │ │ │
│ with WHITE nodules │ │ Uniform waxy │
│ (like white pearls │ │ enlarged spleen │
│ or sago grains) │ │ with lard-like │
│ ○ ○ ○ ○ ○ │ │ consistency │
│ ○ ○ ○ │ │ throughout │
│ ○ ○ ○ ○ ○ │ │ │
└─────────────────────┘ └─────────────────────┘
Small gray-white nodules Homogeneous, large,
(tapioca-like) on cross waxy spleen
section
Microscopic Features
┌──────────────────────────────────────────────────────────────────┐
│ AMYLOIDOSIS OF SPLEEN - MICROSCOPY │
│ │
│ H&E stain: │
│ - Amyloid appears as HOMOGENEOUS, EOSINOPHILIC (pink), │
│ AMORPHOUS extracellular material │
│ - Deposits replace normal splenic architecture │
│ - Follicles / sinuses replaced by acellular pink material │
│ - Pressure atrophy of surrounding cells │
│ │
│ Congo Red stain: │
│ - Deposits stain salmon-pink/orange-red │
│ - Under polarized light → APPLE-GREEN BIREFRINGENCE │
│ │
│ EM: │
│ - Non-branching fibrils in extracellular space │
└──────────────────────────────────────────────────────────────────┘
Histopathology description for exam:
- Under H&E: Homogeneous, structureless, eosinophilic (pink), amorphous material deposited in the extracellular spaces
- In sago spleen: deposits in and around the Malpighian corpuscles (white pulp/follicles)
- In lardaceous spleen: deposits in sinusoidal walls and red pulp stroma
- Congo red stain: salmon-pink color; apple-green birefringence under polarized light
TOPIC 4: AUTOIMMUNE DISORDERS - MECHANISMS / AUTOIMMUNITY
Definition
Autoimmunity is the failure of immunological tolerance to self antigens, resulting in immune reactions directed against the body's own tissues, causing tissue damage and organ dysfunction.
Normal Tolerance - Overview
Immunological tolerance = unresponsiveness to self antigens. Two mechanisms:
┌────────────────────────────────────────────────────────────────┐
│ MECHANISMS OF IMMUNOLOGICAL TOLERANCE │
│ │
│ 1. CENTRAL TOLERANCE │
│ - Occurs in THYMUS (T cells) and BONE MARROW (B cells) │
│ - Immature lymphocytes that strongly recognize SELF │
│ antigens → CLONAL DELETION (apoptosis) │
│ - B cells may undergo RECEPTOR EDITING to avoid │
│ self-reactivity │
│ │
│ 2. PERIPHERAL TOLERANCE │
│ - Mature lymphocytes in peripheral tissues │
│ - Mechanisms: │
│ a) ANERGY: T cells recognize self antigen without │
│ costimulation → become unresponsive │
│ b) REGULATORY T CELLS (Tregs): CD4+CD25+ T cells │
│ suppress self-reactive lymphocytes via IL-10, TGF-β │
│ c) ACTIVATION-INDUCED CELL DEATH (AICD): │
│ Fas-FasL interaction → apoptosis of activated cells │
│ d) INHIBITORY RECEPTORS: CTLA-4 and PD-1 on T cells │
│ deliver inhibitory signals │
└────────────────────────────────────────────────────────────────┘
Pathogenesis of Autoimmunity
Factors Leading to Breakdown of Tolerance:
1. Genetic Factors
- Strong association with HLA genes (particularly HLA-DR, HLA-DQ)
- HLA-DR3, DR4 → Type 1 DM, RA
- HLA-DR2 → SLE, MS, Goodpasture syndrome
- Non-HLA genes: PTPN22, CTLA4, NOD2 mutations
2. Infections (Environmental Triggers)
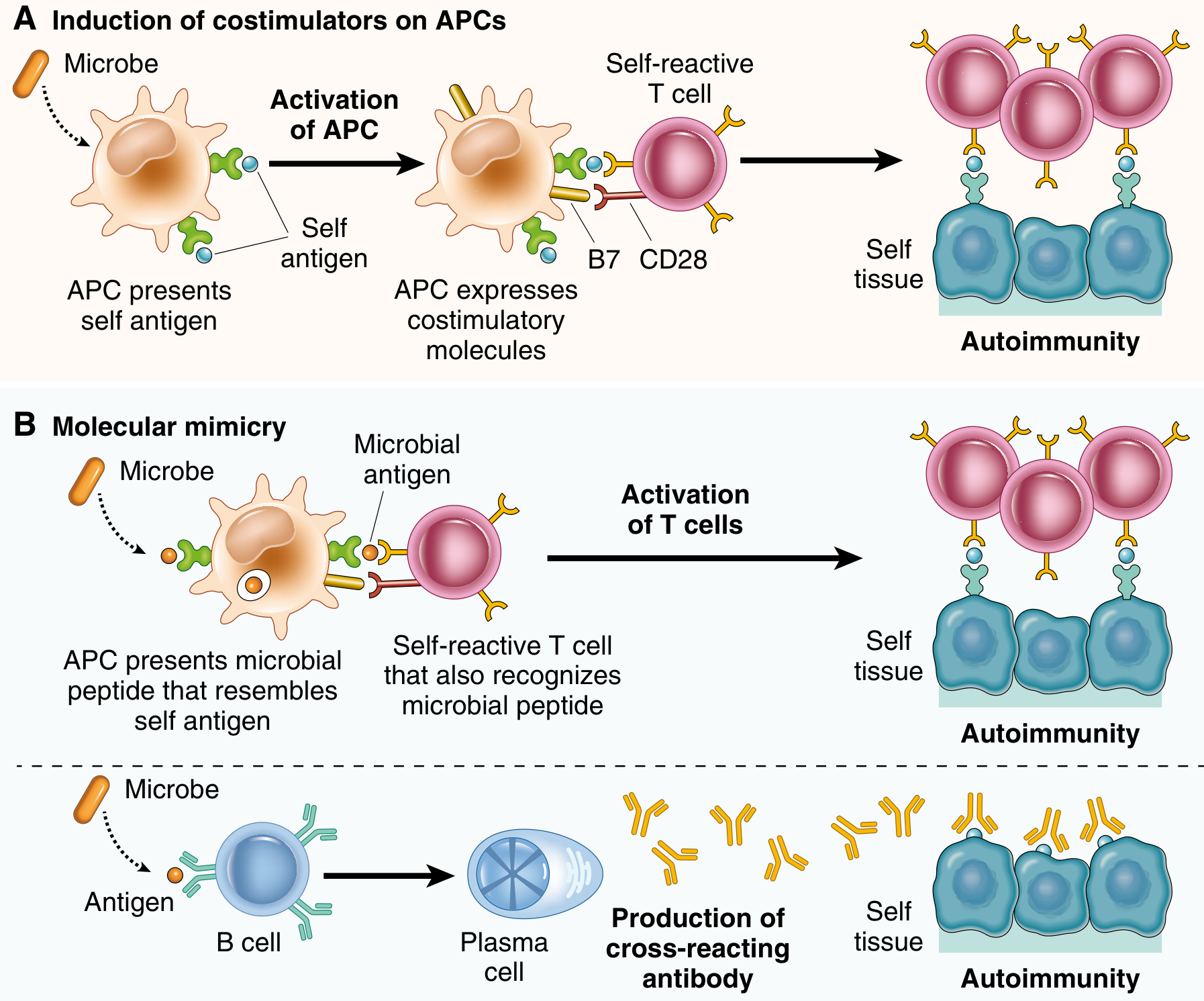
Fig. from Robbins: Role of infections in autoimmunity - (A) Induction of costimulators on APCs; (B) Molecular mimicry
Two key mechanisms by which infections trigger autoimmunity:
a) Induction of Costimulators on APCs:
- Microbes activate APCs → express B7 costimulatory molecules
- Self-reactive T cells (normally anergic) now receive both Signal 1 (antigen) AND Signal 2 (costimulation)
- Result: Self-reactive T cell activation → autoimmunity
b) Molecular Mimicry:
- Microbial antigens structurally resemble self antigens
- T/B cells activated against microbe cross-react with self antigens
- Example: Rheumatic fever - Streptococcal M protein mimics cardiac myosin → cardiac damage
3. Other Mechanisms
| Mechanism | Explanation |
|---|---|
| Release of sequestered antigens | Normally "hidden" antigens (lens, sperm, myelin) exposed after injury → autoimmune response |
| Polyclonal B-cell activation | Certain microbes (EBV, LPS) activate many B-cell clones nonspecifically including autoreactive ones |
| Epitope spreading | Immune response spreads from original antigen to other self epitopes in same tissue |
| Sex hormones | Autoimmune diseases more common in females; estrogen may promote antibody production |
| Regulatory T-cell defects | Defects in Tregs (FOXP3 mutations → IPEX syndrome) allow self-reactive lymphocytes to escape control |
Mechanisms of Tissue Damage in Autoimmune Disease
┌─────────────────────────────────────────────────────────────────┐
│ EFFECTOR MECHANISMS OF AUTOIMMUNE TISSUE DAMAGE │
│ │
│ 1. AUTOANTIBODIES (Humoural) │
│ a) Direct cell damage: Anti-RBC (hemolytic anemia) │
│ Anti-platelet (ITP) │
│ b) Complement activation: Anti-GBM (Goodpasture's) │
│ c) Receptor stimulation: TSH-receptor Ab (Graves' disease) │
│ d) Receptor blockade: AChR-Ab (Myasthenia gravis) │
│ e) Immune complex deposition: Anti-dsDNA (SLE) │
│ │
│ 2. T CELL-MEDIATED DAMAGE │
│ - CD4+ Th1: Cytokines → macrophage activation │
│ → granulomatous inflammation │
│ - CD8+ CTL: Direct cytotoxicity of self cells │
│ Examples: T1DM (islet β-cell destruction) │
│ Multiple sclerosis (myelin damage) │
└─────────────────────────────────────────────────────────────────┘
TOPIC 5: NEOPLASMS IN PATIENTS WITH HIV INFECTION
AIDS-Defining Neoplasms (from Robbins Table 6.16)
The three AIDS-defining neoplasms are:
1. Kaposi Sarcoma (KS) ⭐⭐⭐
- Etiology: HHV-8 (Human Herpesvirus 8 / Kaposi sarcoma-associated herpesvirus)
- Most common AIDS-defining malignancy
- Types:
- Classic KS (elderly Eastern European men)
- Endemic KS (Africa)
- Epidemic/AIDS-related KS (most aggressive)
- Transplant-associated KS
- Morphology:
- Gross: Multiple purplish-red skin lesions (macules, plaques, nodules); also in oral mucosa, GI tract, lymph nodes, lungs
- Histology: Proliferating spindle cells (endothelial/perivascular cell origin), slit-like vascular spaces, red blood cells extravasating into spaces, chronic inflammatory infiltrate
- CD4 count: Can occur even at >200 cells/μL, but more aggressive at lower counts
2. Non-Hodgkin Lymphoma (NHL) - Primary CNS Lymphoma ⭐⭐
- Etiology: EBV-associated
- Primary CNS lymphoma is AIDS-defining
- Also peripheral high-grade B-cell NHL (Burkitt's lymphoma)
- Histology: Large B-cell lymphoma with EBV-positive cells; CNS involvement
- CD4 count: Usually <50 cells/μL for CNS lymphoma
3. Invasive Cancer of the Uterine Cervix ⭐
- Etiology: HPV (Human Papillomavirus) - high-risk types 16, 18
- Loss of cell-mediated immunity → HPV persists → cervical dysplasia → invasive carcinoma
- Regular Pap smears mandatory in HIV-positive women
Other Malignancies Seen in HIV (Not Strictly AIDS-defining but High Yield)
| Malignancy | Association |
|---|---|
| Hodgkin Lymphoma | EBV-related; increased incidence in HIV |
| Anal carcinoma | HPV 16/18 |
| Hepatocellular carcinoma | Hepatitis B/C co-infection |
| Lung cancer | Increased risk (smoking + immunosuppression) |
| Burkitt's lymphoma | EBV; c-MYC translocation |
TOPIC 6: AIDS - ETIOLOGY, ROUTES OF TRANSMISSION, NATURAL HISTORY, DIAGNOSIS
Definition
AIDS (Acquired Immunodeficiency Syndrome) is the end-stage of HIV infection, defined by the CDC as:
- CD4+ T cell count < 200 cells/μL OR
- CD4+ T cell percentage < 14% of total lymphocytes OR
- Presence of an AIDS-defining condition (opportunistic infection or malignancy)
Etiology
┌─────────────────────────────────────────────────────────────────┐
│ HIV - ETIOLOGY │
│ │
│ Virus: Human Immunodeficiency Virus (HIV) │
│ Family: RETROVIRIDAE │
│ Genus: LENTIVIRUS │
│ │
│ Two Types: │
│ HIV-1: Major global pandemic type (more virulent) │
│ HIV-2: Mainly West Africa; less virulent; slower progression │
│ │
│ STRUCTURE (important for exam): │
│ ┌──────────────────────────────────────┐ │
│ │ Envelope (gp120 + gp41) │ │
│ │ → gp120: binds CD4 receptor │ │
│ │ → gp41: fusion with host cell │ │
│ │ Matrix protein: p17 │ │
│ │ Core (capsid): p24 [marker!] │ │
│ │ Genome: 2 copies ssRNA (diploid) │ │
│ │ Enzymes: Reverse transcriptase (RT) │ │
│ │ Integrase │ │
│ │ Protease │ │
│ └──────────────────────────────────────┘ │
│ │
│ HIV infects: CD4+ T cells (PRIMARY TARGET), macrophages, │
│ dendritic cells, microglia (CNS) │
│ Coreceptors: CCR5 (early - macrophage tropic R5 strain) │
│ CXCR4 (late - T-tropic X4 strain) │
└─────────────────────────────────────────────────────────────────┘
Routes of Transmission
┌──────────────────────────────────────────────────────────────────┐
│ ROUTES OF HIV TRANSMISSION │
│ │
│ 1. SEXUAL TRANSMISSION (Most common worldwide - 75-85%) │
│ - Heterosexual (most common in Africa/Asia) │
│ - Homosexual/MSM (most common in developed countries) │
│ - Receptive partner at higher risk │
│ - STIs (ulcerative) increase transmission risk │
│ │
│ 2. PARENTERAL (Blood-borne) │
│ - IV drug users sharing needles │
│ - Blood transfusion (now rare with screening) │
│ - Needle-stick injuries in healthcare workers │
│ (risk ~0.3% per exposure) │
│ - Clotting factor concentrates (hemophiliacs - pre-screening)│
│ │
│ 3. VERTICAL (Mother to Child) │
│ - Transplacental (antepartum) - 30-40% │
│ - Intrapartum (most common): during delivery - 50-60% │
│ - Breast feeding (postpartum) - 10-20% │
│ - PMTCT (prevention): ART during pregnancy │
│ │
│ NOT transmitted by: casual contact, saliva, tears, │
│ air-borne, insect vectors, food/water │
└──────────────────────────────────────────────────────────────────┘
Natural History / Phases of HIV Infection
╔══════════════════════════════════════════════════════════════════╗
║ NATURAL HISTORY OF HIV INFECTION ║
╠═════════════╦════════════╦════════════════════════════════════════╣
║ PHASE ║ CD4 COUNT ║ FEATURES ║
╠═════════════╬════════════╬════════════════════════════════════════╣
║ ║ ║ - Flu-like illness (2-4 wks after ║
║ PHASE 1: ║ Initially ║ exposure) ║
║ ACUTE HIV ║ drops, ║ - Fever, lymphadenopathy, pharyngitis║
║ SYNDROME ║ then rises║ - Maculopapular rash ║
║ (Acute ║ ║ - High viral load, low CD4 ║
║ Serocon- ║ >500 ║ - CD8+ T cell response controls ║
║ version) ║ ║ viremia temporarily ║
║ (2-4 wks) ║ ║ - Window period: 2-18 weeks ║
╠═════════════╬════════════╬════════════════════════════════════════╣
║ PHASE 2: ║ ║ - Clinically asymptomatic ║
║ CHRONIC ║ 200-500 ║ - Low-level viral replication ║
║ ASYMPTO- ║ (declining║ - HIV harbored in lymph nodes ║
║ MATIC ║ slowly) ║ - Duration: 7-10 years average ║
║ PHASE ║ ║ - Minor: oral thrush, herpes zoster ║
║ ║ ║ - PGL (persistent generalized ║
║ ║ ║ lymphadenopathy) ║
╠═════════════╬════════════╬════════════════════════════════════════╣
║ PHASE 3: ║ ║ - AIDS-defining conditions appear ║
║ AIDS ║ < 200 ║ - Opportunistic infections ║
║ (Final ║ (crashes) ║ - AIDS-defining neoplasms ║
║ Stage) ║ ║ - Wasting syndrome ║
║ ║ ║ - HIV encephalopathy/dementia ║
╚═════════════╩════════════╩════════════════════════════════════════╝
CD4 Count and Corresponding Complications:
| CD4 Count | Complications |
|---|---|
| > 500 | Acute HIV syndrome; PGL |
| 200-500 | TB, oral candidiasis, herpes zoster, skin infections |
| 100-200 | PCP (Pneumocystis pneumonia), toxoplasmosis, cryptosporidiosis |
| 50-100 | CMV retinitis, Cryptococcal meningitis, disseminated MAC |
| < 50 | Primary CNS lymphoma, CMV end-organ disease, disseminated MAC |
Diagnosis of HIV
┌──────────────────────────────────────────────────────────────────┐
│ DIAGNOSIS OF HIV │
│ │
│ 1. SCREENING TEST (Initial) │
│ ELISA (Enzyme-Linked Immunosorbent Assay) │
│ - Detects HIV antibodies (anti-HIV IgG/IgM) │
│ - Highly SENSITIVE (>99.5%) but less specific │
│ - Window period: 3-12 weeks (Ab seroconversion) │
│ - 4th generation ELISA: detects p24 antigen + antibodies │
│ (reduces window period) │
│ │
│ 2. CONFIRMATORY TEST │
│ WESTERN BLOT │
│ - Detects antibodies to specific HIV proteins │
│ - Positive: bands for gp41, gp120, gp160, p24, p31 │
│ - Highly SPECIFIC │
│ - Required criteria: ≥2 of gp41, gp120/gp160, p24 │
│ │
│ 3. VIROLOGICAL TESTS (Diagnosis + Monitoring) │
│ HIV RNA PCR (Viral Load) │
│ - Detects HIV RNA (viral load) │
│ - Most sensitive for early/acute infection │
│ - Used for monitoring treatment response │
│ - Guides ART initiation │
│ │
│ 4. CD4+ T CELL COUNT │
│ - Defines stage of disease │
│ - Guides prophylaxis decisions │
│ - Monitors immune reconstitution on ART │
│ │
│ 5. p24 ANTIGEN TEST │
│ - Detects p24 core antigen │
│ - Useful in window period before antibodies appear │
│ │
│ 6. RAPID HIV TESTS │
│ - Point-of-care tests, results in 20-30 minutes │
│ - Blood/oral fluid │
│ - Still require confirmatory testing if positive │
│ │
│ FOR INFANTS (<18 months) of HIV+ mothers: │
│ - Use HIV DNA PCR (not antibody tests - maternal IgG │
│ crosses placenta and gives false positives) │
└──────────────────────────────────────────────────────────────────┘
Algorithm for HIV Diagnosis (NACO/WHO):
Suspected HIV
↓
ELISA (Screening) → NEGATIVE = Not infected (if no window period)
↓ POSITIVE
Repeat ELISA (Different kit)
↓ POSITIVE
Western Blot (Confirmatory)
↓ POSITIVE
CONFIRMED HIV INFECTION
↓
CD4 count + Viral load → Staging and treatment decisions
CDC Classification of HIV (1993)
| Clinical Category | CD4 ≥500 (Cat 1) | CD4 200-499 (Cat 2) | CD4 <200 (Cat 3) |
|---|---|---|---|
| A: Asymptomatic/PGL | A1 | A2 | A3 |
| B: Symptomatic (not A or C) | B1 | B2 | B3 |
| C: AIDS-indicator conditions | C1 | C2 | C3 |
AIDS = Any Category 3 (CD4 <200) OR Any Category C condition
KEY MNEMONICS FOR EXAM
Hypersensitivity Types - "ACID":
- Anaphylactic (Type I - IgE)
- Cytotoxic (Type II - IgG/IgM)
- Immune complex (Type III)
- Delayed/DTH (Type IV - T cell)
Amyloid stains - "Congo Crystal Thioflavin":
- Congo red → Apple green birefringence (under polarized light)
- Crystal violet → Metachromasia (purple → pink/rose)
- Thioflavin T → Yellow-green fluorescence
AIDS-defining neoplasms:
- Kaposi sarcoma (HHV-8)
- Lymphoma - Primary CNS (EBV)
- Cervical carcinoma - Invasive (HPV)
HIV structure: "RT with p24 core and gp120/41 envelope"
QUICK SUMMARY TABLE FOR VIVA/EXAM
| Topic | Key Points |
|---|---|
| Type I HS | IgE-mediated; mast cells; histamine; anaphylaxis/atopy |
| Amyloid stain | Congo red → apple-green birefringence under polarized light |
| Sago spleen | Amyloid in white pulp; tapioca-like nodules |
| Lardaceous spleen | Amyloid in red pulp; homogeneous waxy enlargement |
| Autoimmunity | Failure of tolerance; genetic + environmental; HLA associations |
| AIDS neoplasms | KS (HHV-8), CNS lymphoma (EBV), cervical cancer (HPV) |
| HIV CD4 <200 | AIDS definition; PCP, CMV, lymphoma |
| HIV diagnosis | ELISA screening → Western blot confirmation → HIV RNA PCR |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed., 9780443264528); Jawetz, Melnick & Adelberg's Medical Microbiology 28E; Cellular and Molecular Immunology (Abbas, Lichtman & Pillai); supplemented with Harsh Mohan Pathology concepts. All content MUHS 2nd MBBS exam-oriented.
This is a shared conversation. Sign in to Orris to start your own chat.