White blood cells types n function with interpretation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
white blood cells types neutrophil eosinophil basophil monocyte lymphocyte
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Here is a comprehensive overview of white blood cells (WBCs/leukocytes) — their types, functions, and clinical interpretation.
White Blood Cells (Leukocytes): Types, Functions & Interpretation
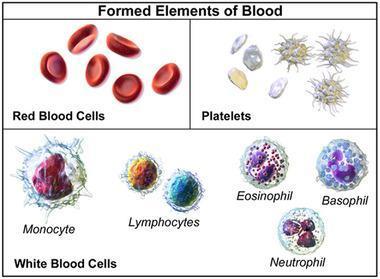
Leukocytes are the mobile units of the body's protective system. They are formed in the bone marrow (granulocytes, monocytes, some lymphocytes) and lymphoid tissue (lymphocytes, plasma cells). Normal total WBC count in an adult: 4,500–11,000 cells/µL.
Classification
WBCs are divided into two major groups based on the presence of cytoplasmic granules:
| Group | Cell Types |
|---|---|
| Granulocytes | Neutrophils, Eosinophils, Basophils |
| Agranulocytes | Monocytes, Lymphocytes |
1. Neutrophils (Polymorphonuclear Cells)
| Feature | Detail |
|---|---|
| Normal % | 50–70% (47–67%) of all leukocytes |
| Normal absolute | 1,800–7,700/µL |
| Nucleus | Multi-lobed (2–5 lobes) |
| Granules | Small, contain lysozyme, lactoferrin, myeloperoxidase, defensins |
| Life span | 4–8 hrs in blood; 4–5 days in tissue |
Functions:
- Phagocytosis — primary defense against bacteria and fungi
- Chemotaxis — migrate via diapedesis to sites of infection/inflammation
- Bactericidal killing — via oxidative burst (superoxide, H₂O₂, hypochlorite) and myeloperoxidase
- Degranulation — release proteolytic enzymes to destroy pathogens
Clinical Interpretation:
- Neutrophilia (>7,700/µL): Bacterial infections, physical/emotional stress, corticosteroids, myocardial infarction, myeloproliferative disorders
- Neutropenia (<1,800/µL): Viral infections, aplastic anemia, chemotherapy, autoimmune disease (risk of serious infection)
- Left shift (band forms ↑): Active bacterial infection, sepsis
- Hypersegmentation (>5 lobes): B₁₂/folate deficiency (megaloblastic anemia)
2. Eosinophils
| Feature | Detail |
|---|---|
| Normal % | 1–4% |
| Normal absolute | 100–400/µL |
| Nucleus | Bilobed |
| Granules | Large, red-orange on Romanowsky stain; contain MBP, ECP, EDN, EPO |
| Life span | ~18 hours in blood |
Functions:
- Anti-parasitic activity — major basic protein (MBP) and eosinophil cationic protein (ECP) are toxic to helminths and protozoa
- Modulation of hypersensitivity — dampen allergic/inflammatory reactions by inactivating histamine and SRS-A from mast cells
- Phagocytosis of antigen-antibody complexes
- Participate in allergic reactions, asthma, and some myocardial diseases
Clinical Interpretation:
- Eosinophilia (>400/µL): Allergic diseases (asthma, hay fever, drug reactions), parasitic infections (helminths), skin disorders (eczema), Hodgkin lymphoma, adrenal insufficiency
- Eosinopenia (<100/µL): Acute bacterial infection, corticosteroid therapy (adrenal hormones cause eosinophils to leave circulation)
- Charcot-Leyden crystals: Seen in eosinophilic inflammation (asthma sputum, parasitic disease)
3. Basophils
| Feature | Detail |
|---|---|
| Normal % | <0.5–1% |
| Normal absolute | 0–100/µL |
| Nucleus | Irregular, lobulated, often obscured by granules |
| Granules | Large, dark blue-purple; contain heparin, histamine, heparan sulfate, leukotrienes, ECF-A, SRS-A, PAF |
Functions:
- Immediate hypersensitivity reactions — IgE binds to surface; antigen triggers degranulation releasing histamine, SRS-A, PAF → anaphylaxis, asthma, urticaria
- Delayed hypersensitivity (cutaneous basophil hypersensitivity — contact allergies)
- Anticoagulation via heparin release
- Recruitment of eosinophils via ECF-A
Clinical Interpretation:
- Basophilia (>100/µL): Chronic myeloid leukemia (CML — a key feature), myeloproliferative disorders, hypothyroidism, allergic reactions, inflammatory bowel disease
- Basopenia: Hyperthyroidism, acute allergic reactions (degranulation), corticosteroid use
4. Monocytes
| Feature | Detail |
|---|---|
| Normal % | 3–9% |
| Normal absolute | 200–800/µL |
| Nucleus | Kidney-bean or horseshoe shaped, indented |
| Cytoplasm | Gray, ground-glass appearance, fine azurophilic granules |
| Life span | 10–20 hours in blood; months as tissue macrophages |
Functions:
- Phagocytosis — ingest bacteria, dead cells, foreign particles
- Differentiate into macrophages in tissues (Kupffer cells in liver, alveolar macrophages in lungs, microglia in brain, Langerhans cells in skin)
- Antigen presentation to T lymphocytes (adaptive immunity)
- Reticuloendothelial system — macrophages form tissue defense network
- Release cytokines (IL-1, TNF-α, IL-6) to orchestrate inflammation
Clinical Interpretation:
- Monocytosis (>800/µL): Chronic infections (TB, SBE, brucellosis), autoimmune diseases (SLE, IBD), recovery phase of acute infection, myelomonocytic leukemia
- Monocytopenia: Aplastic anemia, hairy cell leukemia, corticosteroid use
5. Lymphocytes
| Feature | Detail |
|---|---|
| Normal % | 20–40% (26–28%) |
| Normal absolute | 1,000–4,800/µL |
| Nucleus | Large, dense, round; thin rim of cytoplasm |
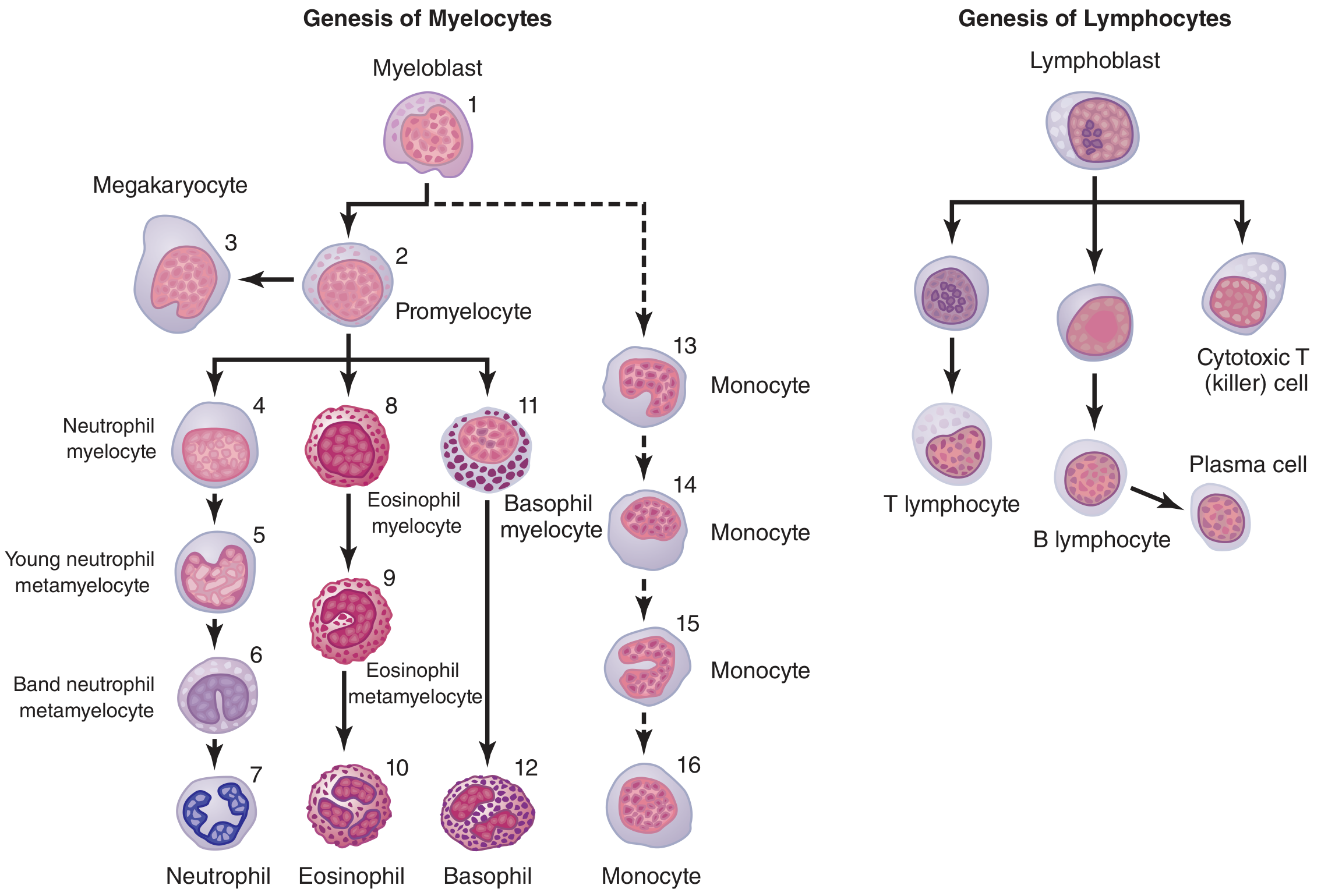
Three major subtypes:
| Subtype | Function |
|---|---|
| T lymphocytes (T cells) | Cell-mediated immunity — cytotoxic killing of virus-infected/tumor cells, helper functions (CD4⁺), regulatory suppression |
| B lymphocytes (B cells) | Humoral immunity — differentiate into plasma cells that produce antibodies (IgG, IgM, IgA, IgE, IgD) |
| NK (Natural Killer) cells | Innate immunity — kill virus-infected and cancer cells without prior sensitization |
Clinical Interpretation:
- Lymphocytosis (>4,800/µL):
- Absolute: Viral infections (EBV/mono, CMV, hepatitis, pertussis, HIV acute), chronic lymphocytic leukemia (CLL)
- Relative: Typhoid fever, brucellosis
- Atypical lymphocytes (Downey cells): Infectious mononucleosis (EBV)
- Lymphopenia (<1,000/µL): HIV/AIDS (CD4⁺ T cell depletion), corticosteroids, chemotherapy/radiation, severe combined immunodeficiency (SCID), SLE
Normal WBC Differential at a Glance
| Cell Type | % | Absolute Count (/µL) | Key Features |
|---|---|---|---|
| Neutrophils | 50–70% | 1,800–7,700 | Multilobed nucleus, first responders to bacteria |
| Eosinophils | 1–4% | 100–400 | Bilobed, red granules, anti-parasitic |
| Basophils | 0–1% | 0–100 | Dark granules, IgE-mediated allergy |
| Monocytes | 3–9% | 200–800 | Kidney-shaped nucleus, become macrophages |
| Lymphocytes | 20–40% | 1,000–4,800 | Round nucleus, adaptive immunity |
Quick Clinical Memory Aid: "Never Let Monkeys Eat Bananas"
Neutrophils → Lymphocytes → Monocytes → Eosinophils → Basophils (in order of normal relative abundance)
Key Interpretation Patterns
| Finding | Think of |
|---|---|
| ↑ Neutrophils + left shift | Acute bacterial infection, sepsis |
| ↑ Eosinophils | Allergy, parasites, Hodgkin lymphoma |
| ↑ Basophils | CML, myeloproliferative disease |
| ↑ Monocytes | TB, SBE, recovery phase |
| ↑ Lymphocytes + atypical forms | EBV (mononucleosis), viral infections |
| ↓ All WBCs (pancytopenia) | Aplastic anemia, bone marrow failure |
| ↑ WBCs in all lines | Leukemia |
Sources: Guyton and Hall Textbook of Medical Physiology; Histology: A Text and Atlas (Ross & Pawlina); Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.